OLI Psychology is not your typical course. Our goal is for you to work through the course
materials online on your own time and in the way that is most efficient given your prior
knowledge.
While you will have more flexibility than you do in a traditional course, you will also
have more responsibility for your own learning. You will need to:
- Plan how to work through each unit.
- Determine how to use the various features of the course to help you learn.
- Decide when you need to seek additional support.
What You Need to Know About Each Unit
Each unit in this course has features designed to support you as an independent learner,
including:
-
Explanatory content: This is the
informational “meat” of every unit. It consists of short passages of
text with information, images, explanations, and short videos.
-
Learn By Doing activities: Learn By
Doing activities give you the chance to practice the concept that you
are learning, with hints and feedback to guide you if you struggle.
-
Did I Get This? activities: Did I Get
This? activities are your chance to do a quick "self-check" and assess
your own understanding of the material before doing a graded activity.
Completing this course efficiently and effectively
When starting an online course, most people neglect planning, opting instead to
jump in and begin working. While this might seem efficient (after all, who wants
to spend time planning when they could be doing?), it can ultimately be
inefficient. In fact, one of the characteristics that distinguishes experts
from novices is that experts spend far more time planning their approach to a
task and less time actually completing it; while novices do the reverse: rushing
through the planning stage and spending far more time overall.
In this course, we want to help you work as efficiently and effectively as
possible, given what you already know. Some of you have already taken a
psychology course, and are already familiar with many of the concepts. You may
not need to work through all of the activities in the course; just enough to
make sure that you've "got it." For others, this is your first exposure to
psychology, and you will want to do more of the activities, since you are
learning these concepts for the first time.
Improving your planning skills as you work through the material in the course
will help you to become a more strategic and thoughtful learner and will enable
you to more effectively plan your approach to assignments, exams and projects in
other courses.
Metacognition
This idea of planning your approach to the course before you start is called
Metacognition.
- Metacognition
-
(Definition)
Metacognition, or “thinking about thinking,” refers to your
awareness of yourself as a learner and your ability to regulate your
own learning.
Metacognition involves five
distinct skills:
-
Assess the task—Get a handle on what is involved in
completing a task (the steps or components required for success) and any
constraints (time, resources).
-
Evaluate your strengths and weaknesses—Evaluate your own
skills and knowledge in relation to a task.
-
Plan an approach—Take into account your assessment of the
task and your evaluation of your own strengths and weaknesses in order to
devise an appropriate plan.
-
Apply strategies and monitor your performance—Continually
monitor your progress as you are working on a task, comparing where you are
to the goal you want to achieve.
-
Reflect and adjust if needed—Look back on what worked and
what didn't work so that you can adjust your approach next time and, if
needed, start the cycle again.
These five skills are applied over and over again in a cycle—within the
same course as well as from one course to another:
Mouse over the individual skills to learn more.
Example
Metacognition in Action
You get an assignment and ask yourself: “What exactly does this assignment involve
and what have I learned in this course that is relevant to it?”
You are exercising metacognitive skills (1) and (2) by assessing the task and
evaluating your strengths and weaknesses in relation to it.
If you think about what steps you need to take to complete the assignment and
determine when it is reasonable to begin, you are exercising skill (3) by
planning.
If you start in on your plan and realize that you are working more slowly
than you anticipated, you are putting skill (4) to work by applying a
strategy and monitoring your performance.
Finally, if you reflect on your performance in relation to your timeframe for
the task, and discover an equally effective but more efficient way to work,
you are engaged in skill (5); reflecting and adjusting your approach as
needed.
Example
Joe's Learning Strategies
Metacognition is not rocket science. In some respects, it is fairly ordinary and
intuitive. Yet you’d be surprised how often people lack strong metacognitive skills; and
you’d be amazed by how much weak metacognitive skills can undermine performance.
Learn By Doing
Now take the opportunity to practice the concepts you've been learning by doing
these two Learn By Doing activities. Read each of the scenarios below and
identify which metacognitive skill the student is struggling with. If you need
help, remember that you can ask for a hint.
You've now read through the explanatory content in this unit, and you've had a chance to
practice the concepts. Take a moment to reflect on your understanding. Do you feel like
you are "getting it"? Use these next two activities to find out.
Strong metacognitive skills are essential for independent learning, so use the experience
of monitoring your own learning in OLI Psychology as an opportunity to hone these skills
for other classes and tasks.
References
Ambrose, S. A., Bridges, M. W., DiPietro, M., Lovett, M. C., & Norman, M. K.
(2010). How learning works: 7 research-based principles for
smart teaching. San Francisco: Jossey-Bass.
Chi, M. T. H., Bassock, M., Lewis, M. W., Reimann, P., & Glaser, R. (1989).
"Self-explanations: How students study and use examples in learning to solve
problems." Cognitive Science, 13, 145-182.
Dunning, D. (2007). Self-insight: Roadblocks and detours on
the path to knowing thyself. New York: Taylor and Francis.
Hayes, J. R., & Flower, L. S. (1986). "Writing research and the writer." American Psychologist Special Issue: Psychological Science
and Education, 41, 1106-1113.
Schoenfeld, A. H (1987). "What’s all the fuss about metacognition?" In A. H.
Schoenfeld (Ed.), Cognitive science and mathematics
education. (pp.189-215). Hillsdale, NJ: Erlbaum.
This Introduction to Psychology course was developed as part of the Community College Open
Learning Initiative. Using an open textbook from Flatworld Knowledge as a foundation,
Carnegie Mellon University's Open Learning Initiative has built an online learning
environment designed to enact instruction for psychology students.
|
The Open Learning Initiative (OLI) is a grant-funded group at Carnegie Mellon University,
offering innovative online courses to anyone who wants to learn or teach. Our aim is to
create high-quality courses and contribute original research to improve learning and
transform higher education by:
- Supporting better learning and instruction with high-quality, scientifically-based,
classroom-tested online courses and materials.
- Sharing our courses and materials openly and freely so that anyone can learn.
- Developing a community of use, research, and development.
|
|
|
Flatworld Knowledge is a college
textbook publishing company on a mission. By using technology and innovative business
models to lower costs, Flatword is increasing access and personalizing learning for college
students and faculty worldwide. Text, graphics and video in this course are built on materials by
Flatworld Knowledge, made available
under a CC-BY-NC-SA
license. Interested in a companion text for this course? Flatworld provides access
to the original textbook online and makes digital and print copies of the original
textbook available at a low cost.
|
Welcome to world of psychology. This course will introduce you to
some of the most important ideas, people, and research methods from the field of
Psychology. You probably already know about some people, perhaps Sigmund Freud or B. F.
Skinner, who contributed to our understanding of human thought and behavior, and you may
have learned about important ideas, such as personality testing or methods of
psychotherapy. This course will give you the opportunity to refine and organize the
knowledge you bring to the class, and we hope that you will learn about theories,
phenomena, and research results that give you new insight into the human condition.
This first module is your opportunity to explore the field of psychology for a while before
moving into material that will be assessed and tracked. Let’s start with an obvious
question:
The word psychology is based on two words from the Greek language:
psyche, which means “life” or, in a more restricted sense
“mind,” or “spirit,” and logia, which is the source for the current
meaning, “the study of…”
Whatever the origin of the word, over the years, philosophers, scientists, and other
interested people have debated about the “proper” subject matter for psychology. Should we
focus on actual behavior, which we can observe and even measure, or on the mind, which
includes the rich inner experience we all have of the world and of our own thoughts and
motives, or on the brain, which is the centerpiece of the physical systems that make
thought and behavior possible? And psychology is not just a bunch of fancy theories.
Psychology is a vibrant, growing field because psychologists’ ideas and skills are used
every day in thousands of ways to solve real-world problems.
To start your introduction to psychology, first survey the range of topics you will be
studying in this course. The section on “What do psychologists study?” reviews the scope of
topics covered in this course and allows you to see some of the general themes the various
units develop. When you are finished with your survey of topics, the section on “What do
psychologists do?” gives you some sense of the scope of psychological work and professional
fields where psychological training is essential.
Your work in the rest of this module will also introduce you to one of the essential
features of this course: Learning by Doing. Research and experience tell us that active
involvement in learning is far more effective than mere passive reading or listening.
Learning by Doing doesn’t need to be complicated or difficult. It simply requires that you
get out of automatic mode and think a bit about the ideas you are encountering. We will get
you to participate a bit in your introduction to the online materials and to the field of
psychology, so you can Learn by Doing.
You will also encounter another type of activity: Did I Get This? These brief quizzes allow
you to determine if you are on track in your understanding of the material. Take the Did I
Get This? quiz after each section of the module. If you do well, you might decide that you
have mastered the material enough to go on. However, keep in mind that you, not the quiz,
should decide if you are ready. The quiz is just there to help you.
Before you leave a particular section of a module, you will usually have the opportunity to
check your knowledge. The activities called Did I Get This? are brief quizzes about the
material you have just been studying. Use them to monitor your understanding of the
material before moving on.
You now know that psychology is a big field and psychologists are interested in a great
variety of issues. In order to introduce you to so much material, we will often have to
focus on specific issues or problems and on an experiment or theory that addresses issue or
problem. Much of this research is conducted in university laboratories. This may give you
the impression that psychologists only work in universities, conducting experiments with
undergraduate psychology students. It is true that a lot of research takes place in
university labs, but the majority of psychologists work outside of the university
setting.
The next Learn by Doing will give you a chance to consider different ways that people with
training in psychology use their skills. In the second module of this introductory unit, we
will explore the various areas of psychology more systematically, so this is just a first
look at the scope of the work psychologists do.
learn by doing
Your task is to categorize the work of each of our seven psychologists as best
fitting basic research, mental health, or applied psychology. In the real world, a
single individual might work in two or all three of these areas, but, for the sake of
our exercise, find the best fit for the description. Answer by clicking on the
appropriate box below.
Images in this activity courtesy of Kim J, Matthews NL, Park S (CC-BY-2.5), FrozenMan (Public Domain), and Brian J. McDermott (CC-BY-2.0).
In the next module of this introductory unit you will learn a bit about the history of
psychology and some of the major issues that influence psychological thinking.
In this module we review some of the important philosophical questions that psychologists
attempt to answer, the evolution of psychology from ancient philosophy and how
psychology became a science. You will learn about the early schools (or approaches) of
psychological inquiry and some of the important contributors to each of these early
schools of psychology. You will also learn how some of these early schools influenced
the newer contemporary perspective of psychology.
The approaches that psychologists originally used to assess the issues that interested
them have changed dramatically over the history of psychology. Perhaps most importantly,
the field has moved steadily from speculation about the mind and behavior toward a more
objective and scientific approach as the technology available to study human behavior
has improved. There has also been an increasing influx of women into the field. Although
most early psychologists were men, now most psychologists, including the presidents of
the most important psychological organizations, are women.
Questions That Psychologists Ask
Although psychology has changed dramatically over its history, several questions that
psychologists address have remained constant and we will discuss them both here
and in the units and modules to come:
-
Nature versus nurture. Are genes or environment most influential in
determining the behavior of individuals and in accounting for differences
among people? Most scientists now agree that both genes and environment play
crucial roles in most human behaviors, and yet we still have much to learn
about how nature (our biological makeup) and nurture (the experiences that
we have during our lives) work together. In this course we will see that
nature and nurture interact in complex ways, making the question “Is it
nature or is it nurture?” very difficult to answer.
-
Mind versus Body.How is the mind—our thoughts, feelings, and
ideas—related to the body and brain? Are they the same, or are they
different and separate entities? The relationship between the mind and
body/brain has been debated for centuries and the early predominate belief
was that the mind and body were separate entities. This belief became known
as the mind-body dualism in which the body is physical and the mind is nonphysical, mysterious, and
somehow controls the body. Others believe that the mind and body
are not separate in that the mind is a result of activity in the brain. For
example, we know that the body can influence the mind such as when feelings
of passion or other emotions take over our better judgment. Just like the
debate of nature versus nurture, the debate of mind versus body does not
have an either-or answer; we know today that the mind and body are
intricately intertwined. Today biological psychologists are most interested
in this reciprocal relationship between biology and behavior.
-
Automatic versus controlled processing. One of the great
contributions of Sigmund Freud to psychology was his emphasis on unconscious
mental activities that influence and even control our thoughts and
behaviors. Now, in the age of neuroscience, Freud’s ideas have been
radically updated and revised. Much of our normal thinking, perceiving, and
acting occurs through brain processes that work automatically, often because
we have learned to do them so well and practiced them so much that they
occur whether or not we are aware of their occurrence. For example, as you
read these words, your visual system quickly and effortlessly translates
black lines on a white background into words that have meaning. This is
automatic processing, and you can’t avoid it. (Look at
the following word but do not read it: FORK). However, you can also process information in a
slow, analytic way, focusing attention on an object or an idea. For example,
if I ask you how many different meanings the word “bank” has, the answer
comes slowly and you probably use conscious strategies to search your mind
for possible meanings (“Hmm, the side of a river and a
place you put money. Oh, and the inward tilting movement of an airplane.
And an elevated part of the ocean floor. And...."). The study of
automatic and controlled processes is an important part of our study of
child and adolescent development, clinical conditions, and communication
through language, to name just a few areas of application.
-
Differences versus similarities. To what extent are we
all similar, and to what extent are we different? For instance, are there
basic psychological and personality differences between men and women, or
are men and women by and large similar? And what about people from different
ethnicity and cultures? Are people around the world generally the same, or
are they influenced by their backgrounds and environments in different ways?
Personality, social, and cross-cultural psychologists attempt to answer
these classic questions.
learn by doing
Directions: Read each scenario and answer the questions
about how each situation might be viewed by a psychologist.
Scenario 1: Alex and Julie, his girlfriend, are having a
discussion about aggression in men and women. Julie thinks that males are much
more aggressive than females because males have more physical fights and get
into trouble with the law than females. Alex does not agree with Julie and tells
her that even though males get into more physical fights, he thinks that females
are much more aggressive than males because females engage more in gossip,
social exclusion, and spreading of malicious rumors than men. Is Alex or Julie’s
thinking about aggression correct?
Scenario 2: Your genetics give you certain physical traits
and cognitive capabilities. You are great at math but may never be an artist.
Sometimes in life, we have to accept the traits and abilities that have been
given to us, even though you may wish you were different.
Scenario 3: Raul is having a discussion with his mother
about his father, Tomas, and his brother, Hector. Tomas, the father, is an
alcoholic and Raul expresses to his mother that he is concerned about his
brother, Hector, who is also beginning to drink a lot. Raul does not want his
brother to turn out like his father. Raul’s mother tells him that there have
been several men in the family who are alcoholics such as his grandfather and
two uncles. She says that it runs in the family and that his brother, Hector,
can’t help himself and he will also be an alcoholic. Raul responds that he
thinks they could stop drinking if they wanted too, despite the history of
alcoholism in the family. “After all, look at me. I don’t drink and my friends
don’t either. I don’t think I will become an alcoholic because I have friends
who know how to control themselves."
The earliest psychologists that we know about are the Greek philosophers Plato
(428–347 BC) and Aristotle (384–322 BC). These philosophers asked many of the same
questions that today’s psychologists ask; for instance, they questioned the
distinction between nature and nurture and mind and body. For example, Plato argued
on the nature side, believing that certain kinds of knowledge are innate or inborn,
whereas Aristotle was more on the nurture side, believing that each child is born as
an “empty slate” (in Latin a tabula
rasa) and that knowledge is primarily acquired through sensory learning
and experiences.
European philosophers continued to ask these fundamental questions during the
Renaissance. For instance, the French philosopher, René Descartes (1596–1650)
influenced the belief that the mind (the mental aspects of life) and body (the
physical aspects of life) were separate entities. He argued that the mind controls
the body through the pineal gland in the brain (an idea that made some sense at the
time but was later proved incorrect). This relationship between the mind and body is
known as the mind-body dualism in which the mind is fundamentally different from the
mechanical body, so much so that we have free will to choose the behaviors that we
engage in. Descartes also believed in the existence of innate natural abilities
(nature).
Another European philosopher, Englishman John Lock (1632–1704), is known for his
viewpoint of empiricism, the belief that the
newborn’s mind is a “blank slate” and that the accumulation of experiences mold
the person into who he or she becomes.
The fundamental problem that these philosophers faced was that they had few methods
for collecting data and testing their ideas. Most philosophers didn’t conduct any
research on these questions, because they didn’t yet know how to do it and they
weren’t sure it was even possible to objectively study human experience. Philosophers
began to argue for the experimental study of human behavior.
Gradually in the mid-1800s, the scientific field of psychology gained its
independence from philosophy when researchers developed laboratories to examine and
test human sensations and perceptions using scientific methods. The first two
prominent research psychologists were the German psychologist Wilhelm Wundt
(1832–1920), who developed the first psychology laboratory in Leipzig, Germany in
1879, and the American psychologist William James (1842–1910), who founded an
American psychology laboratory at Harvard University.
| The Early Schools of Psychology: No Longer Active |
|---|
| From Flat World Knowledge: Adapted from Introduction to Psychology, v1.0. CC-BY-NC-SA. |
| School of Psychology |
Description |
Earliest Period |
Historically Important People |
| Structuralism |
Uses the method of introspection to identify the basic elements of "structure" of
psychological experiences. |
Late 19th Century |
Wilhelm Wundt, Edward B. Titchener |
| Functionalism |
Inspired by Darwin's work in biology. Attempted to explain behavior, emotion, and
thought as active adaptations to environmental pressures. These ideas influenced
later behaviorism and evolutionary psychology. |
Late 19th Century |
William James, John Dewey |
|
| Early Schools of Psychology: Still Active and Advanced Beyond Early Ideas |
|---|
| From Flat World Knowledge: Adapted from Introduction to Psychology, v1.0. CC-BY-NC-SA. |
| School of Psychology |
Description |
Earliest Period |
Historically Important People |
| Psychodynamic Psychology |
Focuses on the role of our unconscious thoughts, feelings, and memories and our
early childhood experiences in determining behavior. Modern psychodynamic psychology
has built on Freud's original ideas, and it has also influenced modern
neuroscience. |
Very late 19th to Early 20th Century |
Sigmund Freud, Erik Erikson |
| Behaviorism |
Based on the premise that it is not possible to objectively study the mind.
Therefore, psychologists should limit their attention to the study of behavior
itself. Contemporary behaviorism is an active field increasingly integrated with
cognitive-neuroscience. |
Early 20th Century |
Ivan Pavlov, John B. Watson, B. F. Skinner |
| Cognitive Development |
Studies the growth of thought and language processes in infants and children.
Emphasizes the idea that children are not incompetent adults but think creatively and
effectively based on their limited experience in the world. Modern cognitive
psychology owes a great deal to these early cognitive development researchers. |
1920s |
Jean Piaget, Lee Vygotsky |
| Humanistic Psychology |
Emphasizes the development of a healthy, effectively functioning person. Rejects the
idea that clinical psychology and other applied areas should focus only on disorders
and problems. This school developed ideas of self-actualization, personal
responsibility, and human potential. Contemporary positive psychology has been
strongly influence by humanistic psychology. |
1950s |
Abraham Maslow, Carl Rogers |
|
Stucturalism: The Influence of Chemistry and Measurement
Wundt’s research in his laboratory in Liepzig focused on the nature of consciousness
itself. Wundt and his students believed that it was possible to analyze the basic
elements of the mind and to classify our conscious experiences scientifically. This
focus developed into the field known as structuralism, a school of psychology whose goal was to identify the basic
elements or “structures” of psychological experience. Its goal was to create
a “periodic table” of the “elements of sensations,” similar to the periodic table of
elements that had recently been created in chemistry.
Structuralists used the method of introspection in an attempt to create a map of the
elements of consciousness. Introspection involves asking research participants to describe exactly what they
experience as they work on mental tasks, such as viewing colors, reading a
page in a book, or performing a math problem. A participant who is reading a book
might report, for instance, that he saw some black and colored straight and curved
marks on a white background. In other studies the structuralists used newly invented
reaction time instruments to systematically assess not only what the participants
were thinking but how long it took them to do so. Wundt discovered that it took
people longer to report what sound they had just heard than to simply respond that
they had heard the sound. These studies marked the first time researchers realized
that there is a difference between the sensation of a
stimulus and the perception of that stimulus, and the idea of
using reaction times to study mental events has now become a mainstay of cognitive
psychology.
Perhaps the best known of the structuralists was Edward Bradford Titchener
(1867–1927). Titchener was a student of Wundt who came to the United States in the
late 1800s and founded a laboratory at Cornell University. In his research using
introspection, Titchener and his students claimed to have identified more than 40,000
sensations, including those relating to vision, hearing, and taste.
An important aspect of the structuralist approach was that it was rigorous and
scientific. The research marked the beginning of psychology as a science, because it
demonstrated that mental events could be quantified. But the structuralists also
discovered the limitations of introspection. Even highly trained research
participants were often unable to report on their subjective experiences. When the
participants were asked to do simple math problems, they could easily do them, but
they could not easily answer how they did them. Thus the
structuralists were the first to realize the importance of unconscious processes—that
many important aspects of human psychology occur outside our conscious awareness and
that psychologists cannot expect research participants to be able to accurately
report on all of their experiences. Introspection was eventually abandoned because it
was not a reliable method for understanding psychological processes.
Functionalism: The Influence of Biology
In contrast to structuralism, which attempted to understand the nature of
consciousness, the goal of William James and the other members of the school of functionalism was to understand why animals
and humans have developed the particular psychological aspects that they currently
possess. For James, one’s thinking was relevant only to one’s behavior. As he
put it in his psychology textbook, “My thinking is first and last and always for the
sake of my doing.”
James and the other members of the functionalist school were influenced by Charles
Darwin’s (1809–1882) theory of natural selection, which
proposed that the physical characteristics of animals and humans
evolved because they were useful, or functional. The functionalists believed
that Darwin’s theory applied to psychological characteristics too. Just as some
animals have developed strong muscles to allow them to run fast, the human brain, so
functionalists thought, must have adapted to serve a particular function in human
experience.
Although functionalism no longer exists as a school of psychology, its basic
principles have been absorbed into psychology and continue to influence it in many
ways. The work of the functionalists has developed into the field of evolutionary psychology, a contemporary perspective of
psychology that applies the Darwinian theory of natural selection to human and
animal behavior. You learn more about the perspective of evolutionary
psychology in the next section of this module.
Psychodynamics: The Foundation of Clinical Psychology
Perhaps the school of psychology that is most familiar to the general public is the
psychodynamic approach to understanding behavior, which was championed by Sigmund
Freud (1856–1939) and his followers. Psychodynamic psychology
is an approach to understanding human behavior that focuses on the
role of unconscious thoughts, feelings, and memories. Freud developed his
theories about behavior through extensive analysis of the patients that he treated in
his private clinical practice. Freud believed that many of the problems that his
patients experienced, including anxiety, depression, and sexual dysfunction, were the
result of the effects of painful childhood experiences that the person could no
longer remember.
Freud’s ideas were extended by other psychologists whom he influenced including Erik
Erikson (1902–1994). These and others who follow the psychodynamic approach believe
that it is possible to help the patient if the unconscious drives can be remembered,
particularly through a deep and thorough exploration of the person’s early sexual
experiences and current sexual desires. These explorations are revealed through talk
therapy and dream analysis, in a process called psychoanalysis.
The founders of the school of psychodynamics were primarily practitioners who worked
with individuals to help them understand and confront their psychological symptoms.
Although they did not conduct much research on their ideas, and although later, more
sophisticated tests of their theories have not always supported their proposals,
psychodynamics has nevertheless had substantial impact on the perspective of clinical
psychology and, indeed, on thinking about human behavior more generally. The
importance of the unconscious in human behavior, the idea that early childhood
experiences are critical, and the concept of therapy as a way of improving human
lives are all ideas that are derived from the psychodynamic approach and that remain
central to psychology.
Behaviorism: How We Learn
Although they differed in approach, both structuralism and functionalism were
essentially studies of the mind. The psychologists associated with the school of
behaviorism, on the other hand, were reacting in part to the difficulties
psychologists encountered when they tried to use introspection to understand
behavior. Behaviorism is a school of
psychology that is based on the premise that it is not possible to objectively
study the mind, and therefore that psychologists should limit their attention to
the study of behavior itself. Behaviorists believe that the human mind is a
“black box” into which stimuli are sent and from which responses are received. They
argue that there is no point in trying to determine what happens in the box because
we can successfully predict behavior without knowing what happens inside the mind.
Furthermore, behaviorists believe that it is possible to develop laws of learning
that can explain all behaviors.
The first behaviorist was the American psychologist John B. Watson (1878–1958).
Watson was influenced in large part by the work of the Russian physiologist Ivan
Pavlov (1849–1936), who had discovered that dogs would salivate at the sound of a
tone that had previously been associated with the presentation of food. Watson and
other behaviorists began to use these ideas to explain how events that people and
animals experienced in their environment (stimuli) could
produce specific behaviors (responses). For instance, in
Pavlov’s research the stimulus (either the food or, after learning, the tone) would
produce the response of salivation in the dogs.
In his research Watson found that systematically exposing a child to fearful stimuli
in the presence of objects that did not themselves elicit fear could lead the child
to respond with a fearful behavior to the presence of the stimulus. In the best known
of his studies, an 8-month-old boy named Little Albert was used as the subject. Here
is a summary of the findings:
The baby was placed in the middle of a room; a white laboratory rat was placed near
him and he was allowed to play with it. The child showed no fear of the rat. In later
trials, the researchers made a loud sound behind Albert’s back by striking a steel
bar with a hammer whenever the baby touched the rat. The child cried when he heard
the noise. After several such pairings of the two stimuli, the child was again shown
the rat. Now, however, he cried and tried to move away from the rat. In line with the
behaviorist approach, Little Albert had learned to associate the white rat with the
loud noise, resulting in crying.
The most famous behaviorist was Burrhus Frederick (B. F.) Skinner (1904–1990), who
expanded the principles of behaviorism and also brought them to the attention of the
public at large. Skinner used the ideas of stimulus and response, along with the
application of rewards or reinforcements, to train pigeons
and other animals. He used the general principles of behaviorism to develop theories
about how best to teach children and how to create societies that were peaceful and
productive. Skinner even developed a method for studying thoughts and feelings using
the behaviorist approach.
The behaviorists made substantial contributions to psychology by identifying the
principles of learning. Although the behaviorists were
incorrect in their beliefs that it was not possible to measure thoughts and feelings,
their ideas provided new ideas that helped further our understanding regarding the
nature-nurture and mind-body debates. The ideas of behaviorism are fundamental to
psychology and have been developed to help us better understand the role of prior
experiences in a variety of areas of psychology.
Cognitive Development: The Brain and How it Thinks
During the first half of the twentieth century, evidence emerged that learning was
not as simple as it was described by the behaviorists. Several psychologists studied
how people think, learn and remember. And this approach became known as cognitive psychology, a field of psychology
that studies mental processes, including perception, thinking, memory, and
judgment. The German psychologist Hermann Ebbinghaus (1850–1909) showed how
memory could be studied and understood using basic scientific principles. The English
psychologist Frederick Bartlett also looked at memory but focused more on how our
memories can be distorted by our beliefs and expectations.
The two individuals from this time who arguably made the strongest impact on
contemporary cognitive psychology were two great students of child development: the
Swiss psychologist Jean Piaget (1896–1980) and the Russian psychologist Lev Vygotsky
(1896–1934).
Jean Piaget was a prolific writer, a brilliant systematizer, and a creative observer
of children. Using interviews and situations he contrived, he studied the thinking
and reasoning of children from their earliest days into adolescence. He is best known
for his theory that tracks the development of children’s thinking into a series of
four major stages, each with several substages. Within each stage, Piaget pointed to
behaviors and responses to questions that revealed how the developing child
understands the world. One of Piaget’s critical insights was that children are not
deficient adults, so when they do something or make a judgement that, in an adult,
might seem to be a mistake, we should not assume that it is a mistake from the
child’s perspective. Instead, the child may be using the knowledge and reasoning that
are completely appropriate at his or her particular age to make sense of the world.
For example, Piaget found that children often believe that other people know or can
see whatever they know or can see. So, if you show a young child a scene containing
several dolls, where a particular doll is visible to the child but blocked from your
view by a dollhouse, the child will simply assume that you can see the blocked doll.
Why? Because he or she can see it. Piaget called this thinking egocentrism, by which he meant that the child’s thinking
is centered in his or her own view of the world (not that the child is
selfish). If an adult made this error, we would find it odd. But it is quite
natural for the child, because prior to about 4 years of age, children do not
understand that different minds (theirs and yours) can know different things.
Egocentric thinking is normal and healthy for a two year old (though not for a
20-year-old).
During the same years that Piaget was interviewing children and trying to chart the
course of development, Russian psychologist Lev Vygotsky was struck by the rich
social influences that influenced and even guided cognitive development. Like Piaget,
Vygotsky observed children playing with one another, and he saw how children guide
each other to learn social rules and, through those, to improve self-regulation of
behavior and thoughts.
Vygotsky’s best known contribution was his analysis of the interactions of children
and parents that lead to the development of more and more sophisticated thinking. He
suggested that the effective parent or teacher is one who helps
the child reach beyond his or her current level of thinking by creating
supports, which Vygotsky’s followers called scaffolding. For example, if a teacher wants the child to learn the difference
between a square and a triangle, she might allow the child to play with cardboard
cutouts of the shapes, and help the child count the number of sides and angles on
each. This assisted exploration is a scaffold—a set of supports for the child who is
actively doing something—that can help the child do things and explore in ways that
would not be likely or even possible alone.
Both Piaget and Vygotsky emphasized the mental development of the child and gave
later psychologists a rich set of theoretical ideas as well as observable phenomena
to serve as a foundation for the science of the mind that blossomed in the middle and
late 20th century and is the core of 21st century psychology.
Humanistic Psychology: A New Approach
By the 1950s, a clear contrast existed between psychologists who favored
behaviorism which focused exclusively on behavior that is shaped by the
environment and those who favored psychodynamic psychology which focused on
mental unconscious processes to explain behavior. Many of the psychodynamic
therapists became disillusioned with the results of their therapy and began to
propose new ways of thinking about behavior in that unlike animals, human
behavior was not innately uncivilized as Freud, James and Skinner believed.
Humanism developed on the beliefs that humans are inherently good, have free
will to make decisions, and are motivated to seek and improve themselves to
their highest potential. Instead of focusing on what went wrong with people’s
lives as did the psychodynamic psychologists, humanists asked interesting
questions about what made a person “good.” Thus, a new approach to psychology
emerged called humanism, an early school of psychology
which emphasized that each person is inherently good and
motivated to learn and improve to become a healthy, effectively functioning
individual. Abraham Maslow and Carl Rogers are credited for developing
the humanistic approach in which they asked questions about what made a person
good.
Abraham Maslow (1908–1970) developed the theory of self-motivation in which we all
have a basic, broad need to develop our special unique human
potential, which he called the drive for self-actualization. He proposed that, in order for us to achieve
self-actualization, several basic needs beginning with physiological needs of
hunger, thirst, and maintenance of other internal states of the body must first
be met. As the lower-level needs are satisfied, our internal motivation strives
to achieve higher-ordered needs such as safety, belonging and love needs and
self-esteem needs until we ultimately achieve self-actualization. Maslow’s
theory of hierarchy of needs represents our internal motivation to strive for
self-actualization. Achieving self-actualization meant that one has
achieved their unique and special human potential to be able to lead a positive
and fulfilling life.
Carl Rogers (1902–1987), originally a psychodynamic therapist, developed a new
therapy approach which he called client-centered therapy. This therapy approach
viewed the person, not as a patient, but rather as a client with more equal
status with the therapist. He believed that the client as well as every person
should be respected and valued for his or her unique and special abilities and
potential, and that the person had the ability to make conscious decisions and
free will to achieve one’s highest potential.
While the humanistic school of psychology has been criticized for its lack of
rigorous experimental investigation as being more of a philosophical approach, it has
influenced current thinking on personality theories and psychotherapy methods.
Furthermore, the foundations of the early school of humanism evolved into the
contemporary perspective of positive psychology, the scientific
study of optimal human functioning.
learn by doing
Psychologist Abraham Maslow introduced the concept of a hierarchy of needs,
which suggests that people are motivated to fulfill basic needs before moving
on to other, more advanced needs. Consider how this may influence our
development, motivation, and accomplishments. Choose which level of needs would
best explain the scenario below.
As you may have noticed in the six early schools of psychology, each attempted to answer
psychological questions with a single approach. While some attempted to build a big theory
around their approach (and some did not even attempt), no one school was successful. By the
mid-20th century, the field of psychology was still a very young science, but it was
gaining a lot of diverse attention and popularity. Psychologists began to study mental
processes and behavior from their own specific points of interests and views. Thus, some of
the specific viewpoints became known as perspectives from which to
investigate a specific psychological topic.
Today, contemporary psychology reflects several major perspectives such
biological/neuroscience, cognitive, behavioral, social, developmental, clinical, and
individual differences/personality. These are not a complete list of perspectives and your
instructor may introduce others. What’s important to know is that today all psychologists
believe that there is no one specific perspective with which to study psychology, but
rather any given topic can be approached from a variety of perspectives. For example,
investigating how an infant learns language can be studied from all of the different
perspectives that could provide information from a different viewpoint about the child’s
learning. Also as perspectives become more specific, we see that the perspectives are
interconnected with each other, meaning that it is difficult to study any topic on human
thought or behavior from just one perspective without considering the complex influence of
information from other perspectives.
| Contemporary Perspectives of Psychology |
|---|
| Perspective |
Major Emphasis |
Examples of Research Questions |
| Behavioral Neuroscience |
Genetics and the links among brain, mind, and behavior |
What brain structures influence behavior? If a brain function is altered, how is
behavior affected. To what extent do genes influence behavior when the environment is
manipulated? |
| Biological |
Relationship between bodily systems and chemicals and how they influence behavior
and thought |
How do hormones and neurotransmitters affect thought and behavior? |
| Cognitive |
Thinking, decision-making, problem-solving, memory, language, and information
processing |
What are the processes for developing language, memory, decision-making, and
problem-solving? How does thinking affect behavior? What is intelligence, and how is
it determined? What affects intelligence, memory, language, and information
processing? |
| Social |
Concepts of self and social interaction and how they differ across cultures and
shape behavior |
How do social stresses affect self-concept? How do social conditions contribute to
destructive behavior? How are behaviors affected by cultural differences? |
| Developmental |
How and why people change or remain the same over time from conception to death |
How does a person’s development from conception to death change or stay the same in
the biosocial, cognitive and psychosocial domains? What changes are universal or
unique to a person? Which periods of life are critical or sensitive for certain
development? |
| Clinical |
Diagnosis and treatment of mental, emotional, and behavioral disorders and promotion
of psychological health |
What are the cognitive and behavioral characteristics and symptoms of a mental or
behavioral abnormality? What treatment methods are most effective for the various
emotional and behavioral disorders? |
| Individual Differences/ Personality |
Uniqueness and differences of people and the consistencies in behavior across time
and situations. |
What determines personality? How does personality change or remain the same as one
ages or experiences social or environmental situations? |
|
Behavioral Neuroscience
Behavioral neuroscience studies the links among the brain, mind, and behavior. This
perspective used to be called psychobiological psychology, which studied the
biological roots such as brain structure and brain activity of behavior. But due to
the advancements in our ability to view the intricate workings of the brain, called
neuroimaging, the name behavioral neuroscience is now used for this broad discipline.
Neuroimaging is the use of various
techniques to provide pictures of the structures and functions of the living
brain. And as you read about the following contemporary psychological
perspectives, you will see how interconnected these perspectives are, largely due to
neuroimaging techniques.
For example, neuroimaging techniques are used to study brain functions in learning,
emotions, social behavior and mental illness which each have their own specialty
perspective (see the descriptions of these perspectives below). Also the two
perspectives of behavioral neuroscience and biological psychology are closely
interconnected in that the uses of neuroimaging techniques such as electrical brain
recordings enable biological psychologists to study the structure and functions of
the brain. Another example is the study of behavioral genetics which is the study of
how genes influence cognition, physical development and behavior.
Another related perspective is evolutionary psychology, which
supports the idea that the brain and body are products of
evolution and that inheritance plays an important role in shaping thought and
behavior. This perspective developed from the functionalists’ basic
assumption that many human psychological systems, including memory, emotion and
personality, serve key adaptive functions called fitness characteristics.
Evolutionary psychologists theorize that fitness characteristics have helped humans
to survive and reproduce throughout the centuries at a higher rate than do other
species who do not have the same fitness characteristics. Fitter organisms pass on
their genes more successfully to later generations, making the characteristics that
produce fitness more likely to become part of the organism’s nature than
characteristics that do not produce fitness. For example, evolutionary theory
attempts to explain many different behaviors including romantic attraction, jealousy,
stereotypes and prejudice, and psychological disorders. The evolutionary perspective
is important to psychology because it provides logical explanations for why we have
many psychological characteristics.
Biological Psychology
Closely related to behavioral neuroscience, the perspective of biological psychology
focuses on studying the connections between bodily systems such as the nervous and
endocrine systems and chemicals such as hormones and their relationships to behavior
and thought. Biological research on the chemicals produced in the body and brain have
helped psychologists to better understand psychological disorders such as depression
and anxiety and the effects of stress on hormones and behavior.
Cognitive Psychology
Cognitive psychology is the study of how we think, process information and solve
problems, how we learn and remember, and how we acquire and use language. Cognitive
psychology is interconnected with other perspectives that study language, problem
solving, memory, intelligence, education, human development, social psychology, and
clinical psychology.
Starting in the 1950s, psychologists developed a rich and technically complex set of
ideas to understand human thought processes, initially inspired by the same insights
and advances in information technology that produced the computer, cell phone and
internet. As technology advanced, so did cognitive psychology. We are now able to see
the brain in action using neuroimaging techniques. These images are used to diagnose
brain disease and injury, but they also allow researchers to view information
processing as it occurs in the brain, because the processing causes the involved area
of the brain to increase metabolism and show up on the scan such as the functional
magnetic resonance imaging (fMRI). We discuss the use of neuroimaging techniques in
many areas of psychology in the units to follow.
Social Psychology
The field of social psychology is the study of how social
situations and cultures in which people live influence their thinking, feelings and
behavior. Social psychologists are particularly concerned with how people perceive
themselves and others, and how people influence each other’s behavior. For instance,
social psychologists have found that we are attracted to others who are similar to us
in terms of attitudes and interests. We develop our own beliefs and attitudes by
comparing our opinions to those of others and we frequently change our beliefs and
behaviors to be similar to people we care about.
Social psychologists are also interested in how our beliefs, attitudes and behaviors
are influenced by our culture. Cultures influence every aspect of our lives. For
example, fundamental differences in thinking, feeling and behaving exist among people
of Western cultures (such as the United States, Canada, Western Europe, Australia,
and New Zealand) and East Asian cultures (such as China, Japan, Taiwan, Korea, India,
and Southeast Asia). Western cultures are primarily oriented toward individualism, which is about valuing the self and one’s
independence from others, sometimes at the expense of others. The East Asian
culture, on the other hand, is oriented toward interdependence, or collectivism, which focuses on developing harmonious
social relationships with others, group togetherness and connectedness, and duty
and responsibility to one’s family and other groups.
As our world becomes more global, sociocultural research will become more interconnected
with the research of other psychological perspectives such as biological, cognitive,
personality, developmental and clinical.
Developmental Psychology
Developmental psychology is the study of the
development of a human being from conception until death. This perspective
emphasizes all of the transformations and consistencies of human life. Three major
domains or aspects of human life, cognitive, physical and socioemotional, are
researched as one ages. The cognitive domain refers to all of the mental processes
that a person uses to obtain knowledge or think about the environment. The physical
domain refers to all the growth and changes that occur in a person’s body and the
genetic, nutritional, and health factors that affect that growth and change. And the
socioemotional development includes development of emotions, temperament, and social
skills. Developmentalists study how individuals change or remain the same over time
in each of these three domains. It is easy to see how the perspective of
developmental psychology is interconnected with all of the other major contemporary
perspectives because of the overlapping and all encompassing aspects of the
developmental perspective.
Clinical psychology
Clinical psychology focuses on the diagnosis and treatment of mental, emotional and
behavioral disorders and ways to promote psychological health. This field evolved from the
early psychodynamic and humanistic schools of psychology. While the clinical psychology
perspective emphasizes treating individuals so that they may lead fulfilling and productive
lives, clinical psychologists also conduct research to discover the origins of mental and
behavioral disorders and effective treatment methods. The clinical psychology perspective
is closely interconnected to behavioral neuroscience and biological psychology.
Individual differences: Personality
Personality psychology is the study of the differences and uniqueness of people and the
influences on a person’s personality. Researchers in this field study whether personality
traits change as we age or stay the same, something that developmental psychologists also
study. Researchers interested in personality also study how environmental influences such
as traumatic events affect personality.
learn by doing
Instructions: Imagine that you are a psychologist and you want
to investigate specific behaviors of a person with Alzheimer’s disease. You have a
team of psychologists who represent several contemporary perspectives in psychology
to help you explore information as to the origin, symptoms, prevalence, influences
and causes of this brain disease and the impact on family members who care for a
relative with Alzheimer’s disease. Read the following scenario about a person who had
Alzheimer’s disease.
Alzheimer’s disease (AD), the most common type of dementia, is a
steady and gradual progressive brain disorder that damages and destroys brain
cells. Eventually Alzheimer’s disease progresses to the point where the person
requires full nursing care. Ronald Reagan, who was president of the United States
from 1981 to 1989, announced in 1994 that he had Alzheimer’s disease. He died 10
years later at age 93. Despite extensive research, psychologists still have many
questions to be researched about this fatal disease.
Read each set of questions. While some of these sets of questions could be researched
by different psychological perspectives, try to determine which psychological
perspective would most likely want to provide answers for
each set of questions. Your team of psychologists represents the following
perspectives and only one perspective is the correct answer for each set of
questions.
Challenge Questions
As you can see, psychologists from all different contemporary perspectives can
contribute to the scientific knowledge of Alzheimer’s disease, and for that matter,
any kind of research pertaining to humans and animals.
Psychology is not one discipline but rather a collection of many subdisciplines that all
share at least some common perspectives that work together to exchange knowledge to form a
coherent discipline. Because the field of psychology is so broad, students may wonder which
areas are most suitable for their interests and which types of careers might be available
to them. The following figure will help you consider the answers to these questions. Click
on any of the labeled, blue circles to learn more about each discipline.
Photo courtesy of longislandwins (CC-BY-2.0).
learn by doing
You can learn more about these different subdisciplines of psychology and the careers
associated with them by visiting the American Psychological Association (APA)
website.
Step 1: Go to the APA
website.
On this APA Home webpage, notice the various types of information.
Step 2: Find the box titled “Quick Links” on the APA
Homepage.
Click on the link titled Divisions.
Step 3: On the APA site, search for the topic “Undergraduate
Education.” Find the “Psychology as a Career” webpage to learn about what employers
need from an employee, and then answer the following questions.
Now search for the topic “Careers in Psychology” on the APA website. Here you can
read interesting information about the field of psychology. This section provides a
long list of subfields in psychology that psychologists specialize in. Read about
some of the interesting job tasks that psychologists perform in some of the
subfields, and then complete the following statements by identifying the subfield
that corresponds with it job tasks.
Psychologists aren’t the only people who seek to understand human behavior and solve
social problems. Philosophers, religious leaders, and politicians, among others, also
strive to provide explanations for human behavior. But psychologists believe that
research is the best tool for understanding human beings and their relationships with
others. Rather than accepting the claim of a philosopher that people do (or do not) have
free will, a psychologist would collect data to empirically test whether or not people
are able to actively control their own behavior. Rather than accepting a politician’s
contention that creating (or abandoning) a new center for mental health will improve the
lives of individuals in the inner city, a psychologist would empirically assess the
effects of receiving mental health treatment on the quality of life of the recipients.
The statements made by psychologists are based on an empirical study. An empirical study
is results of verifiable evidence from a systematic collection and
analysis of data that has been objectively observed, measured, and undergone
experimentation.
In this unit you will learn how psychologists develop and test their research ideas; how
they measure the thoughts, feelings, and behavior of individuals; and how they analyze
and interpret the data they collect. To really understand psychology, you must also
understand how and why the research you are reading about was conducted and what the
collected data mean. Learning about the principles and practices of psychological
research will allow you to critically read, interpret, and evaluate research.
In addition to helping you learn the material in this course, the ability to interpret
and conduct research is also useful in many of the careers that you might choose. For
instance, advertising and marketing researchers study how to make advertising more
effective, health and medical researchers study the impact of behaviors such as drug use
and smoking on illness, and computer scientists study how people interact with
computers. Furthermore, even if you are not planning a career as a researcher, jobs in
almost any area of social, medical, or mental health science require that a worker be
informed about psychological research.
Psychologists study behavior of both humans and animals, and the main purpose of this
research is to help us understand people and to improve the quality of human lives. The
results of psychological research are relevant to problems such as learning and memory,
homelessness, psychological disorders, family instability, and aggressive behavior and
violence. Psychological research is used in a range of important areas, from public
policy to driver safety. It guides court rulings with respect to racism and sexism as in
the 1954 case of Brown v. Board of Education, as well as court procedure, in the use of
lie detectors during criminal trials, for example. Psychological research helps us
understand how driver behavior affects safety such as the effects of texting while
driving, which methods of educating children are most effective, how to best detect
deception, and the causes of terrorism.
Some psychological research is basic research. Basic research is research that answers fundamental questions about behavior. For instance,
bio-psychologists study how nerves conduct impulses from the receptors in the skin to
the brain, and cognitive psychologists investigate how different types of studying
influence memory for pictures and words. There is no particular reason to examine such
things except to acquire a better knowledge of how these processes occur. Applied
research is research that investigates issues that have implications
for everyday life and provides solutions to everyday problems. Applied research
has been conducted to study, among many other things, the most effective methods for
reducing depression, the types of advertising campaigns that serve to reduce drug and
alcohol abuse, the key predictors of managerial success in business, and the indicators
of effective government programs, such as Head Start.
Basic research and applied research inform
each other, and advances in science occur more rapidly when each type of research is
conducted. For instance, although research concerning the role of practice on memory for
lists of words is basic in orientation, the results could potentially be applied to help
children learn to read. Correspondingly, psychologist-practitioners who wish to reduce
the spread of AIDS or to promote volunteering frequently base their programs on the
results of basic research. This basic AIDS or volunteering research is then applied to
help change people’s attitudes and behaviors.
One goal of research is to organize information into meaningful statements that can be
applied in many situations.
A
theory is an integrated set of principles that
explains and predicts many, but not all, observed relationships within a given domain of
inquiry. One example of an important theory in psychology is the stage theory of
cognitive development proposed by the Swiss psychologist Jean Piaget. The theory states
that children pass through a series of cognitive stages as they grow, each of which must be
mastered in succession before movement to the next cognitive stage can occur. This is an
extremely useful theory in human development because it can be applied to many different
content areas and can be tested in many different ways.
Good theories have four important characteristics. A good theory is:
-
General, meaning it summarizes different outcomes.
-
Parsimonious, meaning it provides the simplest possible account
of those outcomes.
-
Provides ideas for future research.
-
Falsifiable, meaning that the variables of interest can be
adequately measured and the relationships between the variables that are predicted by
the theory can be shown through research to be incorrect.
Piaget’s stage theory of cognitive development meets all four characteristics of a good
theory. First, it is general in that it can account for developmental changes in behavior
across a wide variety of domains, and second, it does so parsimoniously—by hypothesizing a
simple set of cognitive stages. Third, the stage theory of cognitive development has been
applied not only to learning about cognitive skills but also to the study of children’s
moral and gender development. And finally, the stage theory of cognitive development is
falsifiable because the stages of cognitive reasoning can be measured and because if
research discovers, for instance, that children learn new tasks before they have reached
the cognitive stage hypothesized to be required for that task, then the theory will be
shown to be incorrect.
No single theory is able to account for all behavior in all cases. Rather, theories are
each limited in that they make accurate predictions in some situations or for some people
but not in other situations or for other people. As a result, there is a constant exchange
between theory and data: Existing theories are modified on the basis of collected data, and
the new modified theories then make new predictions that are tested by new data, and so
forth. When a better theory is found, it will replace the old one. This is part of the
accumulation of scientific knowledge as a result of research.
When psychologists have a question that they want to research, it usually comes from a
theory based on other’s research reported in scientific journals. Recall that a
theory is based on principles that are general and can be applied to many situations
or relationships. Therefore, when a scientist has a research question to study, the
question must be stated in a research hypothesis, which is a precise statement of the presumed relationship among specific
parts of a theory. Furthermore, a research hypothesis is a
specific and falsifiable prediction about the relationship between or among two or
more variables, where a variable is any attribute that can assume different values among different people or across
different times or places.
The research hypothesis states the existence of a relationship between the variables of
interest and the specific direction of that relationship. For instance, the research
hypothesis “Using marijuana will reduce learning” predicts that there is a
relationship between a variable “using marijuana” and another variable called
“learning.” Similarly, in the research hypothesis “Participating in psychotherapy
will reduce anxiety,” the variables that are expected to be related are
“participating in psychotherapy” and “level of anxiety.”
When stated in an abstract manner, the ideas that form the basis of a research hypothesis
are known as conceptual variables. Conceptual variables are abstract ideas that form the basis of research hypotheses.
Sometimes the conceptual variables are rather simple—for instance, age, gender, or
weight. In other cases the conceptual variables represent more complex ideas, such as
anxiety, cognitive development, learning, self-esteem, or sexism.
The first step in testing a research hypothesis involves turning the conceptual variables
into measured variables, which are variables
consisting of numbers that represent the conceptual variables. For instance, the
conceptual variable “participating in psychotherapy” could be represented as the measured
variable “number of psychotherapy hours the patient has accrued” and the conceptual
variable “using marijuana” could be assessed by having the research participants rate, on a
scale from 1 to 10, how often they use marijuana or by administering a blood test that
measures the presence of the chemicals in marijuana.
Psychologists use the term operational definition to refer to a precise
statement of how a conceptual variable is turned into a measured variable. The following table lists some
potential operational definitions for conceptual variables that have been used in
psychological research. As you read through this list, note that in contrast to the
abstract conceptual variables, the operational definitions are measurable and very
specific. This specificity is important for two reasons. First, more specific definitions
mean that there is less danger that the collected data will be misunderstood by others.
Second, specific definitions will enable future researchers to replicate the research.
| Examples of Some Conceptual Variables Defined as Operational Definitions for Psychological Research |
|---|
| From Flat World Knowledge, Introduction to Psychology,
v1.0, CC-BY-NC-SA. |
| Conceptual Variable |
Operational Definitions |
| Aggression |
Number of presses of a button that administers shock to another student; number of
seconds taken to honk the horn at the car ahead after a stoplight turns
green |
| Interpersonal attraction |
Number of inches that an individual places his or her chair away from another
person; number of millimeters of pupil dilation when one person looks at
another |
| Employee satisfaction |
Number of days per month an employee shows up to work on time; rating of job
satisfaction from 1 (not at all satisfied) to 9 (extremely satisfied) |
| Decision-making skills |
Number of groups able to correctly solve a group performance task; number of seconds
in which a person solves a problem |
| Depression |
Number of negative words used in a creative story; number of appointments made with
a psychotherapist |
|
learn by doing
One of the keys to developing a well-designed research study is to precisely define
the conceptual variables found in a hypothesis. When conceptual variables are turned
into operational variables in a hypothesis, it then becomes a testable hypothesis. In
this activity, read each of the following statements and answer its accompanying
question to:
- distinguish the conceptual variable from its operational definition or variable
to be tested and
- determine whether the statement describing the variables contain the
characteristics for a testable hypothesis.
did I get this
Now to make sure that you can identify the characteristics of a hypothesis and
distinguish its conceptual variables from operational definitions used in a research
study, choose an answer that correctly completes each of the following statements.
All scientists (whether they are physicists, chemists, biologists, sociologists, or
psychologists) are engaged in the basic processes of collecting data and drawing
conclusions about those data. The methods used by scientists have developed over many
years and provide a common framework for developing, organizing, and sharing
information. The scientific method is the
set of assumptions, rules, and procedures scientists use to conduct
research.
In addition to requiring that science be empirical, the
scientific method demands that the procedures used are objective, or free from the personal bias or emotions of the scientist. The
scientific method proscribes how scientists collect and analyze data, how they draw
conclusions from data, and how they share data with others. These rules increase
objectivity by placing data under the scrutiny of other scientists and even the
public at large. Because data are reported objectively, other scientists know exactly
how the scientist collected and analyzed the data. This means that they do not have
to rely only on the scientist’s own interpretation of the data; they may draw their
own, potentially different, conclusions.
In the following activity, you learn about a model presenting a five-step process of
scientific research in psychology. A researcher or a small group of researchers
formulate a research question and state a hypothesis, conduct a study designed to
answer the question, analyze the resulting data, draw conclusions about the answer to
the question, and then publish the results so that they become part of the research
literature found in scientific
journals.
Because the research literature is one of the primary sources of new research
questions, this process can be thought of as a cycle. New research leads to new
questions and new hypotheses, which lead to new research, and so on.
This model also indicates that research questions can originate outside of this cycle
either with informal observations or with practical problems that need to be solved.
But even in these cases, the researcher begins by checking the research literature to
see if the question had already been answered and to refine it based on what previous
research had already found.
learn by doing
All scientists use the the scientific method which is a set of basic processes
performed in the same order for conducting research. Using the following
diagram of the scientific method, label each of the research steps in the
correct order that scientists use to conduct scientific studies.
learn by doing
Now imagine that you are a research psychologist and you want to conduct a
study to find out if there are any negative effects of talking on a cell phone
while driving a car. What would you do first to begin your study? How would you
know if your study might provide any new information? How would you go about
conducting your study? What would you do after you have completed your study?
These are questions that every researcher must answer in order to properly
conduct a scientific study. As the researcher for your study on cell phone
usage while driving, you will need to answer all of these questions.
The research by Mehl and his colleagues is described nicely by this model. Their
question—whether women are more talkative than men—was suggested to them both by
people’s stereotypes and by published claims about the relative talkativeness of
women and men. When they checked the research literature, however, they found that
this question had not been adequately addressed in scientific studies. They conducted
a careful empirical study , analyzed the results (finding very little difference
between women and men), and published their work so that it became part of the
research literature. The publication of their article is not the end of the story,
however, because their work suggests many new questions about the reliability of the result, such as potential cultural differences that will
likely be further researched by them or other researchers.
Most new research is designed to replicate—that is, to repeat, add to, or
modify—previous research findings. The process of repeating
previous research, which forms the basis of all scientific inquiry, is known
as replication. The scientific method therefore results in an
accumulation of scientific knowledge through the reporting of research and the
addition to and modifications of previous reported findings that are then replicated
by other researchers.
One of the questions that all scientists must address concerns the ethics of their
research. Research in psychology may cause some stress, harm, or inconvenience for the
people who participate in that research. For instance, researchers may require introductory
psychology students to participate in research projects and then deceive these students, at
least temporarily, about the nature of the research. Psychologists may induce stress,
anxiety, or negative moods in their participants, expose them to weak electrical shocks, or
convince them to behave in ways that violate their moral standards. And researchers may
sometimes use animals in their research, potentially harming them in the process.
Decisions about whether research is ethical are made using established ethical codes and
standards developed by scientific organizations, such as the American Psychological
Association, and the federal government, such as the U.S. Department of Health and Human
Services (DHHS). In addition, there is no way to know ahead of time what the effects of a
given procedure will be on every person or animal who participates or what benefit to
society the research is likely to produce. What is ethical is defined by the current state
of thinking within society, and thus perceived costs and benefits change over time. The
DHHS regulations require that all universities receiving funds from the department set up
an Institutional Review Board (IRB) to determine whether proposed research meets department
regulations. The Institutional Review Board is a
committee of at least five members whose goal it is to determine the cost-benefit ratio
of research conducted within an institution. The IRB approves the procedures of all
the research conducted at the institution before the research can begin. The board may
suggest modifications to the procedures, or (in rare cases) it may inform the scientist
that the research violates DHHS guidelines and thus cannot be conducted at all.
The following table presents some of the most
important factors that psychologists take into consideration when designing their research
using people.
| Characteristics of an Ethical Research Project Using Human Participants |
|---|
| From Flat World Knowledge, Introduction to Psychology, v1.0, CC-BY-NC-SA. |
| Characteristics |
|---|
| Trust and positive rapport are created between the researcher and the
participant. |
| The rights of both the experimenter and participant are considered, and the
relationship between them is mutually beneficial. |
| The experimenter treats the participant with concern and respect and attempts to
make the research experience a pleasant and informative one. |
| Before the research begins, the participant is given all information relevant to his
or her decision to participate, including any possibilities of physical danger or
psychological stress. |
| The participant is given a chance to have questions about the procedure answered,
thus guaranteeing his or her free choice about participating. |
| After the experiment is over, any deception that has been used is made public, and
the necessity for it is explained. |
| The experimenter carefully debriefs the participant, explaining the underlying
research hypothesis and the purpose of the experimental procedure in detail and
answering any questions. |
| The experimenter provides information about how he or she can be contacted and
offers to provide information about the results of the research if the participant is
interested in receiving it. [1]
|
|
The most direct ethical concern of the scientist is to prevent harm
to the research participants. One example is the well-known research, conducted in 1961 by
Stanley Milgram, which investigated obedience to authority. Participants were induced by an
experimenter to administer electric shocks to another person so that Milgram could study
the extent to which they would obey the demands of an authority figure. Most participants
evidenced high levels of stress resulting from the psychological conflict they experienced
between engaging in aggressive and dangerous behavior and following the instructions of the
experimenter. Studies such as those by Milgram are no longer conducted because the
scientific community is now much more sensitized to the potential of such procedures to
create emotional discomfort or harm.
Another goal of ethical research is to guarantee that participants have free choice regarding whether they wish to participate in research. Students in
psychology classes may be allowed, or even required, to participate in research, but they
are also always given an option to choose a different study to be in, or to perform other
activities instead. And once an experiment begins, the research participant is always free
to leave the experiment if he or she wishes to. Concerns about free choice also occur in
institutional settings, such as in schools, hospitals, corporations, and prisons, when
individuals are required by the institutions to take certain tests or when employees are
told or asked to participate in research.
Researchers must also protect the privacy of the research
participants. In some cases data can be kept anonymous by not having the respondents put
any identifying information on their questionnaires. In other cases the data cannot be
anonymous because the researcher needs to keep track of which respondent contributed the
data. In this case one technique is to have each participant use a unique code number to
identify his or her data, such as the last four digits of the student ID number. In this
way the researcher can keep track of which person completed which questionnaire, but no one
will be able to connect the data with the individual who contributed them.
Perhaps the most widespread ethical concern to the participants in behavioral research is
the extent to which researchers employ deception. Deception occurs
whenever research participants are not completely and fully informed
about the nature of the research project before participating in it. Deception may
occur in an active way, such as when the researcher tells the participants that he or she
is studying learning when in fact the experiment really concerns obedience to authority. In
other cases the deception is more passive, such as when participants are not told about the
hypothesis being studied or the potential use of the data being collected.
Some researchers have argued that no deception should ever be used in any research. [2]
They argue that participants should always be told the complete truth
about the nature of the research they are in, and that when participants are deceived there
will be negative consequences, such as the possibility that participants may arrive at
other studies already expecting to be deceived. Other psychologists defend the use of
deception on the grounds that it is needed to get participants to act naturally and to
enable the study of psychological phenomena that might not otherwise get investigated. They
argue that it would be impossible to study topics such as altruism, aggression, obedience,
and stereotyping without using deception because if participants were informed ahead of
time what the study involved, this knowledge would certainly change their behavior. The
codes of ethics of the American Psychological Association and other organizations allow
researchers to use deception, but these codes also require them to explicitly consider how
their research might be conducted without the use of deception.
Nevertheless, an important tool for ensuring that research is ethical is the use of a
written informed consent form. Informed consent, conducted before a
participant begins a research session, is designed to explain the
research procedures and inform the participant of his or her rights during the
investigation. An informed consent form explains as much as possible about the true
nature of the study, particularly everything that might be expected to influence
willingness to participate, but it may in some cases withhold some information that allows
the study to work.
Finally, participating in research has the potential for producing long-term changes in the
research participants. Therefore, all participants should be fully debriefed immediately
after their participation. The debriefing is a
procedure designed to fully explain the purposes and procedures of the research and
remove any harmful aftereffects of participation.
learn by doing
Instructions: View the video clip that describes the Stanley
Milgram experiment on obedience and watch for any ethical violations made by the
researchers. Then using the information provided in table above titled,
"Characteristics of an Ethical Research Project Using Human Participants," answer the
following questions to determine which ethical violations occurred in the Milgram
experiment on obedience.
Note: In the following questions, the two types of participants used in Stanley
Milgram’s study are the “participant-punisher” who administers electric shocks and
the “participant-learner” who repeats the paired-word combinations.
Research with Animals
Because animals make up an important part of the natural world, and because some
research cannot be conducted using humans, animals are also participants in
psychological research. Most psychological research using animals is now conducted
with rats, mice, and birds; the use of other animals in research is declining. As
with ethical decisions involving human participants, basic principles have been
developed to help researchers make informed decisions about such research.
The following table summarizes the APA
Guidelines on Humane Care and Use of Animals in Research.
| APA Guidelines on Humane Care and Use of Animals in Research |
|---|
| From Flat World Knowledge, Introduction to Psychology, v1.0, CC-BY-NC-SA. |
| APA Guidelines |
|---|
| The following are some of the most important ethical principles from the
American Psychological Association’s guidelines on research with animals. |
| Psychologists acquire, care for, use, and dispose of animals in compliance
with current federal, state, and local laws and regulations, and with
professional standards. |
| Psychologists trained in research methods and experienced in the care of
laboratory animals supervise all procedures involving animals and are
responsible for ensuring appropriate consideration of their comfort, health,
and humane treatment. |
| Psychologists ensure that all individuals under their supervision who are
using animals have received instruction in research methods and in the care,
maintenance, and handling of the species being used, to the extent appropriate
to their role. |
| Psychologists make reasonable efforts to minimize the discomfort, infection,
illness, and pain of animal subjects. |
| Psychologists use a procedure subjecting animals to pain, stress, or privation
only when an alternative procedure is unavailable and the goal is justified by
its prospective scientific, educational, or applied value. |
| Psychologists perform surgical procedures under appropriate anesthesia and
follow techniques to avoid infection and minimize pain during and after
surgery. |
| When it is appropriate that an animal’s life be terminated, psychologists
proceed rapidly, with an effort to minimize pain and in accordance with
accepted procedures. [3]
|
|
Because the use of animals in research involves a personal value, people naturally
disagree about this practice. Although many people accept the value of such research,
a minority of people, including animal-rights activists, believes that it is
ethically wrong to conduct research on animals. This argument is based on the
assumption that because animals are living creatures just as humans are, no harm
should ever be done to them.
Most scientists, however, reject this view. They argue that such beliefs ignore the
potential benefits that have and continue to come from research with animals. For
instance, drugs that can reduce the incidence of cancer or AIDS may first be tested
on animals, and surgery that can save human lives may first be practiced on animals.
Research on animals has also led to a better understanding of the physiological
causes of depression, phobias, and stress, among other illnesses. In contrast to
animal-rights activists, then, scientists believe that because there are many
benefits that accrue from animal research, such research can and should continue as
long as the humane treatment of the animals used in the research is guaranteed.
learn by doing
Determine whether each each of the following scenarios is a compliance or
violation of the ethical and humane care and use of animals as outlined by the
American Psychological Association. Then select the appropriate guideline that
applies to each scenario. To help you with this activity, you may want to
review the APA Guidelines on Humane Care and Use of Animals in Research
presented earlier.
learn by doing
Imagine you are on the Animal Care and Use Committee at your college. It is
part of your responsibility to evaluate and either approve or reject research
proposals of faculty members who want to use animals for research or
instructional purposes. The two proposals are based on real experiments and
describe the studies including goals, benefits, and discomforts or injuries of
animals used. You must either approve or disapprove the research proposal based
on the information provided. There is no need to suggest improvements or
experimental design changes. Indicate why you decided upon the course of action
that you did for each proposal. [4]
Case 1
Professor Smith is a psychobiologist working on the frontiers of a new and
exciting research area of neuroscience, brain grafting. Research has shown that
neural tissue can be be removed from the brains of monkey fetuses and implanted
into the brains of monkeys that have suffered brain damage. The neurons seem to
make the proper connections and are sometimes effective in improving
performance in brain-damaged animals. These experiments offer important animal
models for human degenerative diseases such as Parkinson’s and Alzheimer’s. Dr.
Smith want to transplant tissue from fetal monkey brains into the entorhinal
cortex of adult monkeys; this is the area of the human brain that is involved
with Alzheimer’s disease.
The experiment will use 20 adult rhesus monkeys. First, the monkeys will be
subjected to brain lesioning. The procedure will involve anesthetizing the
animals, opening their skulls, and making lesions using a surgical instrument.
After they recover, the monkeys will be tested on a learning task to make sure
their memory is impaired. Three months later, half of the animals will be given
transplant surgery. Tissue taken from the cortex of the monkey fetuses will be
implanted into the area of the brain damage. Control animals will be subjected
to a placebo surgery, and all animals will be allowed to recover for 2 months.
They will then learn a task to test the hypothesis that the animals having
brain grafts will show better memory than the control group.
Dr. Smith argues that this research is in the exploratory stages and can only
be done using animals. She further states that in 10 years, over 2 million
Americans will have Alzheimer’s disease and that her research could lead to a
treatment for the devastating memory loss that Alzheimer’s victims suffer. [4]
Case 2
The Psychology Department is requesting permission from your committee to use
10 rats per semester for demonstration experiments in a physiological
psychology course. The students will work in groups of three; each group will
be given a rat. The students will first perform surgery on the rats. Each
animal will be anesthetized. Following standard surgical procedures, an
incision will be made in the scalp and two holes drilled in the animal’s skull.
Electrodes will be lowered into the brain to create lesions on each side. The
animals will then be allowed to recover. Several weeks later, the effects of
destroying this part of the animal’s brain will be tested in a shuttle
avoidance task in which the animals will learn when to cross over an
electrified grid.
The instructor acknowledges that the procedure is a common demonstration and
that no new scientific information will be gained from the experiment. He
argues, however, that students taking a course in physiological psychology must
have the opportunity to engage in small animal surgery and to see firsthand the
effects of brain lesions. [4]
References
- Stangor, C.
(2011).
Research Methods for the Behavioral Sciences. Cengage. Mountain View, CA. Edition 4th.
- Baumrind,
Diana
(1985).
"Research using intentional deception: Ethical issues revisited."
American Psychologist. Volume 40. Number 2. 165–174 Pages.
- APA (American Psychological Association)
(2002).
"Ethical principles of psychologists ." American Psychologist. Volume 57. Number 12. 1060–1073 Pages.
- Herzog, Harold A.
(1990).
"Discussing animal rights and animal research in the classroom."
Teaching of Psychology. Volume 17. Number 2. 90–94 Pages.
Psychologists agree that if their ideas and theories about human behavior are to be taken
seriously, they must be backed up by data collected through research. The research goals
that a psychologist wants to study determine the use of one of three types of research
approaches. These varying approaches, summarized in the table
below,
are known as research designs. A research design is the specific method a researcher uses to collect, analyze, and interpret
data. Psychologists use three major types of research designs in their research,
and each provides an essential avenue for scientific investigation.
-
Descriptive research is research designed to provide a snapshot of the current state of
affairs.
-
Correlational research is research designed to discover relationships among variables and to
allow the prediction of future events from present knowledge.
-
Experimental research is research in which there is random assignment of research participants into two groups. This is
followed by a manipulation of a given experience for one group while the other is not
manipulated. The two groups are then compared to determine the influence of the
manipulation.
Each of the three research designs varies according to its strengths and limitations, and
it is important to understand how each differs.
| Characteristics of the Three Research Designs |
|---|
| From Flat World Knowledge, Introduction to Psychology, v1.0: Stangor, C. (2011). Research Methods for the Behavioral Sciences (4th ed.). Mountain View, CA: Cengage. |
| Research design |
Goal |
Advantages |
Disadvantages |
| Descriptive |
To create a snapshot of the current state of affairs. |
Provides a relatively complete picture of what is occurring at a given time. Allows
the development of questions for further study. |
Does not assess relationships among variables. May be unethical if participants do
not know they are being observed. |
| Correlational |
To assess the relationships between and among two or more variables. |
Allows testing of expected relationships between and among variables and the making
of predictions. Can assess these relationships in everyday life events. |
Cannot be used to draw inferences about the causal relationships between and among
the variables. |
| Experimental |
To assess the causal impact of one or more experimental manipulations on a dependent
variable. |
Allows drawing of conclusions about the causal relationships among variables. |
Cannot experimentally manipulate many important variables. May be expensive and time
consuming. |
|
Descriptive research is designed to create a snapshot of the current thoughts, feelings, or
behavior of individuals. There are three types of descriptive research: case studies, surveys, and naturalistic
observation.
Sometimes the data in a descriptive research project is based on only a small set of
individuals, often only one person or a single small group. These research designs are
known as case studies—descriptive records of one or more individuals’ experiences and behavior.
Sometimes case studies involve ordinary individuals, as when developmental psychologist
Jean Piaget used his observation of his own children to develop his stage theory of
cognitive development. More frequently, case studies are conducted on individuals who have
unusual or abnormal experiences or characteristics or who find themselves in particularly
difficult or stressful situations. The assumption is that we can learn something about
human nature by carefully studying individuals who are socially marginal, experiencing
unusual situations, or going through a difficult phase in their lives.
Sigmund Freud was a master of using the psychological difficulties of individuals to draw
conclusions about basic psychological processes. Freud wrote case studies of some of his
most interesting patients and used these careful examinations to develop his important
theories of personality. One classic example is Freud’s description of “Little Hans,” a
child whose fear of horses the psychoanalyst interpreted in terms of repressed sexual
impulses and the Oedipus complex.
The second type of descriptive research is the survey—a measure administered through either a
face-to-face or telephone interview, or a written or computer-generated questionnaire—to
get a picture of the beliefs or behaviors of a sample of people of interest. The
people chosen to participate in the research, called a sample, are selected to be representative of all
the people that the researcher wishes to know about, called the population. In election polls, for instance, a sample is taken from the population
of all “likely voters” in the upcoming elections.
The results of surveys may sometimes be rather mundane, such as “nine out of ten doctors
prefer Tymenocin,” or “the median income in Montgomery County is $36,712.” Yet other times
(particularly in discussions of social behavior), the results can be shocking: “more than
40,000 people are killed by gunfire in the United States every year,” or “more than 60% of
women between the ages of 50 and 60 suffer from depression.” Descriptive research is
frequently used by psychologists to get an estimate of the prevalence (or incidence) of psychological disorders.
The third type of descriptive research—known as naturalistic observation—is research based on the
observation of everyday events occurring in the natural environment of people or
animals. For instance, a developmental psychologist who watches children on a
playground and describes how they interact is conducting descriptive research. Another
example of naturalistic research is a bio-psychologist who observes animals in their
natural habitats.
A famous example of this type of research is the work of Dr. Jane Goodall at her primate
research facility in Gombe Stream National Park, Tanzania (on the continent of Africa).
Goodall and her staff have observed and recorded the social interactions and family life of
the Kasakela chimpanzee community for over 50 years. Their work is considered
groundbreaking and has revealed aspects of chimpanzee life that may have gone undiscovered.
For instance, Goodall described human-like socializing behaviors in that members of the
group would show affection and encouragement to one another. It was discovered that the
chimpanzees were toolmakers and users—stripping leaves from twigs and poking the twig into
termite holes to retrieve a meal. Goodall also described the carnivore side of chimpanzees,
reporting that hunting groups from the chimpanzee community would stalk, isolate, and kill
smaller primates for food and then divide their kill for distribution to other group
members.
Two parts of Dr. Goodall’s research methods are representative of the disadvantages of
naturalistic observational research. First, she decided to name the chimpanzees she studied
instead of using the scientific convention of numbering subjects. The numbering technique
hypothetically promotes objective observation that is devoid of attachment and bias on the
part of the observer. Dr. Goodall identified members of her chimpanzee community by name,
and discussed their behavior in terms of emotion, personality, intelligence, and family
relationships; she was criticized by some for becoming overly involved and thus more
subjective in her interpretations. This is known as observer bias,
which happens when the individual observing behavior is influenced by
their own experiences, expectations, or knowledge about the purpose of the observation
or study.
Second, the Gombe research team utilized feeding stations to attract the animals for
observation, thus potentially altering the natural feeding patterns and behaviors of the
troop.
This
may have promoted artificial competition and increased aggression among the chimpanzees
when the observers meaningfully interacted with the chimpanzees. This is called the observer effect. Indeed, the observer effect (interference with or modification of the subject’s behaviors by the process of
observation) can lead to a distorted picture of a natural phenomenon, thus
defeating the point of “naturalistic” observational research. It is difficult to know how
influential the presence of a stranger can be in an established social situation or for the
subject being observed.
In many observational studies, particularly those conducted with children, the observers
are hidden away from the subjects.
Some
researchers use two-way mirrors, others use hidden cameras with monitors located in a
separate room. Subjects can also be recorded on video from several angles as they interact
socially or within their environment; the video recordings can then be observed and data
recorded at a later time. A major advantage to this method is the ability to have two or
more observers observe and record the behavior, followed by calculating a score for interrater reliability. This score can estimate how
much agreement there is between the two observers about what the subjects were
doing. This type of test can also identify observer bias.
An
advantage of descriptive research is that it attempts to capture the complexity of everyday
behavior. Specifically, case studies provide detailed information about a single person or
a small group of people and surveys capture the thoughts or reported behaviors of a large
population of people. Naturalistic observation, meanwhile, objectively record the behavior
of people or animals as it naturally occurs. In sum, descriptive research is used to
provide a relatively complete understanding of what is currently happening.
Despite these advantages, descriptive research has a distinct disadvantage in that,
although it allows us to get an idea of what is currently happening, it is usually limited
to static pictures. Although descriptions of particular experiences may be interesting,
they are not always transferable to other individuals in other situations, nor do they tell
us exactly why specific behaviors or events occurred. For instance, descriptions of
individuals who have suffered a stressful event, such as a war or an earthquake, can be
used to understand the individuals’ reactions to the event but cannot tell us anything
about the long-term effects of the stress. And because there is no comparison group that
did not experience the stressful situation, we cannot know what these individuals would be
like if they hadn’t had the stressful experience.
In contrast to descriptive research, which is designed primarily to provide static
pictures, correlational research involves measuring the relationship between or
among two or more relevant variables. For instance, the variables of height and weight
are systematically related (correlated) because taller people generally weigh more than
shorter people. In the same way, study time and memory errors are also related, because the
more time a person is given to study a list of words, the fewer errors he or she will make.
When there are two variables in the research design, one of them is called the predictor variable and the other the outcome
variable.
One way of organizing the data from a correlational study with two variables is to graph
the values of each of the measured variables using a scatter plot. As you can see in figure
below,
a scatter plot is a visual image of the
relationship between two variables. A point is plotted for each individual at the
intersection of his or her scores for the two variables. When the
association between the variables on the scatter plot can be easily approximated with a
straight line, as in parts (a) and
(b), the
variables are said to have a linear relationship.
When the straight line indicates that individuals who have above-average values for one
variable also tend to have above-average values for the other variable, as in part (a), the
relationship is said to be positive linear. Examples of positive
linear relationships include those between height and weight, between education and income,
and between age and mathematical abilities in children. In each case people who score
higher on one of the variables also tend to score higher on the other variable. Negative linear relationships, in contrast, as shown in part (b),
occur when above-average values for one variable tend to be associated with below-average
values for the other variable. Examples of negative linear relationships include those
between the age of a child and the number of diapers the child uses, and between practice
on and errors made on a learning task. In these cases, people who score higher on one of
the variables tend to score lower on the other variable.
Relationships between variables that cannot be described with a straight line are known as
nonlinear relationships. Part
(c)
shows a common pattern in which the distribution of the points is essentially random. In
this case there is no relationship at all between the two variables, and they are said to
be independent.
The most common statistical measure of the strength of linear
relationships among variables is the Pearson
correlation coefficient, which is symbolized by the letter r. The value of the correlation coefficient ranges from r = –1.00 to r = +1.00. The direction of the
linear relationship is indicated by the sign of the correlation coefficient. Positive
values of r (such as r= .54 or r = .67) indicate that the relationship is positive linear (i.e.,
the pattern of the dots on the scatter plot runs from the lower left to the upper right),
whereas negative values of r (such as r =
–.30 or r = –.72) indicate negative linear relationships (i.e., the
dots run from the upper left to the lower right). The strength of the linear relationship
is indexed by the distance of the correlation coefficient from zero (its absolute value).
For instance, r = –.54 is a stronger relationship than r = .30, and r = .72 is a stronger
relationship than r = –.57.
An important limitation of correlational research designs is that they cannot be used to
draw conclusions about the causal relationships among the measured variables. Consider, for
instance, a researcher who has hypothesized that viewing violent behavior will cause
increased aggressive play in children. He has collected, from a sample of fourth-grade
children, the data on how many violent television shows each child views during the week.
He has also collected the data on how aggressively each child plays on the school
playground. From his collected data, the researcher discovers a positive correlation
between the two measured variables.
Although this positive correlation appears to support the researcher’s hypothesis, it
cannot be taken to indicate that viewing violent television causes aggressive behavior.
Although the researcher is tempted to assume that viewing violent television causes
aggressive play, there are other possibilities.
It may be possible that the causal direction is exactly opposite from what has been
hypothesized. Perhaps children who buhave aggressively at school develop residual
excitement that leads them to want to watch violent television shows at home:
Although this possibility may seem less likely, there is no way to rule out the possibility
of such reverse causation on the basis of this observed correlation. It is also possible
that both causal directions are operating and that the two variables cause each other:
Another possible explanation for the observed correlation is that it has been produced by
the presence of a common-causal variable (also known as a third variable). A common-causal variable is a variable that is not
part of the research hypothesis but that causes both the predictor and the outcome
variable and thus produces the observed correlation between them. In our example, a
potential common-causal variable is the discipline style of the children’s parents. Parents
who use a harsh and punitive discipline style may produce children who like to watch
violent television and who behave aggressively in comparison to children whose parents use
less harsh discipline:
In this case, television viewing and aggressive play would be positively correlated (as
indicated by the curved arrow between them), even though neither one caused the other but
they were both caused by the discipline style of the parents (the straight arrows). When
the predictor and outcome variables are both caused by a common-causal variable, the
observed relationship between them is said to be spurious. A spurious relationship is a
relationship between two variables in which a common-causal variable produces and
“explains away” the relationship. If effects of the common-causal variable were
taken away, or controlled for, the relationship between the predictor and outcome variables
would disappear. In the example, the relationship between aggression and television viewing
might be spurious because by controlling for the effect of the parents’ disciplining style,
the relationship between television viewing and aggressive behavior might go away.
Common-causal
variables in correlational research designs can sometimes be thought of as “mystery”
variables. For instance, some variables have not been measured or their presence and
identity are unknown to the researcher. Since it is not possible to measure every variable
that could cause both the predictor and outcome variables, the existence of an unknown
common-causal variable is always a possibility. For this reason, we are left with the basic
limitation of correlational research: Correlation does not demonstrate causation. It is
important that when you read about correlational research projects, you keep in mind the
possibility of spurious relationships and be sure to interpret the findings appropriately.
Although correlational research is sometimes reported as demonstrating causality without
any mention being made of the possibility of reverse causation or common-causal variables,
informed consumers of research, like you, are aware of these interpretational problems.
In summary, correlational research designs have both strengths and limitations. One
strength is that they can be used when experimental research is not possible because the
predictor variables cannot be manipulated. Correlational designs also have the advantage of
allowing the researcher to study behavior as it occurs in everyday life. And we can also
use correlational designs to make predictions—for instance, to predict from the scores on
their battery of tests the success of job trainees during a training session. But we cannot
use such correlational information to determine whether the training caused better job
performance. For that, researchers rely on experiments.
learn by doing
Instructions: Each of the following examples describes an
actual correlational study. Your task is to decide what the results look like. Was
there a positive correlation, a negative correlation, or no correlation?
All of the research reported here is loosely based on actual studies. Because most
published research is more complicated than the descriptions given here, we have
simplified—but hopefully not seriously distorted—the results of actual research.
Research Study 1
Researchers found that the constant exposure to mass media (television, magazines,
websites) depicting atypically thin, glamorous female models (the thin-ideal body)
may be linked to body image disturbance in women. The general finding was that the
more women were exposed to pictures and articles about thin females perceived as
ideal, the lower their satisfaction was with their own bodies.
Research Study 2
This research study found that kindergarten and elementary school children who were
better at rhymes and hearing the sounds of individual letters before they started to
read later learned to read words more quickly than children who were not as good with
making and distinguishing elementary sounds of language.
Research Study 3
Ninth-grade students and teachers were surveyed to determine the level of bullying
that the students experienced. The researchers were given permission to access scores
of the students on several standardized tests, with topics including algebra, earth
science, and world history. The researchers found that the more bullying a student
experienced, the lower the student’s grades on the standardized tests.
Research Study 4
At one time, people used to assume that poor reading abilities were caused by low
intelligence. The most thoroughly studied kind of reading problem is called dyslexia,
a learning disability which appears in elementary school readers as difficulty
learning to recognize individual words. Dyslexia can vary in seriousness from mild
forms to profound levels. In one study, researchers assessed a large number of
kindergarten and first-grade children for signs of dyslexia, and they also measured
the children’s IQ using a standardized IQ measure. They found no relationship between
IQ and seriousness of dyslexia.
Research Study 5
Researchers from the United Kingdom analyzed results of a survey of more than 5,000
young people ages 10 to 15. They used a variety of indicators to rate how healthy a
lifestyle each person led, using factors like eating and drinking habits, smoking and
drug use, and participation in sports and other activities. In addition, they used
responses to several questions to rate each person on his or her level of happiness.
They found that healthier habits were strongly related to how happy these young
adolescents reported themselves to be.
True experiments are the only reliable method scientists have for inferring causal
relationships between two variables of interest: Does one thing cause another? So, the goal of an experimental research design is to provide more
definitive conclusions about the causal relationships among the variables in the research
hypothesis than is available from correlational designs.
In an experimental research design, the variables of interest are called the independent variable (or variables) and the
dependent variable. The independent variable in an experiment is the causing
variable that is created (manipulated) by the experimenter. The dependent variable in an experiment is a measured variable that is expected to be influenced by the experimental
manipulation. The research hypothesis suggests that the manipulated independent
variable or variables will cause changes in the measured dependent variables. We can
diagram the research hypothesis by using an arrow that points in one direction. This
demonstrates the expected direction of causality:
An example of the use of these independent and dependent variables in an experiment is the
effect of witnessing aggression on children’s aggressive behaviors—certainly an important
developmental question given the television and video game influence currently in place. In
a classic study conducted by Albert Bandura in 1961, it was revealed that children who
first watched an adult demonstrating violent behavior on a Bobo doll (inflatable clown with
sand at the base) in a play room were more likely to show the same aggressive behaviors,
compared to children who watched a passive adult in the play room or no adult at all in the
play room before each child entered the play room. The independent variable manipulated by
the experimenter was viewing violent behavior with the Bobo doll. The dependent variable,
or the measure of behavior, was whether the child in a play room by his or herself
expressed aggression by hitting a Bobo doll. The operational
definition of this dependent variable was the number of hits, kicks, and other
displays of aggression the child inflicted on the Bobo doll. The design of the experiment
is shown in the following figure .
Consider an experiment conducted by Anderson and Dill. [1] The study was designed to
test the hypothesis that viewing violent video games would increase aggressive behavior. In
this research, male and female undergraduates from Iowa State University were given a
chance to play with either a violent video game (Wolfenstein 3D) or a nonviolent video game
(Myst). During the experimental session, the participants played their assigned video games
for 15 minutes. Then, after the play, each participant played a competitive game with an
opponent in which the participant could deliver blasts of white noise through the earphones
of the opponent. The operational definition of the dependent variable (aggressive behavior)
was the level and duration of noise delivered to the opponent. The design of the experiment
is shown in the figure below.
Anderson and Dill first randomly assigned about 100 participants to each of
their two groups (Group A and Group B). Because they used random assignment to
conditions, they could be confident that, before the experimental manipulation
occurred, the students in Group A were, on average, equivalent to the students
in Group B on every possible variable, including variables that are likely to
be related to aggression, such as parental discipline style, peer
relationships, hormone levels, diet—and in fact everything else.
Then, after they had created initial equivalence, Anderson and Dill created the
experimental manipulation—they had the participants in Group A play the violent
game and the participants in Group B play the nonviolent game. Then they
compared the dependent variable (the white noise blasts) between the two
groups, finding that the students who had viewed the violent video game gave
significantly longer noise blasts than did the students who had played the
nonviolent game.
Anderson and Dill had from the outset created initial equivalence between the
groups. This initial equivalence allowed them to observe differences in the
white noise levels between the two groups after the experimental manipulation,
leading to the conclusion that it was the independent variable (and not some
other variable) that caused these differences. The idea is that the only thing
that was different between the students in the two groups was the video game
they had played.
Experimental designs have two very nice features. For one, they guarantee that
the independent variable occurs prior to the measurement of the dependent
variable. This eliminates the possibility of reverse causation. Second, the
influence of common-causal variables is controlled, and thus eliminated, by
creating initial equivalence among the participants in
each of the experimental conditions before the manipulation occurs.
The most common method of creating equivalence among the experimental
conditions is through random assignment to
conditions, a procedure in which the
condition that each participant is assigned to is determined through a
random process, such as drawing numbers out of an envelope or using a random
number table.
Despite the advantage of determining causation, experiments do have
limitations. One is that they are often conducted in laboratory situations
rather than in the everyday lives of people. Therefore, we do not know whether
results that we find in a laboratory setting will necessarily hold up in
everyday life. Second, and more important, is that some of the most interesting
and key social variables cannot be experimentally manipulated. If we want to
study the influence of the size of a mob on the destructiveness of its
behavior, or to compare the personality characteristics of people who join
suicide cults with those of people who do not join such cults, these
relationships must be assessed using a quasi-experiemental design because it
may simply not possible to randomly assign subjects to groups or manipulate
variables of interest.
Considering the phenomenon of aggression, certainly some would argue that spanking is a
demonstration of aggression to which some children are exposed. Does spanking increase
aggression in children? To study this question with an experimental design, one would need
to recruit families into the study, randomly divide them into “spanking” and “non-spanking”
groups, and compare the aggression in the children from the two groups. However, it would
not be ethical or even possible to compel parents to spank their children in order to
manipulate the independent variable. Thus, the strategy for this type of research would be
a quasi-experimental design, which compares two
groups that already exist in the population—in this case families who spank their
children and those who do not. However, this nonrandom design eliminates the possibility of
finding a causal relationship because we could never be sure there wasn’t a third variable
contributing to differences in aggression. For instance, perhaps the families who do not
spank their children also watch a significant amount of violence on television while the
spanking families watch much less television in general. There’s no pattern or order to
these habits, but they can nonetheless influence the analysis, particularly if there’s no
difference in aggression found. Why? If spanking increases aggression and so does violent
television, the groups might be about equal in aggression but for completely different
reasons. Without random assignment and controlling for extraneous variables, it’s not
possible to discover causality. Thus, quasi-experiments are used to describe relationships
between existing groups. We call these pre-existing variables quasi-independent variables, and studies that use quasi-independent variables
instead of randomly assigned true independent variables quasi-experiments.
learn by doing
In this activity, you will view a series of short videos about
experimental designs. For each video, you will answer several
questions:
- What is the dependent variable? If there is more than one, identify
all of the dependent variables.
- What is the independent variable? If there is more than one, identify
all of the independent variables.
- Is this a true experiment or a quasi-experiment?
- What conclusions can we draw from this study about the relationship
between the independent and dependent variables?
Study 1: Reducing Stress
Background: Social Psychologist Mark Baldwin has
studied the relationship between stressful environments and feelings of
anxiety. He wondered if stressful work might lead people to expect and
even search for negative messages, such as angry facial expressions, from
other people. This can be a problem, because these negative messages then
add to the stress which in turn increases anxiety. In this video, Dr.
Baldwin shows a creative way to help people break away from this
stress-induced tendency to search for negative messages.
Summary of the experiment:
Telemarketers were randomly assigned to one of two tasks. Some of them
looked for happy faces among sets of non-smiling faces. This version of
the independent variable was the “treatment condition” because the
experimenter believed that this task would be the one that would reduce
stress levels. The other task was to search for flowers with five petals.
This was the control condition, because the experimenter believed that
this task would have little if any beneficial effect on stress.
Because telemarketers were randomly assigned to one of the two tasks, we can call
this a TRUE experiment. If they had been assigned based on personal characteristics
or preferences or some other nonrandom basis, we would call this a
quasi-experiment.
 Photo captured from “Anti-Stress Video Game” by ScienCentral, Inc.
Partial Funding by National Science Foundation.
Photo captured from “Anti-Stress Video Game” by ScienCentral, Inc.
Partial Funding by National Science Foundation.
The primary dependent variable in this study was stress hormone level.
Stress hormones are a biological indicator of the stress that the person
is feeling, so level of the hormone is a valuable measure of actual
stress experienced, and it does not depend on people’s personal
statements about their feelings of stress, which might be distorted by
various other factors. The researchers also looked at telemarketing
sales, though the idea is that lower stress leads to better performance,
so telemarketing sales are only indirectly affected by the task.
The research question was this: Does the specific task—looking for smiling faces
versus flowers—affect stress hormone levels and telemarketing sales performance?
 Photo captured from “Anti-Stress Video Game” by ScienCentral, Inc.
Partial Funding by National Science Foundation.
Photo captured from “Anti-Stress Video Game” by ScienCentral, Inc.
Partial Funding by National Science Foundation.
The results were clear. Stress hormones were 17% lower in the group that looked for
smiling faces when compared to the control group. The only known difference between
these groups was the task itself, so—tentatively—we can conclude that the task of
looking for smiling faces caused the people in that group to have lower stress levels
than similar telemarketers in the other group.
The results also showed that telemarketing sales in the treatment group (smiling
faces) were 68% higher than sales for those in the control group (flowers). Here,
too, we can tentatively conclude that the task of looking for smiling faces caused
the people in that group to have higher telemarketing sales than similar
telemarketers in the other group.
 Photo captured from “Anti-Stress Video Game” by ScienCentral, Inc.
Partial Funding by National Science Foundation.
Photo captured from “Anti-Stress Video Game” by ScienCentral, Inc.
Partial Funding by National Science Foundation.
Study 2: Red for Romance?
Background: Psychologist Daniella Niesta is a
researcher who is interested in factors that influence our motivation.
Some factors that influence our behavior and thoughts can be unconscious
and subtle. Dr. Niesta believes that colors often have meaning, and that
red, particularly in a context of romantic attraction, carries a strong
subconscious meaning for men. If she is correct, then colors associated
with a romantic context should influence men’s feelings of attraction and
interest.
Summary of the experiment:
Undergraduate males were randomly assigned to one of two conditions. The
men in one group saw a picture of a woman wearing a red blouse and the
men in the other condition saw the same picture, except that the blouse
had been digitally altered to be blue. The color of the shirt was the
independent variable.
 Photo captured from “Red: The Color to a Man’s Heart?” by ScienCentral, Inc. Partial Funding by National Science Foundation.
Photo captured from “Red: The Color to a Man’s Heart?” by ScienCentral, Inc. Partial Funding by National Science Foundation.
The men then rated the woman on the question:”How attractive do you think this person
is?” They answered on a 9-point scale, where 1 was labeled “not at all” and 9 was
labeled “extremely.” They were also asked other related questions and answered these
on a similar scale.
 Photo captured from “Red: The Color to a Man’s Heart?” by ScienCentral, Inc. Partial Funding by National Science Foundation.
Photo captured from “Red: The Color to a Man’s Heart?” by ScienCentral, Inc. Partial Funding by National Science Foundation.
The results showed that the woman was rated as more attractive on the
average when she was depicted in a red blouse than when she was in a blue
blouse. Other related questions showed a similar higher level of
attraction for the woman when the shirt was red.
Dr. Niesta also looked at other colors: green, gray, and white. The same
pattern of results showed when red was up against these other colors. Men
found the woman more attractive when she was wearing red.
Study 3
Background: Dr. Ahmed El-Sohemy is a professor of
nutritional science at the University of Toronto. In this study, he was
interested in differences in people’s ability to regulate their own food
intake, particularly their consumption of sugar. He divided people
according to which version of a particular gene they had and studied
their eating behavior. Watch the video for more details.
Summary of the experiment:
Previous research had indicated to Dr. El-Sohemy that the GLUT2 gene
might be involved in regulation of sugar consumption. He recruited
volunteers and, using blood samples, divided his volunteers into two
groups according to the variation on the GLUT2 gene each person had. The
gene with its two variations (alleles) was the quasi-independent
variable.
 Photo courtesy of National Human Genome Research Institute, Public Domain.
Photo courtesy of National Human Genome Research Institute, Public Domain.
He then had each person fill out an extensive questionnaire on their
eating behaviors. For the study reported here, sugar consumption based on
these reports was the dependent variable.
 Photo captured from "Sweet Tooth
Gene" by ScienCentral, Inc. Partial Funding by National Science
Foundation.
Photo captured from "Sweet Tooth
Gene" by ScienCentral, Inc. Partial Funding by National Science
Foundation.
The researcher found that people with different versions of the gene
consumed substantially different amounts of sugar. The researcher
speculated that this gene might be associated with sensitivity to sugar
so it could influence how much we eat before we feel we have had enough.
did I get this
Example 1
A researcher is interested in the effects of a famous author on the persuasiveness of
a message. He recruits 50 college students to be in his study and randomly assigns 25
to be in the “high prestige” group and 25 to the be in the “low prestige” group. All
of the students read the same document about the importance of improving mental
health services at the college. But the 25 students in the “high prestige” group read
on the document that the author is the chairperson of the Psychology Department. The
25 students in the “low prestige” group read on the document that the author is a
psychology undergraduate student as part of a class assignment. Everyone was asked
after reading the article to indicate how much they agreed with the idea that
psychological services should be improved at the college.
Example 2
A therapist develops a new approach to treating depression using exercise
and diet along with regular counseling sessions. For all of her new
clients who agree to be in her test of the therapy approach, she randomly
assigns half to receive her new form of treatment and the other half
receive the traditional form of treatment that the therapist has offered
for many years. She uses a respected, standardized measure of depression
before the beginning of her therapy and then again after 3 months of
treatment. She uses the difference between these before and after
measures to indicate the change in level of depression.
Example 3
A researcher is interested to see if older adults (70 to 80 years old) have more
trouble with multitasking than middle-age adults (40 to 50 years old). Participants
were seated in a driving simulator that allowed them to drive a simulated car through
a variety of situations. They were asked to carry on a hands-free cellphone
conversation with an experimenter located in a different room during the driving
test. The experimenters measured driving abilities, including avoidance of problems,
speed, braking effectiveness, and other related behaviors.
References
- Anderson, C. A., and Dill, K. E.
(2000).
"Video games and aggressive thoughts, feelings, and behavior in the
laboratory and in life." Journal of Personality and Social Psychology .
Volume 78. Number 4. 772–790 Pages.
Good research is valid research. When research is valid, the
conclusions drawn by the researcher are legitimate. For instance, if a researcher
concludes that participating in psychotherapy reduces anxiety, or that taller people are
smarter than shorter people, the research is valid only if the therapy really works or
if taller people really are smarter. Unfortunately, there are many threats to the
validity of research, and these threats may sometimes lead to unwarranted conclusions.
Often, and despite researchers’ best intentions, some of the research reported on
websites as well as in newspapers, magazines, and even scientific journals is invalid.
Validity is not an all-or-nothing proposition, which means that some research is more
valid than other research. Only by understanding the potential threats to validity will
you be able to make knowledgeable decisions about the conclusions that can or cannot be
drawn from a research project. Here we discuss two of these major types of threats to
the validity of research: internal and external validity.
Two Threats to the Validity of Research
-
Threats to internal validity. Although it is claimed that
the independent variable caused the dependent variable, the dependent variable
actually may have been caused by a confounding variable.
-
Threats to external validity. Although it is claimed that
the results are more general, the observed effects may actually only be found under
limited conditions or for specific groups of people. [1]
Internal validity refers to the extent to which we can trust the conclusions that have been drawn
about the causal relationship between the independent and dependent variables.
Internal validity applies primarily to experimental research designs, in which the
researcher hopes to conclude that the independent variable has caused the dependent
variable. Internal validity is maximized when the research is free from the presence of
confounding variables—variables other than the independent variable on which the
participants in one experimental condition differ systematically from those in other
conditions.
Consider an experiment in which a researcher tested the hypothesis that drinking alcohol
makes members of the opposite sex look more attractive. Participants older than 21 years
of age were randomly assigned either to drink orange juice mixed with vodka or to drink
orange juice alone. To eliminate the need for deception, the participants were told
whether or not their drinks contained vodka. After enough time had passed for the
alcohol to take effect, the participants were asked to rate the attractiveness of
pictures of members of the opposite sex. The results of the experiment showed that, as
predicted, the participants who drank the vodka rated the photos as significantly more
attractive.
If you think about this experiment for a minute, it may occur to you that although the
researcher wanted to draw the conclusion that the alcohol caused the differences in
perceived attractiveness, the expectation of having consumed alcohol is confounded with
the presence of alcohol. That is, the people who drank alcohol also knew they drank
alcohol, and those who did not drink alcohol knew they did not. It is possible that
simply knowing that they were drinking alcohol, rather than the effect of the alcohol
itself, may have caused the differences as shown in the following figure.
One solution to the problem of potential expectancy effects is
to tell both groups that they are drinking orange juice and vodka but really give
alcohol to only half of the participants (it is possible to do this because vodka has
very little smell or taste). If differences in perceived attractiveness are found, the
experimenter could then confidently attribute them to the alcohol rather than to the
expectancies about having consumed alcohol.
Another threat to internal validity can occur when the experimenter knows the research
hypothesis and also knows which experimental condition the participants are in. The
outcome is the potential for experimenter
bias, a situation in which the experimenter subtly
treats the research participants in the various experimental conditions differently,
resulting in an invalid confirmation of the research hypothesis. In one study
demonstrating experimenter bias, Rosenthal and Fode [2] sent twelve students to test
a research hypothesis concerning maze learning in rats. Although it was not initially
revealed to the students, they were actually the participants in an experiment. Six of
the students were randomly told that the rats they would be testing had been bred to be
highly intelligent, whereas the other six students were led to believe that the rats had
been bred to be unintelligent. In reality there were no differences among the rats given
to the two groups of students. When the students returned with their data, a startling
result emerged. The rats run by students who expected them to be intelligent showed
significantly better maze learning than the rats run by students who expected them to be
unintelligent. Somehow the students’ expectations influenced their data. They evidently
did something different when they tested the rats, perhaps subtly changing how they
timed the maze running or how they treated the rats. And this experimenter bias probably
occurred entirely out of their awareness.
To avoid experimenter bias, researchers frequently run experiments in which the
researchers are blind to condition. This means that although the
experimenters know the research hypotheses, they do not know which conditions the
participants are assigned to. Experimenter bias cannot occur if the researcher is blind
to condition. In a double-blind
experiment, both the researcher and the research
participants are blind to condition. For instance, in a double-blind trial of a
drug, the researcher does not know whether the drug being given is the real drug or the
ineffective placebo, and the patients also do not know which they are getting.
Double-blind experiments eliminate the potential for experimenter effects and at the
same time eliminate participant expectancy effects.
While internal validity refers to conclusions drawn about events that occurred within the
experiment, external validity refers to
the extent to which the results of a research design can be
generalized beyond the specific way the original experiment was conducted. Generalization is the extent to which relationships among conceptual variables can be
demonstrated in a wide variety of people and a wide variety of manipulated or
measured variables.
Psychologists who use college students as participants in their research may be concerned
about generalization, wondering if their research will generalize to people who are not
college students. And researchers who study the behaviors of employees in one company
may wonder whether the same findings would translate to other companies. Whenever there
is reason to suspect that a result found for one sample of participants would not hold
up for another sample, then research may be conducted with these other populations to
test for generalization.
Recently, many psychologists have been interested in testing hypotheses about the extent
to which a result will replicate across people from different cultures. For instance, a
researcher might test whether the effects on aggression of viewing violent video games
are the same for Japanese children as they are for American children by showing violent
and nonviolent films to a sample of both Japanese and American schoolchildren. If the
results are the same in both cultures, then we say that the results have generalized,
but if they are different, then we have learned a limiting condition
of the effect.
Unless the researcher has a specific reason to believe that generalization will not hold,
it is appropriate to assume that a result found in one population (even if that
population is college students) will generalize to other populations. Because the
investigator can never demonstrate that the research results generalize to all
populations, it is not expected that the researcher will attempt to do so. Rather, the
burden of proof rests on those who claim that a result will not generalize.
Because any single test of a research hypothesis will always be limited in terms of what
it can show, important advances in science are never the result of a single research
project. Advances occur through the accumulation of knowledge that comes from many
different tests of the same theory or research hypothesis. These tests are conducted by
different researchers using different research designs, participants, and
operationalizations of the independent and dependent variables. The
process of repeating previous research, which forms the basis of all scientific
inquiry, is known as replication.
learn by doing
Situation 1: A researcher wants to know if creativity can
be taught. She designs a curriculum for teaching creative drawing to elementary
school children. Then (with the permission of parents and the school) she
randomly assigns 30 students to participate in several weekly sessions of
creativity training. Another 30 randomly chosen students participate in a weekly
session where they can draw, but they receive no creativity instruction. At the
end of the six weeks of instruction, she has each child draw a picture. Five
local school art teachers, who are also friends of hers, serve as judges. Each
picture has a label showing whether the child was in the “creative training”
group or the “no creative training” group. The art teacher-judges rate each
picture on a 10-point scale, where 10 means “very high in creativity” and 1
means “very low in creativity.” The results were that the children in the
“creative training” group received an average rating of 8.5 and the children in
the “no creative training” group received an average rating of 4.0. Based on
these results, the researcher claimed that her creativity training curriculum
succeeded in teaching students to be more creative.
Situation 2: A researcher at Harvard University is
interested in how much people enjoy film documentaries. He recruits 40 students
enrolled in the documentary filmmaking program at Harvard. He has each person
watch 5 recently produced documentaries about poverty, pollution, and European
monetary policy. Then the students rated each documentary on a several questions
related to enjoyment (e.g., How much did you enjoy this movie? Would you take a
date to see this movie?). He also had the students watch and rate 5 recently
produced Hollywood action movies. The students rated the documentaries more
enjoyable than the Hollywood action movies. Based on this, the researcher states
that movie producers should move from the “dying art form” of action movies to
the “new wave” of important issue documentaries because people now prefer
documentaries.
Situation 3: The following descriptions are from two actual
research studies. Read both studies and answer the following questions about the
validity of Experiment 1.
Experiment 1: In 1950, the Pepsi Cola Corporation, now
PepsiCo, Inc., conducted the “Pepsi Challenge” by randomly assigning individuals
to taste either Pepsi or Coca-Cola. The researchers labeled the cups with only
an “S” for Pepsi or an “L” for Coca-Cola and asked the participants to rate how
much they liked the beverage. The research showed that participants
overwhelmingly preferred cup S over cup L, and the researchers concluded that
Pepsi was preferred to Coca-Cola.
Experiment 2: In 1983, independent researchers modified
the 1950s study in which randomly assigned participants tasted cola from two
cups, one marked L and the other marked S. The same product (either Pepsi or
Coca-Cola) was placed in both cups. Just as in the 1950s study, the participants
overwhelmingly reported that cup S contained the better-tasting product
regardless of whether cup S contained Pepsi or Coca-Cola.
The researchers then extended their study by conducting another experiment in
which participants were asked their preference for either Pepsi or Coca-Cola.
The participants drank from a Pepsi bottle (which contained Coke) and from a
Coke bottle (which contained Pepsi). The results indicated that the participants
were significantly influenced by the visible label of the product they preferred
and not by taste differences between the two products. The researchers concluded
that a taste comparison of colas should avoid using any type of labels, even
presumably neutral ones like letters of the alphabet, since such labels may have
more powerful influences on product comparisons than taste differences.
References
- Stangor, C.
(2011).
Research Methods for the Behavioral Sciences. Cengage. Mountain View, CA. Edition 4th.
- Rosenthal, R., and Fode, K. L.
(1963).
"The effect of experimenter bias on the performance of the albino
rat." Behavioral Science . Volume 8. Number 3. 183–189 Pages.
Did a Neurological Disorder Cause a Musician to Compose Boléro and an Artist to Paint It 66 Years Later?
In 1986 Anne Adams was working as a cell biologist at the University of Toronto in
Ontario, Canada. She took a leave of absence from her work to care for a sick child, and
while she was away, she completely changed her interests, dropping biology entirely and
turning her attention to art. In 1994 she completed her painting Unravelling Boléro, a translation of Maurice Ravel’s famous orchestral piece,
Boléro, onto canvas. As you can see in the following image,
this artwork is filled with themes of repetition. Each bar of music is represented by a
lacy vertical figure, with the height representing volume, the shape representing note
quality, and the color representing the music’s pitch. Like Ravel’s music (see the
following video), which is a hypnotic melody consisting of two melodial themes repeated
eight times over 340 musical bars, the theme in the painting repeats and builds, leading
to a dramatic change in color from blue to orange and pink, a representation of Boléro’s
sudden and dramatic climax.
 Adams’s depiction of Ravel’s orchestral piece Boléro was painted during the very early phase of her illness in 1994. From Flat World Knowledge, Introduction to Psychology, v1.0: Photo courtesy of New Scientist, http://www.newscientist.com/data/images/ns/cms/dn13599/dn13599-1_567.jpg.
Adams’s depiction of Ravel’s orchestral piece Boléro was painted during the very early phase of her illness in 1994. From Flat World Knowledge, Introduction to Psychology, v1.0: Photo courtesy of New Scientist, http://www.newscientist.com/data/images/ns/cms/dn13599/dn13599-1_567.jpg.
This is a video clip of Maurice Ravel's Boléro composed in 1928 during the early phases of his illness.
Shortly after finishing the painting, Adams began to experience behavioral problems,
including increased difficulty speaking. Neuroimages of Adams’s brain taken during this
time show that regions in the front part of her brain, which are normally associated
with language processing, had begun to deteriorate, while at the same time, regions of
the brain responsible for the integration of information from the five senses were
unusually well developed. [1]
The deterioration of the frontal cortex is a symptom of frontotemporal dementia, a disease associated with changes in artistic and
musical tastes and skills [2] as well as with an
increase in repetitive behaviors. [3]
What Adams did not know as she worked on her painting was that her brain may have been
undergoing the same changes that Ravel’s had undergone 66 years earlier. In fact, it
appears that Ravel may have suffered from the same neurological disorder. Ravel composed
Boléro at age 53, when he himself was beginning to show
behavioral symptoms that interfered with his ability to move and speak. Scientists have
concluded, on the basis of an analysis of his written notes and letters, that Ravel was
also experiencing the effects of frontotemporal dementia. [4] If Adams and Ravel were both affected by
the same disease, it could explain why they both became fascinated with the repetitive
aspects of their arts, and it would present a remarkable example of the influence of our
brains on behavior.
Every behavior begins with biology. Our behaviors, as well as our thoughts and
feelings, are produced by the actions of our brains, nerves, muscles, and glands. In
this unit, we begin our journey into the world of psychology by considering the
biological makeup of the human being, including the most remarkable of human
organs—the brain. We consider the structure of the brain and the methods
psychologists use to study the brain and to understand how it works. Let’s begin by
looking at neurons, which are nerve cells involved with all information processing in
your brain.
A neuron is a cell in the nervous system
whose function it is to receive and transmit information. Amazingly, your
nervous system is composed of more than 100 billion neurons!
As you can see in the following figure, neurons consist of three major parts: a cell
body, or soma, which contains the nucleus of
the cell and keeps the cell alive; a branching, treelike fiber known as the
dendrite, which collects information from
other cells and sends the information to the soma; and a long, segmented
fiber known as the axon, which transmits
information away from the cell body toward other neurons or to the muscles and
glands.
Some neurons have hundreds or even thousands of dendrites, and these dendrites may be
branched to allow the cell to receive information from thousands of other cells. The
axons are also specialized, and some, such as those that send messages from the
spinal cord to the muscles in the hands or feet, may be very long—even up to several
feet in length. To improve the speed of their communication, and to keep their
electrical charges from shorting out with other neurons, axons are often surrounded
by a myelin sheath. The myelin sheath is a layer of fatty tissue surrounding the axon of a neuron that both acts as an
insulator and allows faster transmission of the electrical signal. Axons
branch out toward their ends, and at the tip of each branch is a terminal button.
The nervous system operates using an electrochemical process (see the following video). An
electrical charge moves through the neuron, and chemicals are used to transmit information
between neurons. Within the neuron, when a signal is received by the dendrites, it is
transmitted to the soma in the form of an electrical signal, and if the signal is strong
enough, it may then be passed to the axon and then to the terminal buttons. If the signal
reaches the terminal buttons, they are signaled to emit chemicals known as
neurotransmitters, which communicate with other neurons across the spaces between the cells, known as synapses. You will be
learning more about synapses and why they are important later on in this module.
References
- Seeley, W. W., Matthews, B. R., Crawford, R. K.,
Gorno-Tempini, M. L., Foti, D., Mackenzie, I. R., and Miller, B. L.
(2008).
"“Unravelling Boléro”: Progressive aphasia, transmodal creativity,
and the right posterior neocortex." Brain. Volume 131. Number 1. 39–49
Pages.
- Miller, B. L., Boone, K., Cummings, J. L.,
Read, S. L., and Mishkin, F.
(2000).
"Functional correlates of musical and visual ability in
frontotemporal dementia." Journal of Psychiatry. Volume 176. Number 5.
458–463 Pages.
- Aldhous, P.
(2008).
“Boléro”: Beautiful symptom of a terrible disease. Retrieved from http://www.newscientist.com/article/dn13599-bolero-beautiful-symptom-of-a-terrible-disease.html.
- Amaducci, L., Grassi, E., and Boller, F.
(2002).
"Maurice Ravel and right-hemisphere musical creativity: Influence
of disease on his last musical works?." European Journal of Neurology.
Volume 9. Number 1. 75–82 Pages.
The electrical signal moves through the neuron as a result of changes in the electrical
charge of the axon. Normally, the axon remains in the resting
potential, a state in which the interior of the neuron
contains a greater number of negatively charged ions than does the area outside the
cell. When the segment of the axon that is closest to the cell body is
stimulated by an electrical signal from the dendrites, and if this electrical signal is
strong enough that it passes a certain level or threshold, the cell membrane in this
first segment opens its gates, allowing positively charged sodium ions that were
previously kept out to enter. This change in electrical charge that
occurs in a neuron when a nerve impulse is transmitted is known as the action potential. Once the action potential occurs, the number of
positive ions exceeds the number of negative ions in this segment, and the segment
temporarily becomes positively charged.
As you can see in the following figure, the axon is segmented by a series of breaks
between the sausage-like segments of the myelin sheath. Each of these
gaps is a node of Ranvier. The electrical charge moves
down the axon from segment to segment, in a set of small jumps, moving from node to
node. When the action potential occurs in the first segment of the axon, it quickly
creates a similar change in the next segment, which then stimulates the next segment,
and so forth, as the positive electrical impulse continues all the way down to the end
of the axon. As each new segment becomes positive, the membrane in the prior segment
closes up again, and the segment returns to its negative resting potential. In this way,
the action potential is transmitted along the axon toward the terminal buttons. The
entire response along the length of the axon is very fast—it can happen up to 1,000
times each second.
An important aspect of the action potential is that it operates in an all-or-nothing
manner. What this means is that the neuron either fires completely, such that the action
potential moves all the way down the axon, or it does not fire at all. Thus, neurons can
provide more energy to the neurons down the line by firing faster but not by firing more
strongly. Furthermore, the neuron is prevented from repeated firing by the presence of a
refractory period—a brief time after the firing of the axon in which the axon cannot
fire again because the neuron has not yet returned to its resting potential.
Not only do neural signals travel via electrical charges within the neuron, but they also
travel via chemical transmission between the neurons. As we just learned, neurons are
separated by junction areas known as synapses, areas where the terminal buttons at the
end of the axon of one neuron nearly, but don’t quite, touch the dendrites of another.
The synapses provide a remarkable function because they allow each axon to communicate
with many dendrites in neighboring cells. Because a neuron may have synaptic connections
with thousands of other neurons, the communication links among the neurons in the
nervous system allow for a highly sophisticated communication system.
When the electrical impulse from the action potential reaches the end of the axon, it
signals the terminal buttons to release neurotransmitters into the synapse. A neurotransmitter is a chemical that relays
signals across the synapses between neurons. Neurotransmitters travel across
the synaptic space between the terminal button of one neuron and the dendrites of other
neurons, where they bind to the dendrites in the neighboring neurons. Furthermore,
different terminal buttons release different neurotransmitters, and different dendrites
are particularly sensitive to different neurotransmitters. The dendrites admit the
neurotransmitters only if they are the right shape to fit in the receptor sites on the
receiving neuron. For this reason, the receptor sites and neurotransmitters are often
compared to a lock and key, as shown in the following figure.
To explore the process of neurotransmission, watch this animation.
When neurotransmitters are accepted by the receptors on the receiving neurons, their
effect may be either excitatory (i.e., they make the cell more likely to fire) or
inhibitory (i.e., they make the cell less likely to fire). Furthermore, if the receiving
neuron is able to accept more than one neurotransmitter, it is influenced by the
excitatory and inhibitory processes of each. If the excitatory effects of the
neurotransmitters are greater than the inhibitory influences of the neurotransmitters,
the neuron moves closer to its firing threshold, and if it reaches the threshold, the
action potential and the process of transferring information through the neuron
begins.
Neurotransmitters that are not accepted by the receptor sites must be removed from the
synapse in order for the next potential stimulation of the neuron to happen. This
process occurs in part through the breaking down of the neurotransmitters by enzymes,
and in part through reuptake, a process in
which neurotransmitters that are in the synapse are reabsorbed into the transmitting
terminal buttons, ready to again be released after the neuron fires.
More than 100 chemical substances produced in the body have been identified as
neurotransmitters, and these substances have a wide and profound effect on emotion,
cognition, and behavior. Neurotransmitters regulate our appetite, our memory, our
emotions, as well as our muscle action and movement. And as you can see in the following
table, some neurotransmitters are also associated with psychological and physical
diseases.
Drugs that we might ingest—either for medical reasons or recreationally—can act like
neurotransmitters to influence our thoughts, feelings, and behavior. An agonist is a
drug that has chemical properties similar to a particular neurotransmitter and thus
mimics the effects of the neurotransmitter. When an agonist is ingested, it binds to the
receptor sites in the dendrites to excite the neuron, acting as if more of the
neurotransmitter had been present. As an example, cocaine is an agonist for the
neurotransmitter dopamine. Because dopamine produces feelings of pleasure when it is
released by neurons, cocaine creates similar feelings when it is ingested. An antagonist
is a drug that reduces or stops the normal effects of a neurotransmitter. When an
antagonist is ingested, it binds to the receptor sites in the dendrite, thereby blocking
the neurotransmitter. As an example, the poison curare is an antagonist for the
neurotransmitter acetylcholine. When the poison enters the brain, it binds to the
dendrites, stops communication among the neurons, and usually causes death. Still other
drugs work by blocking the reuptake of the neurotransmitter itself—when reuptake is
reduced by the drug, more neurotransmitter remains in the synapse, increasing its
action.
This video clip shows the role of chemical molecules, called neurotransmitters,
in transmitting messages between neurons.
| The Major Neurotransmitters and Their Functions |
|---|
| From Flat World Knowledge, Introduction to Psychology, v1.0, CC-BY-NC-SA. |
| Neurotransmitter |
Description and Function |
Notes |
| Acetylcholine (ACh) |
A common neurotransmitter used in the spinal cord and motor neurons to stimulate
muscle contractions. It’s also used in the brain to regulate memory, sleeping,
and dreaming. |
Alzheimer’s disease is associated with an undersupply of acetylcholine. Nicotine
is an agonist that acts like acetylcholine. |
| Dopamine |
Involved in movement, motivation, and emotion, dopamine produces feelings of
pleasure when released by the brain’s reward system, and it’s also involved in
learning. |
Schizophrenia is linked to increases in dopamine, whereas Parkinson disease is
linked to reductions in dopamine (and dopamine agonists may be used to treat
it). |
| Endorphins |
Released in response to behaviors such as vigorous exercise, orgasm, and eating
spicy foods. |
Endorphins are natural pain relievers. They are related to the compounds found
in drugs such as opium, morphine, and heroin. The release of endorphins creates
the runner’s high that is experienced after intense physical exertion. |
| GABA (gamma-aminobutyric acid) |
The major inhibitory neurotransmitter in the brain. |
A lack of GABA can lead to involuntary motor actions, including tremors and
seizures. Alcohol stimulates the release of GABA, which inhibits the nervous
system and makes us feel drunk. Low levels of GABA can produce anxiety, and GABA
agonists (tranquilizers) are used to reduce anxiety. |
| Glutamate |
The most common neurotransmitter, it’s released in more than 90% of the brain’s
synapses. Glutamate is found in the food additive MSG (monosodium
glutamate). |
Excess glutamate can cause overstimulation, migraines, and seizures. |
| Serotonin |
Involved in many functions, including mood, appetite, sleep, and
aggression. |
Low levels of serotonin are associated with depression, and some drugs designed
to treat depression (known as selective serotonin reuptake inhibitors, or SSRIs)
serve to prevent serotonin reuptake. |
|
If you were someone who understood brain anatomy and were to look at the brain of an animal
that you had never seen before, you would nevertheless be able to deduce the likely
capacities of the animal because the brains of all animals are much alike in overall
form. In each animal the brain is layered, and the basic structures of the brain are
similar. The innermost structures of the brain—the parts nearest the spinal cord—are the
oldest part of the brain, and these areas carry out the same functions they did for our
distant ancestors. The “old brain” regulates basic survival functions, such as
breathing, moving, resting, and feeding, and creates our experiences of emotion.
Mammals, including humans, have developed further brain layers that provide more
advanced functions—for instance, better memory, more sophisticated social interactions,
and the ability to experience emotions. Humans have a large and highly developed outer
layer known as the cerebral cortex, which makes us particularly adept at these
processes.
The brain stem is the oldest and innermost region of the brain. It controls the most basic functions of life, including breathing,
attention, and motor responses. The brain stem begins where the spinal cord
enters the skull and forms the medulla, the area of the brain stem that controls heart rate and breathing. In many cases,
the medulla alone is sufficient to maintain life—animals that have their brains severed
above the medulla are still able to eat, breathe, and even move. The spherical shape
above the medulla is the pons, a structure in the brain stem that
helps control the movements of the body, playing a particularly
important role in balance and walking. The pons is also important in sleeping,
waking, dreaming, and arousal.
Running through the medulla and the pons is a long, narrow network of neurons known as
the reticular formation. The job of the reticular formation is to
filter out some of the stimuli that are coming into the brain from the spinal cord and
to relay the remainder of the signals to other areas of the brain. The reticular
formation also plays important roles in walking, eating, sexual activity, and sleeping.
When electrical stimulation is applied to the reticular formation of an animal, it
immediately becomes fully awake, and when the reticular formation is severed from the
higher brain regions, the animal falls into a deep coma.
Two structures near the brain stem are also vital for basic survival functions. The thalamus is the egg-shaped structure sitting just above the brain
stem that applies still more filtering to the sensory information
coming from the spinal cord and through the reticular formation, and it relays some
of these remaining signals to the higher brain levels. [1] The thalamus also
receives some of the higher brain’s replies, forwarding them to the medulla and the
cerebellum. The thalamus is also important in sleep because it shuts off incoming
signals from the senses, allowing us to rest.
The cerebellum (literally, “little brain”) consists of two wrinkled ovals
behind the brain stem. It functions to coordinate voluntary
movement. People who have damage to the cerebellum have difficulty walking,
keeping their balance, and holding their hands steady. Consuming alcohol influences the
cerebellum, which is why people who are drunk have difficulty walking in a straight
line. Also, the cerebellum contributes to emotional responses, helps us discriminate
between different sounds and textures, and is important in learning. [2]
References
- Sherman, S. M., and Guillery, R. W.
(2006).
Exploring the Thalamus and Its Role in Cortical Function. MIT Press. Cambridge, MA. Edition 2nd.
- Bower, J. M., and Parsons, J. M.
(2003).
"Rethinking the lesser brain." Scientific American. Volume 289. Number 2. 50–57 Pages.
Whereas the primary function of the brain stem is to regulate the most basic aspects of life,
including motor functions, the limbic system is largely responsible for memory and emotions, including our responses to reward
and punishment. The limbic system is a set of distinct and important brain structures
located beneath and around the thalamus. Limbic system structures interact with the rest
of the brain in complex ways, and they are extremely important for memory and control of
emotional responses. They include the amygdala, the hypothalamus, and the hippocampus,
among other structures.
The amygdala consists of two almond-shaped clusters (amygdala comes from
the Latin word for almond) and is primarily
responsible for regulating our perceptions of and reactions to aggression and
fear. The amygdala has connections to other bodily systems related to fear,
including the sympathetic nervous system (which we will see later is important in fear
responses), facial responses (which perceive and express emotions), the processing of
smells, and the release of neurotransmitters related to stress and aggression. [1] In a 1939 study, Klüver and Bucy [2] damaged the amygdala of an aggressive rhesus monkey. They
found that the once angry animal immediately became passive and no longer responded to
fearful situations with aggressive behavior. Electrical stimulation of the amygdala in
other animals also influences aggression. In addition to helping us experience fear, the
amygdala helps us learn from situations that create fear. When we experience events that
are dangerous, the amygdala stimulates the brain to remember the details of the
situation so that we learn to avoid it in the future. [3]
Located just under the thalamus (hence its name), the hypothalamus is a
brain structure that contains a number of small areas that perform a variety of
functions. Through its many interactions with other parts of the brain, the hypothalamus
helps regulate body temperature, hunger, thirst, and sex drive
and responds to the satisfaction of these needs by creating feelings of
pleasure.
The hippocampus consists of two “horns” that curve back from the amygdala. The
hippocampus is important in storing information in long-term memory. If the hippocampus
is seriously damaged on both sides of the brain, a person may be unable to store new
long-term memories, living instead in a strange world where everything he or she
experiences just fades away, even while older memories from the time before the damage
are untouched.
References
- Best, B.
(2008).
"The amygdala and the emotions." In Anatomy of the Mind (chap. 9).
Retrieved from Welcome to the World of Ben Best:
http://www.newscientist.com/article/dn13599-bolero-beautiful-symptom-of-a-terrible-disease.html.
- Klüver, H., and Bucy, P. C.
(1939).
"Preliminary analysis of functions of the temporal lobes in
monkeys." Archives of Neurology & Psychiatry (Chicago). Volume 42.
979–1000 Pages.
- Sigurdsson, T., Doyère, V., Cain, C. K., and
LeDoux, J. E.
(2007).
"Long-term potentiation in the amygdala: A cellular mechanism of
fear learning and memory." Neuropharmacology. Volume 52. Number 1.
215–227 Pages.
All animals have adapted to their environments by developing abilities that help them
survive. Some animals have hard shells, others run extremely fast, and some have acute
hearing. Human beings do not have any of these particular characteristics, but we do
have one big advantage over other animals—we are very, very smart.
You might think we should be able to determine the intelligence of an animal by looking at the
ratio of the animal’s brain weight to the weight of its entire body. But brain size is
not a measure of intelligence. The elephant’s brain is one-thousandth of its body
weight, but the whale’s brain is only one-ten-thousandth of its body weight. On the
other hand, although the human brain is one-sixtieth of its body weight, the mouse’s
brain represents one fortieth of its body weight. Despite these comparisons, elephants
do not seem 10 times smarter than whales, and humans definitely seem smarter than
mice.
The key to the advanced intelligence of humans is not found in the size of our brains. What
sets humans apart from other animals is our larger cerebral cortex—the outer barklike
layer of our brain that allows us to so successfully use language, acquire complex
skills, create tools, and live in social groups. [1] In humans, the cerebral
cortex is wrinkled and folded rather than smooth, as it is in most other animals. This
creates a much greater surface area and size. and allows increased capacities for
learning, remembering, and thinking. The folding of the cerebral cortex is called corticalization.
Although the cortex is only about one tenth of an inch thick, it makes up more than 80% of the
brain’s weight. The cortex contains about 20 billion nerve cells and 300 trillion
synaptic connections. [2] Supporting all these neurons are billions
more glial cells (glia), cells that surround
and link to the neurons, protecting them, providing them with nutrients, and
absorbing unused neurotransmitters. The glia come in different forms and have
different functions. For instance, the myelin sheath surrounding the axon of many
neurons is a type of glial cell. The glia are essential partners of neurons, without
which the neurons could not survive or function. [3]
The cerebral cortex is divided into two hemispheres, and each hemisphere is divided into four
lobes, each separated by folds known as fissures. If we look at the cortex starting at
the front of the brain and moving over the top, we see first the frontal lobe (behind
the forehead), which is responsible primarily for thinking, planning, memory, and
judgment. Following the frontal lobe is the parietal lobe, which extends from the middle
to the back of the skull and is responsible primarily for processing information about
touch. Then comes the occipital lobe, at the very back of the skull, which processes
visual information. Finally, in front of the occipital lobe (pretty much between the
ears) is the temporal lobe, responsible primarily for hearing and language.
Functions of the Cortex
When the German physicists Gustav Fritsch and Eduard Hitzig (1870/2009) applied mild electric
stimulation to different parts of a dog’s cortex, they discovered that they
could make different parts of the dog’s body move. [4] They also discovered an
important and unexpected principle of brain activity. They found that
stimulating the right side of the brain produced movement in the left side of
the dog’s body, and conversely, stimulating the left brain affected the right
side of the body. This finding follows from a general principle about how the
brain is structured, called contralateral control. The
brain is wired such that in most cases the left hemisphere
receives sensations from and controls the right side of the body, and vice
versa.
Fritsch and Hitzig also found that the movement that followed the brain stimulation occurred
only when they stimulated a specific arch-shaped region that runs across the top
of the brain from ear to ear, just at the front of the parietal lobe. Fritsch
and Hitzig had discovered the motor cortex, the part of the cortex that controls and executes movements
of the body by sending signals to the cerebellum and the spinal cord.
More recently, researchers have mapped the motor cortex even more fully by
providing mild electronic stimulation to different areas of the motor cortex in
fully conscious participants while observing their bodily responses (because the
brain has no sensory receptors, these participants feel no pain). As you can see
in the following figure, this research has revealed that the motor cortex is
specialized for providing control over the body: The parts of the body that
require more precise and finer movements, such as the face and hands, also are
allotted the greatest amount of cortical space.
Just as the motor cortex sends out messages to the specific parts of the body, the somatosensory cortex, an area just behind and parallel to
the motor cortex at the back of the frontal lobe, receives
information from the skin’s sensory receptors and the movements of different
body parts. Again, the more sensitive the body region, the more area is
dedicated to it in the sensory cortex. Our sensitive lips, for example, occupy a
large area in the sensory cortex, as do our fingers and genitals.
Other areas of the cortex process other types of sensory information. The visual cortex is the area located in the occipital lobe (at the very
back of the brain) that processes visual information. If
you were stimulated in the visual cortex, you would see flashes of light or
color, and perhaps you have had the experience of “seeing stars” when you were
hit in or fell on the back of your head. The temporal lobe, located on the lower
side of each hemisphere, contains the auditory cortex,
which is responsible for hearing and language. The
temporal lobe also processes some visual information, providing us with the
ability to name the objects around us. [5]
As you can see in the preceding figure, the motor and sensory areas of the cortex account for
a relatively small part of the total cortex. The remainder of the cortex is made
up of association areas in which sensory and motor information are combined and
associated with our stored knowledge. These association areas are responsible
for most of the things that make human beings seem human—the higher mental
functions, such as learning, thinking, planning, judging, moral reflecting,
figuring, and spatial reasoning.
References
- Gibson, K. R.
(2002).
"Evolution of human intelligence: The roles of brain size and
mental construction." Brain, Behavior and Evolution. Volume 59. Number
1–2. 10–20 Pages.
- de Courten-Myers, G. M.
(1999).
"The human cerebral cortex: Gender differences in structure and
function." Journal of Neuropathology and Experimental Neurology. Volume
58. Number 3. 217–226 Pages.
- Miller, G.
(2005).
"Neuroscience: The dark side of glia." Science. Volume 308. Number 5723. 778–781 Pages.
- Fritsch,
G., and Hitzig, E.
(2009).
"Electric excitability of the cerebrum (Über die Elektrische
erregbarkeit des Grosshirns)." Epilepsy and Behavior. Volume 15. Number
2. 123–130 Pages. (Original work published 1870).
- Martin, A.
(2007).
"The representation of object concepts in the brain." Annual Review of Psychology. Volume 58. 25–45 Pages.
The control of some bodily functions, such as movement, vision, and hearing, is performed in
specific areas of the cortex, and if an area is damaged, the individual will likely lose
the ability to perform the corresponding function. For instance, if an infant suffers
damage to facial recognition areas in the temporal lobe, it is likely that he or she
will never be able to recognize
faces. [1] However, the brain is not
divided in an entirely rigid way. The brain’s neurons have a remarkable capacity to
reorganize and extend themselves to carry out particular functions in response to the
needs of the organism and to repair damage. As a result, the brain constantly creates
new neural communication routes and rewires existing ones. Neuroplasticity is the brain’s ability to change its
structure and function in response to experience or damage. Neuroplasticity
enables us to learn and remember new things and adjust to new experiences.
Our brains are the most “plastic” when we are young children, as it is during this time that we
learn the most about our environment. And neuroplasticity continues to be observed even
in adults. [2] The principles of neuroplasticity help
us understand how our brains develop to reflect our experiences. For instance,
accomplished musicians have a larger auditory cortex compared with the general
population [3] and also require less neural activity to
play their instruments than do
novices. [4] These observations reflect
the changes in the brain that follow our experiences.
Plasticity is also observed when damage occurs to the brain or to parts of the body that are
represented in the motor and sensory cortexes. When a tumor in the left hemisphere of
the brain impairs language, the right hemisphere begins to compensate to help the person
recover the ability to speak. [5] And if a person loses a
finger, the area of the sensory cortex that previously received information from the
missing finger begins to receive input from adjacent fingers, causing the remaining
digits to become more sensitive to touch. [6]
Although neurons cannot repair or regenerate themselves as skin and blood vessels can, new
evidence suggests that the brain can engage in neurogenesis, the forming of new neurons. [7] These new neurons
originate deep in the brain and may then migrate to other brain areas where they form
new connections with other neurons. [8]
This leaves open the possibility that someday scientists might be able to “rebuild”
damaged brains by creating drugs that help grow neurons.
Unique Functions of the Left and Right Hemispheres Using Split-Brain
Patients
We learned that the left hemisphere of the brain primarily senses and controls the motor
movements on the right side of the body, and vice versa. This fact provides an
interesting way to study brain lateralization—the idea that the left and the
right hemispheres of the brain are specialized to perform different functions.
Gazzaniga, Bogen, and Sperry [9] studied a patient, known as W.
J., who had undergone an operation to relieve severe seizures. In this surgery,
the region that normally connects the two halves of the brain and supports
communication between the hemispheres, known as the corpus callosum, is severed.
As a result, the patient essentially becomes a person with two separate brains.
Because the left and right hemispheres are separated, each hemisphere develops a
mind of its own, with its own sensations, concepts, and
motivations. [10]
In their research, Gazzaniga and his colleagues tested the ability of W. J. to recognize and
respond to objects and written passages that were presented to only the left or
to only the right brain hemispheres. The researchers had W. J. look straight
ahead and then flashed, for a fraction of a second, a picture of a geometric
shape to the left of where he was looking. By doing so, they assured
that—because the two hemispheres had been separated—the image of the shape was
experienced only in the right brain hemisphere (remember that sensory input from
the left side of the body is sent to the right side of the brain). Gazzaniga and
his colleagues found that W. J. was able to identify what he had been shown when
he was asked to pick the object from a series of shapes, using his left hand,
but that he could not do so when the object was shown in the right visual field.
Conversely, W. J. could easily read written material presented in the right
visual field (and thus experienced in the left hemisphere) but not when it was
presented in the left visual field.
Visual and Verbal Processing in the Split-Brain Patient
The information presented on the left side of our field of vision is transmitted to
the right brain hemisphere, and vice versa. In split-brain patients, the severed
corpus callosum does not permit information to be transferred between
hemispheres, which allows researchers to learn about the functions of each
hemisphere.
This research, and many other studies following it, demonstrated that the two brain
hemispheres specialize in different abilities. In most people, the ability to
speak, write, and understand language is located in the left hemisphere. This is
why W. J. could read passages that were presented on the right side and thus
transmitted to the left hemisphere, but could not read passages that were only
experienced in the right brain hemisphere. The left hemisphere is also better at
math and at judging time and rhythm. It is also superior in coordinating the
order of complex movements—for example, lip movements needed for speech. The
right hemisphere has only limited verbal abilities, and yet it excels in
perceptual skills. The right hemisphere is able to recognize objects, including
faces, patterns, and melodies, and it can put a puzzle together or draw a
picture. This is why W. J. could pick out the image when he saw it on the left,
but not the right, visual field.
Although Gazzaniga’s research demonstrated that the brain is in fact lateralized, such that
the two hemispheres specialize in different activities, this does not mean that
when people behave in a certain way or perform a certain activity they are using
only one hemisphere of their brains at a time. That would be drastically
oversimplifying the concept of brain differences. We normally use both
hemispheres at the same time, and the difference between the abilities of the
two hemispheres is not absolute. [11]
References
- Farah, M. J., Rabinowitz, C., Quinn, G. E., and Liu,
G. T.
(2000).
"Early commitment of neural substrates for face recognition."
Cognitive Neuropsychology. Volume 17. Number 1–3. 117–123 Pages.
- Kolb, B., and Fantie, B.
(1989).
Handbook of Clinical Child Neuropsychology.
Chapter Development of the child’s brain and behavior. Plenum Press.
New York. 17–39 Pages. C. R. Reynolds and E. Fletcher-Janzen (Eds.).
- Bengtsson, S. L., Nagy, Z., Skare, S., Forsman,
L., Forssberg, H., and Ullén, F.
(2005).
"Extensive piano practicing has regionally specific effects on
white matter development." Nature Neuroscience. Volume 8. Number 9.
1148–1150 Pages.
- Münte, T. F., Altenmüller, E., and Jäncke, L.
(2002).
"The musician’s brain as a model of neuroplasticity." Nature Reviews Neuroscience. Volume 3. Number 6. 473–478 Pages.
- Thiel, A., Habedank, B., Herholz, K., Kessler, J.,
Winhuisen, L., Haupt, W. F., and Heiss, W. D.
(2006).
"From the left to the right: How the brain compensates progressive
loss of language function." Brain and Language. Volume 98. Number 1.
57–65 Pages.
- Fox, J. L.
(1984).
"The brain’s dynamic way of keeping in touch." Science. Volume 225. Number 4664. 820–821 Pages.
- Van Praag, H., Zhao, X., Gage, F. H., and Gazzaniga, M. S.
(2004).
The Cognitive Neurosciences. Chapter Neurogenesis in the adult mammalian brain. MIT Press. Cambridge, MA. Edition 3. 127–137 Pages. M. S. Gazzaniga (Ed.).
- Gould, E.
(2007).
"How widespread is adult neurogenesis in mammals?." Nature Reviews Neuroscience. Volume 8. Number 6. 481–488 Pages.
- Gazzaniga, M. S., Bogen, J. E., and Sperry, R.
W.
(1965).
"Observations on visual perception after disconnexion of the
cerebral hemispheres in man." Brain. Volume 88. Number 2. 221–236 Pages.
- Gazzaniga, M. S.
(2005).
"Forty-five years of split-brain research and still going strong."
Nature Reviews Neuroscience. Volume 6. Number 8. 653–659 Pages.
- Soroker, N., Kasher, A., Giora, R., Batori, G.,
Corn, C., Gil, M., and Zaidel, E.
(2005).
"Processing of basic speech acts following localized brain damage: A
new light on the neuroanatomy of language." Brain and Cognition. Volume
57. Number 2. 214–217 Pages.
One problem in understanding the brain is that it is difficult to get a good
picture of what is going on inside it. But a variety of empirical methods allow
scientists to look at brains in action, and the means by which to study the
brain have improved dramatically in recent years with the development of new
neuroimaging techniques. In this section, we consider the various techniques
that psychologists use to learn about the brain. Each technique has some
advantages, and when we put them together, we begin to get a relatively good
picture of how the brain functions and which brain structures control which
activities.
Perhaps the most immediate approach to visualizing and understanding the
structure of the brain is to directly analyze the brains of human cadavers. When
Albert Einstein died in 1955, his brain was removed and stored for later
analysis. Researcher Marian Diamond [1] later analyzed a
section of the Einstein’s cortex to investigate its characteristics. Diamond was
interested in the role of glia, and she hypothesized that the ratio of glial
cells to neurons was an important determinant of intelligence. To test this
hypothesis, she compared the ratio of glia to neurons in Einstein’s brain with
the ratio in the preserved brains of 11 more “ordinary” men. However, Diamond
was able to find support for only part of her research hypothesis. Although she
found that Einstein’s brain had relatively more glia in all the areas she
studied than did the control group, the difference was statistically significant
in only one of the areas she tested. Diamond admits a limitation in her study is
that she had only one Einstein to compare with 11 ordinary men.
An advantage of the cadaver approach is that the brains can be fully studied, but
an obvious disadvantage is that the brains are no longer active. In other cases,
however, we can study living brains. The brains of living human beings may be
damaged, for instance, as a result of strokes, falls, automobile accidents,
gunshots, or tumors. These damages are called lesions. In rare circumstances,
brain lesions may be created intentionally through surgery, for example, to
remove brain tumors or (as in split-brain patients) to reduce the effects of
epilepsy. Psychologists also sometimes intentionally create lesions in animals
to study the effects on their behavior. In so doing, they hope to be able to
draw inferences about the likely functions of human brains from the effects of
the lesions in animals.
Lesions allow the scientist to observe any loss of brain function that may occur.
For instance, when an individual suffers a stroke, a blood clot deprives part of
the brain of oxygen, killing the neurons in the area and rendering that area
unable to process information. In some cases, the result of the stroke is a
specific lack of ability. For instance, if the stroke influences the occipital
lobe, then vision may suffer, and if the stroke influences the areas associated
with language or speech, these functions will suffer. In fact, our earliest
understanding of the specific areas involved in speech and language were gained
by studying patients who had experienced strokes.
It is now known that a good part of our social decision-making abilities are
located in the frontal lobe, and at least some of this understanding comes from
lesion studies. For instance, consider the well-known case of Phineas Gage, a
25-year-old railroad worker who, as a result of an explosion in 1848, had an
iron rod driven into his right cheek and out through the top of his skull,
causing major damage to his frontal lobe. [2] Remarkably, Gage was
able to return to work after the wounds healed, but he no longer seemed to be
the same person to those who knew him. The amiable, soft-spoken Gage had become
irritable, rude, irresponsible, and dishonest. Although there are questions
about the interpretation of this case study, [3] it did provide
early evidence that the frontal lobe is involved in personality, emotion,
inhibitory control, and goal-setting abilities.
References
- Diamond, Marian C.
(1999).
Why Einstein’s Brain?. Retrieved from http://www.newhorizons.org/neuro/diamond_einstein.htm.
- Macmillan, M.
(2000).
An Odd Kind of Fame: Stories of Phineas Gage. MIT Press. Cambridge, MA.
- Kotowicz, Z.
(2007).
"The strange case of Phineas Gage." History of the Human Sciences. Volume 20. Number 1. 115–131 Pages.
Lesion studies are done using various neuroimaging methods that can record electrical
activity in the brain, visualize blood flow and areas of brain activity in real time,
provide cross-sectional images, and even provide computer-generated three-dimensional
composites of the brain.
The single-unit recording method, in which a thin microelectrode is surgically inserted
in or near an individual neuron, is used primarily with animals. The microelectrode
records electrical responses or activity of the specific neuron. Research using this
method has found, for instance, that specific neurons, known as feature detectors, in
the visual cortex detect movement, lines, edges, and even faces. [1]
A less invasive electrical method that is used on humans is called the
electroencephalograph (EEG). The EEG is an instrument that records the electrical
activity produced by the brain’s neurons through the use of electrodes placed on the
surface of the research participant’s head. An EEG can show if a person is asleep,
awake, or anesthetized because the brain wave patterns are known to differ during each
state. EEGs can also track the waves that are produced when a person is reading,
writing, and speaking and are useful for understanding brain abnormalities, such as
epilepsy. A particular advantage of EEG is that the participant can move around while
the recordings are being taken, which is useful when measuring brain activity in
children who often have difficulty keeping still. Furthermore, by following electrical
impulses across the surface of the brain, researchers can observe changes over very
short time periods (microseconds).
Although the EEG can provide information about the general patterns of electrical
activity within the brain, and although the EEG allows the researcher to see these
changes quickly as they occur in real time, the electrodes must be placed on the surface
of the skull, and each electrode measures brain waves from large areas of the brain. As
a result, EEGs do not provide a very clear picture of the structure of the brain.
But other methods exist to provide more specific brain images. The positron emission
tomography (PET) scan is an invasive imaging technique that provides color-coded images
of brain activity by tracking the brain’s use of a radioactively tagged compound, such
as glucose, oxygen, or a drug that has been injected into a person’s bloodstream. The
person lies in a PET scanner and performs a mental task, such as recalling a list of
words or solving an arithmetic problem, while the PET scanner tracks the amounts of
radioactive substance that causes metabolic changes in different brain regions as they
are stimulated by a person’s activity. A computer analyzes the data, producing
color-coded images of the brain’s activity. A PET scan can determine levels of activity
when a person is given a task that requires hearing, seeing, speaking, or thinking.
Functional magnetic resonance imaging (fMRI) is a type of brain scan that uses a magnetic
field to create images of brain activity in each brain area. The patient lies on a bed
in a large cylindrical structure containing a very strong magnet. Neurons that are
firing use more oxygen than neurons that are not firing, and the need for oxygen
increases blood flow to the area. The fMRI detects the amount of blood flow in each
brain region and thus is an indicator of neural activity.
Very clear and detailed pictures of brain structures can be produced via fMRI. Often, the
images take the form of cross-sectional “slices” that are obtained as the magnetic field
is passed across the brain. The images of these slices are taken repeatedly and are
superimposed on images of the brain structure itself to show how activity changes in
different brain structures over time. When the research participant is asked to engage
in tasks (e.g., playing a game with another person), the images can show which parts of
the brain are associated with which types of tasks. Another advantage of the fMRI is
that is it noninvasive. The research participant simply enters the machine and the scans
begin.
Although the scanners are expensive, the advantages of fMRI are substantial, and the
machines are now available in many university and hospital settings. fMRI is now the
most commonly used method of learning about brain structure.
References
- Kanwisher, N.
(2000).
"Domain specificity in face perception." Nature Neuroscience. Volume 3. Number 8. 759–763 Pages.
A new approach that is being more frequently implemented to understand brain function,
transcranial magnetic stimulation (TMS), may turn out to be the most useful of all. TMS
is a procedure in which magnetic pulses are applied to the brain of living persons with
the goal of temporarily and safely deactivating a small brain region. In TMS studies,
the research participant is first scanned in an fMRI machine to determine the exact
location of the brain area to be tested. Then the electrical stimulation is provided to
the brain before or while the participant works on a cognitive task, and the effects of
the stimulation on performance are assessed. If the participant’s ability to perform the
task is influenced by the presence of the stimulation, then the researchers can conclude
that this particular area of the brain is important to carrying out the task.
The primary advantage of TMS is that it allows the researcher to draw causal conclusions
about the influence of brain structures on thoughts, feelings, and behaviors. When the
TMS pulses are applied, the brain region becomes less active, and this deactivation is
expected to influence the research participant’s responses. Current research has used
TMS to study the brain areas responsible for emotion and cognition and their roles in
how people perceive intention and approach moral reasoning. [1] [2] [3]
TMS is
also used as a treatment for a variety of conditions, including migraine, Parkinson
disease, and major depressive disorder.
learn by doing
Imagine that you are a brain scientist. In the following scenarios, select the
best method to learn more about the person’s brain and the presenting
problem.
learn by doing
Recall what you learned about the amygdala in the previous module. The amygdala
is a small, almond-shaped group of nuclei found at the base of the temporal
lobe. Research has shown that the amygdala performs a primary role in the
processing and memory of emotional reactions.
Using an fMRI machine, researchers assessed differences in the amygdala activity
of participants when they viewed either expressions on a human face (figure on
the left) or geometric shapes (figure on the right). While each participant was
in the fMRI machine, he or she was told to identify either the two identical
faces or the two identical shapes within a trio. This simple cognitive task was
used to keep the participants’ gaze and attention on either the faces or the
shapes so that the fMRI machine could record the activity of the amygdala in
both conditions (faces or shapes). Then the activity level of the amygdala (its
activation or lack of activation) was compared between the two conditions.
Study the fMRI image above. Using what you have learned about the amygdala and
how the fMRI records activation in the brain, answer the following two
questions.
Research Focus: Cyber-ostracism
Neuroimaging techniques have important implications for understanding human
behavior, including people's responses to others. Naomi Eisenberger and her
colleagues [4] tested the hypothesis that people who were excluded by others
would report emotional distress and that images of their brains would show they
experienced pain in the same part of the brain where physical pain is normally
experienced. The experiment involved 13 participants. Each was placed into an
fMRI brain imaging machine and told that he or she would be playing a computer
cyberball game with two other players who were also in fMRI machines (the two
opponents did not actually exist, and their responses were controlled by the
computer).
Each participant was measured under three different conditions. In the first part
of the experiment, the participants were told that due to technical
difficulties, the link to the other two scanners could not yet be made, and
until the problem was fixed, they could not engage in, but only watch, the game
play. This allowed the researchers to take a baseline fMRI reading. Then, during
a second inclusion scan, the participants played the game, supposedly with two
other players. During this time, the other players threw the ball to the
participants. In the third, exclusion, scan, however, the participants initially
received seven throws from the other two players but were then excluded from the
game because the two players stopped throwing the ball to the participants for
the remainder of the scan (45 throws).
The results of the analyses showed that activity in two areas of the frontal lobe
was significantly greater during the exclusion scan than during the inclusion
scan. Because these brain regions are known from prior research to be active for
individuals who are experiencing physical pain, the results suggest that the
physiological brain responses associated with being socially excluded by others
are similar to brain responses experienced upon physical injury.
Further research [5] [6] has documented that people react to being excluded in a
variety of situations with a variety of emotions and behaviors. People who feel
they are excluded, and even those who observe other people being excluded, not
only experience pain but feel worse about themselves and their relationships
with people more generally, and they may work harder to try to restore their
connections with others.
References
- Kalbe, E., Schlegel, M., Sack, A. T., Nowak, D. A., Dafotakis, M., Bangard, C., et al.
(2010).
"Dissociating cognitive from affective theory of mind: A TMS study." Cortex. Volume 46. Number 6. 769–780 Pages.
- Van den Eynde, F., Claudino, A. M.,
Mogg, A., Horrell, L., Stahl, D., Ribeiro, W., et al.
(2010).
"Repetitive transcranial magnetic stimulation reduces cue-induced
food craving in bulimic disorders." Biological Psychiatry. Volume 67.
Number 8. 793–795 Pages.
- Young, L., Camprodon, J. A., Hauser, M.,
Pascual-Leone, A., and Saxe, R.
(2010).
"Disruption of the right temporoparietal junction with transcranial
magnetic stimulation reduces the role of beliefs in moral judgments."
PNAS Proceedings of the National Academy of Sciences of the United
States of America. Volume 107. Number 15. 6753–6758 Pages.
- Eisenberger, N. I., Lieberman, M. D., and Williams, K. D.
(2003).
"Does rejection hurt? An fMRI study of social exclusion." Science. Volume 302. Number 5643. 290–292 Pages.
- Chen, Z., Williams, K. D., Fitness, J., and
Newton, N. C.
(2008).
"When hurt will not heal: Exploring the capacity to relive social
and physical pain." Psychological Science. Volume 19. Number 8. 789–795
Pages.
- Wesselmann, E. D., Bagg, D., and Williams, K. D.
(2009).
"“I feel your pain”: The effects of observing ostracism on the ostracism
detection system." Journal of Experimental Social Psychology. Volume 45. Number 6. 1308–1311 Pages.
Now that we have considered how individual neurons operate and the roles of the different
brain areas, it is time to ask how the body manages to “put it all together.” How do the
complex activities in the various parts of the brain, the simple all-or-nothing firings
of billions of interconnected neurons, and the various chemical systems within the body,
work together to allow the body to respond to the social environment and engage in
everyday behaviors? In this section, we will see that the complexities of human behavior
are accomplished through the joint actions of electrical and chemical processes in the
nervous system and the endocrine system.
The nervous system, the electrical information highway of the body, is made up of
nerves—bundles of interconnected neurons that fire in synchrony to carry messages. The
central nervous system (CNS) , made up of the brain and spinal
cord, is the major controller of the body’s functions, charged
with interpreting sensory information and responding to it with its own directives. The
CNS interprets information coming in from the senses, formulates an appropriate
reaction, and sends responses to the appropriate system to respond accordingly.
Everything we see, hear, smell, touch, and taste is conveyed to us from our sensory
organs as neural impulses, and each of the commands that the brain sends to the body,
both consciously and unconsciously, travels through this system as well.
Nerves are differentiated according to their function. A sensory neuron
carries information from the sensory receptors, whereas a motor neuron
transmits information to the muscles and glands. An interneuron, which is by far the
most common type of neuron, is located primarily within the CNS and is responsible for
communicating among the neurons. Interneurons allow the brain to combine the multiple
sources of available information to create a coherent picture of the sensory information
being conveyed.
The spinal cord is the long, thin, tubular bundle of nerves and supporting cells that
extends down from the brain. It is the central pathway of information for the body.
Within the spinal cord, ascending tracts of sensory neurons relay sensory information
from the sense organs to the brain while descending tracts of motor neurons relay motor
commands back to the body. When a quicker-than-usual response is required, the spinal
cord can do its own processing, bypassing the brain altogether. A reflex is an
involuntary and nearly instantaneous movement in response to a stimulus. Reflexes are
triggered when sensory information is powerful enough to reach a given threshold and the
interneurons in the spinal cord act to send a message back through the motor neurons
without relaying the information to the brain, as shown in the following figure. When
you touch a hot stove and immediately pull your hand back, or when you fumble your cell
phone and instinctively reach to catch it before it falls, reflexes in your spinal cord
order the appropriate responses before your brain even knows what is happening.
If the central nervous system is the command center of the body, the peripheral nervous system (PNS) represents the front line. The PNS links the CNS to the body’s sense receptors, muscles, and
glands. As you can see in the following figure, the PNS is divided into two
subsystems, one controlling internal responses and one controlling external
responses.
The autonomic nervous system (ANS) is the division of the PNS that
governs the internal activities of the human body, including
heart rate, breathing, digestion, salivation, perspiration, urination, and sexual
arousal. Many of the actions of the ANS, such as heart rate and digestion, are
automatic and out of our conscious control, but others, such as breathing and sexual
activity, can be controlled and influenced by conscious processes.
The somatic nervous system (SNS) is the division of the PNS that
controls the external aspects of the body, including the skeletal
muscles, skin, and sense organs. The somatic nervous system consists primarily
of motor nerves responsible for sending brain signals for muscle contraction.
The autonomic nervous system itself can be further subdivided into the sympathetic and
parasympathetic systems (see figure below). The sympathetic division of
the ANS is involved in preparing the body for rapid action
in response to stress from threats or emergencies by activating the organs and
glands in the endocrine system. When the sympathetic nervous system recognizes danger or
a threat, the heart beats faster, breathing accelerates, and lungs and bronchial tubes
expand. These physiological responses increase the amount of oxygen to the brain and
muscles to prepare your body for defense. In other sympathetic nervous system responses,
your pupils dilate to increase your field of vision, salivation stops and your mouth
becomes dry, digestion stops in your stomach and intestines, and you begin to sweat due
to your body’s use of more energy and heat. These bodily changes collectively represent
the fight-or-flight response, which prepares you to either fight or flee from a
perceived
danger.
The parasympathetic division of the ANS tends to calm the body by slowing the heart and breathing and by allowing the body to
recover from the activities that the sympathetic system causes. The
parasympathetic nervous system acts more slowly than the sympathetic nervous system as
it calms the activated organs and glands of the endocrine system, eventually returning
your body to a normal state, called homeostasis.
Our everyday activities are also controlled by the interaction between the sympathetic
and parasympathetic nervous systems. For example, when we get out of bed in the morning,
we would experience a sharp drop in blood pressure if it were not for the action of the
sympathetic system, which automatically increases blood flow through the body.
Similarly, after we eat a big meal, the parasympathetic system automatically sends more
blood to the stomach and intestines, allowing us to efficiently digest the food. And
perhaps you’ve had the experience of not being at all hungry before a stressful event,
such as a sports game or an exam (when the sympathetic division was primarily in
action), but suddenly finding yourself starved afterward, as the parasympathetic system
takes over. The two systems work together to maintain vital bodily functions, resulting
in homeostasis, the natural balance in the
body’s systems.
As you have seen, the nervous system is divided structurally into the central nervous
system and the peripheral nervous system. The PNS is further divided into subdivisions,
each having a particular function in the nervous system to help regulate the body. In
the following activity, you will learn the function of each of the nervous system
divisions by matching a specific descriptive function with each structure.
learn by doing
Instructions: Read the two scenarios below and answer the
questions for each scenario.
Scenario 1: Susan, a college freshman, is taking college
algebra. She never liked math and fears she will probably not do well in this
first math course. She stays up all night studying for the first exam, and the
next morning, she enters the classroom to take the test. As she sits down and
takes out her pencils, she feels nervous; she begins to sweat, her stomach is
upset, and her heart begins to race.
Scenario 2: As the exam is passed out, Susan takes several
deep breaths and closes her eyes. She visualizes herself confidently taking the
exam and focuses on her breathing and heart rate. She feels her heart and
breathing slow down, and she feels calm and able to focus on answering the
questions on the exam.
The nervous system is designed to protect us from danger through its
interpretation of and reactions to stimuli. But a primary function of the
sympathetic and parasympathetic nervous systems is to interact with the
endocrine system, which secretes chemical messengers called hormones that
influence our emotions and behaviors.
The endocrine system is made up of glands, which are groups of cells that secrete hormones into the
bloodstream. When the hormones released by a gland arrive at receptor
tissues or other glands, these receiving receptors may trigger the release of
other hormones, resulting in a complex chemical chain reaction. The endocrine
system works together with the nervous system to influence many aspects of human
behavior, including growth, reproduction, and metabolism. The endocrine system
also plays a vital role in emotions. Since the glands in men and women differ,
the hormones from each of these glands, the ovaries and testes, explain some of
the observed behavioral differences between men and women. The major glands in
the endocrine system are shown in the figure above.
The secretion of hormones is regulated by the hypothalamus of the brain. The
hypothalamus is the main link between the nervous system and the endocrine
system and directs the release of hormones by its interactions with the
pituitary gland, which is next to and highly interconnected with the
hypothalamus. Review the module "Neurons: The Building Blocks of the Nervous
System" for more information on the hypothalamus. The pituitary gland, a
pea-sized gland, is responsible for controlling the body’s growth, but it also
has many other influences that make it of primary importance to regulating
behavior. The pituitary secretes hormones that influence our responses to pain
as well as hormones that signal the ovaries and testes to make sex hormones. The
pituitary gland also controls ovulation and the menstrual cycle in women.
Because the pituitary has such an important influence on other glands, it is
sometimes known as the “master gland.”
Other glands in the endocrine system include the pancreas, which secretes
hormones designed to keep the body supplied with fuel to produce and maintain
stores of energy; and the pineal gland, located in the middle of the brain,
which secretes melatonin, a hormone that helps regulate the wake-sleep
cycle.
The body has two triangular adrenal glands, one on top of each kidney. The
adrenal glands produce hormones that regulate salt and water balance in the
body, and they are involved in metabolism, the immune system, and sexual
development and function. The most important function of the adrenal glands is
to secrete the hormones epinephrine (also known as adrenaline) and
norepinephrine (also known as noradrenaline) when we are excited, threatened, or
stressed. Epinephrine and norepinephrine stimulate the sympathetic division of
the autonomic nervous system, causing increased heart and lung activity,
dilation of the pupils, and increases in blood sugar, which give the body a
surge of energy to respond to a threat. The activity and role of the adrenal
glands in response to stress provides an excellent example of the close
relationship and interdependency of the nervous and endocrine systems. A
quick-acting nervous system is essential for immediate activation of the adrenal
glands, while the endocrine system mobilizes the body for action.
At this point, you can begin to see the important role the hormones play in
behavior. But the hormones we reviewed in this section represent only a subset
of the many influences that hormones have on our behaviors. In the upcoming
units, we consider the important roles that hormones play in many other
behaviors, including sleeping, sexual activity, and helping and harming
others.
learn by doing
Instructions: In the following vignette, you will
apply what you have learned about how the electrical components of the
nervous system and the chemical components of the endocrine system work
together to influence our behavior. Read the vignette and choose the
best answers to complete the sentences describing the correct
interaction of the nervous system and endocrine system.
Larry and Claire are hiking on a trail in the Rocky Mountains. As they
walk, the trail becomes less distinguishable and is overgrown with
brush. Suddenly, a man holding an axe jumps in front of them. This
scares both of them; their hearts begin to pump faster and their
breathing increases. They begin running in the opposite direction to get
away from the man.
As Larry and Claire begin to run, they hear the man calling them. He
yells, “Wait! I didn’t mean to scare you. I am a forest ranger, trying
the clear part of this trail. Please don’t run away.” Larry and Claire
stop running and turn around to look at the man. They notice that he is
dressed in a typical forest ranger uniform and see his identification
badge. Not feeling threatened any longer, both Larry and Claire begin to
feel “calmed down” and walk back toward the forest ranger to resume
their hike on the trail.
Misperception by Those Trained to Accurately Perceive a Threat
On September 6, 2007, the Asia-Pacific Economic Cooperation (APEC) leaders’ summit was being
held in downtown Sydney, Australia. World leaders, including then U.S. president,
George W. Bush, were attending the summit. Many roads in the area were closed for
security reasons, and police presence was high.
As a prank, eight members of the Australian television satire The
Chaser’s War on Everything assembled a false motorcade made up of two black
four-wheel-drive vehicles, a black sedan, two motorcycles, body guards, and
chauffeurs (see the video below). Group member Chas Licciardello was in one of the
cars disguised as Osama bin Laden. The motorcade drove through Sydney’s central
business district and entered the security zone of the meeting. The motorcade was
waved on by police, through two checkpoints, until the Chaser group decided it had
taken the gag far enough and stopped outside the InterContinental Hotel where former
President Bush was staying. Licciardello stepped out onto the street and complained,
in character as bin Laden, about not being invited to the APEC Summit. Only at this
time did the police belatedly check the identity of the group members, finally
arresting them.
Motorcade Stunt performed by the Chaser pranksters in 2007.
Afterward, the group testified that it had made little effort to disguise its attempt as
anything more than a prank. The group’s only realistic attempt to fool police was
its Canadian flag–marked vehicles. Other than that, the group used obviously fake
credentials, and its security passes were printed with “JOKE,” “Insecurity,” and
“It’s pretty obvious this isn’t a real pass,” all clearly visible to any police
officer who might have been troubled to look closely as the motorcade passed. The
required APEC 2007 Official Vehicle stickers had the name of the group’s show
printed on them, and this text: “This dude likes trees and poetry and certain types
of carnivorous plants excite him.” In addition, a few of the “bodyguards” were
carrying camcorders, and one of the motorcyclists was dressed in jeans, both details
that should have alerted police that something was amiss.
The Chaser pranksters later explained the primary reason for the stunt. They wanted
to make a statement about the fact that bin Laden, a world leader, had not been
invited to an APEC Summit where issues of terror were being discussed. The secondary
motive was to test the event’s security. The show’s lawyers approved the stunt,
under the assumption that the motorcade would be stopped at the APEC meeting.
The senses provide our brains with information about the outside world and about
our own internal world. Even single-celled organisms have ways to detect facts
about their environment and they typically have the ability to use this
information either to find nutrients or to avoid danger. For more complex
organisms, certainly for humans, many sources of information about the external
and internal world are necessary to allow us to survive and thrive. The systems we have throughout our bodies that allow us to detect
information and transform energy into neural impulses are called the
senses or sensory systems.
Detection of food or danger is generally not enough to permit an organism to
respond effectively for survival. The world is full of complex stimuli that must
be responded to in different ways. Organisms generally use
both genetically transmitted knowledge and knowledge derived from experience
to organize and interpret incoming sensory information. This process of organization and interpretation is what we
refer to as perception.
In this unit we discuss the strengths and limitations of these capacities, focusing on both
sensation—awareness resulting from the stimulation of a sense organ, and
perception—the organization and interpretation of sensations. Sensation and
perception work seamlessly together to allow us to experience the world through
our eyes, ears, nose, tongue, and skin, but also to combine what we are
currently learning from the environment with what we already know about it to
make judgments and to choose appropriate behaviors.
The study of sensation and perception is exceedingly important for our everyday lives because
the knowledge generated by psychologists is used in so many ways to help so many
people. Psychologists work closely with mechanical and electrical engineers,
with experts in defense and military contractors, and with clinical, health, and
sports psychologists to help them apply this knowledge to their everyday
practices. The research is used to help us understand and better prepare people
to cope with such diverse events as driving cars, flying planes, creating
robots, and managing pain. [1]
We begin the unit with a focus on the six senses of seeing, hearing, smelling, touching,
tasting, and monitoring the body’s positions, also called proprioception. We
will see that sensation is sometimes relatively direct, in the sense that the
wide variety of stimuli around us inform and guide our behaviors quickly and
accurately, but nevertheless is always the result of at least some
interpretation. We do not directly experience stimuli, but rather we experience
those stimuli as they are created by our senses. Each sense accomplishes the
basic process of transduction—the
conversion of stimuli detected by receptor cells to electrical impulses that
are then transported to the brain—in different but related ways.
Each of your sense organs is a specialized system for detecting energy in the external
environment and initiating neural messages—action potentials—to send information
to the brain about the strength and other characteristics of the detected
stimulus. For example, the eyes detect photons (individual units of light) and
photosensitive (light sensitive) cells in the back of the eye react to the
photons by sending an action potential down a series of neurons all the way to
the occipital cortex in the back of the brain. Each of the senses has a specific
place in the brain where information from that particular sense is processed.
Very often, the information from these sense-specific brain areas is then sent
to other parts of the brain for further analysis and integration with
information with other senses. The result is your experience of a rich and
constantly changing multisensory world, full of sights, sounds, smells, tastes,
and texture.
After we have reviewed the basic processes of sensation, we will turn to the
topic of perception, focusing on how the brain’s processing of sensory
experience allows us to process and organize our experience of the outside
world. However, the perceptual system does more than pass on information to the
brain. Perception involves interpretation and even distortion of the sensory
input. Perceptual illusions, discussed at the end of the unit, allow scientists
to explore the various ways that the brain goes beyond the information that it
receives.
References
- Fajen, B. R., and Warren, W. H.
(2003).
"Behavioral dynamics of steering, obstacle avoidance, and route
selection." Journal of Experimental Psychology: Human Perception and
Performance . Volume 29. Number 2. 343–362 Pages.
What Senses Are There?
Odd as it may seem, there is disagreement about the exact number of senses that we have. No
one questions the fact that seeing uses the visual sensory system and hearing
uses the auditory sensory system. There is some disagreement, however, about how
to categorize the skin senses, which detect pressure and heat and pain, and the
body senses, which tell our brains about body position. For our purposes, we
discuss these senses:
- Vision
- Audition
- Smell (olfaction)
- Taste (gustation)
- Touch
- Balance
What Is Transduction?
Transduction is the process of turning energy detected around us into nerve
impulses. Remember from the brain unit that a nerve impulse is called an action potential, so the result of transduction is
always an action potential along a nerve going to the brain. Even though some
action potentials start in the retina of the eye and other action potentials
start in the cochlea in the inner ear, all action potentials are the same. At
the neural level, there is no difference between an action potential coming from
the eye or the ear or any other sensory system. What makes sensory
experiences different from one another is not the sense organ or the action
potential coming from a sense organ. Sensory experiences differ based on which
brain area interprets the incoming message.
learn by doing
In the list below, for each of the senses, pick the type of signal that
goes along the nerve from the sensory receptor on the body to the
brain.
Transduction: Energy Initiates Action Potential
Each of our senses is specialized to detect a certain kind of energy and then to
send a message to the brain in the form of action potentials in nerves that run
from the sense receptor to specific parts of the brain. Let’s consider what kind
of energy or information each sense receptor picks up:
- Vision detects photons, which are units of light.
- Hearing (audition) detects pressure waves in the air that we experience as
sound.
- Smell detects molecules floating in the air.
- Taste detects molecules in the substances touching our tongues.
- There are four different kinds of detectors in our skin, but taken together
they detect light pressure (touch), heat (or cold), heavy pressure, and
possible damage (pain).
- We also have several kinds of detectors for how our body is positioned and
how it is moving. We will concentrate here on our sense of balance, which is
detected by fluids in our ears that move in response to gravity.
learn by doing
Now let’s do an exercise to see if this all makes sense (no pun
intended!).
There are three major types of transduction:
-
Photoreaction: Photo means “light,” so one type of transduction is the
reaction of a chemical in a nerve cell. This is the basis of vision.
-
Mechanical Reactions: Physical movement of attachments to some nerve cells or
physical pressure against others starts transduction in three systems:
- Our sense of hearing works by fluids in the inner ear brushing against hair
cells attached to neurons. The movement of the fluid is produced by sound
waves.
- Our sense of balance also works in a very similar way to our sense of
hearing: a gelatin-like mass in the semicircular canals of your inner ear
brush against hair cells attached to neurons.
- Our skin senses have four different kinds of detectors, and three of them
respond to physical pressure. We have a soft touch detectors and strong
pressure detectors. Pain detectors respond to strong and potentially
damaging physical contact. Finally, we have hot/cold detectors that respond
to the temperature.
-
Molecular Reactions: Two of our senses are sensitive to molecules in the world
around us.
- Our sense of taste is based on taste buds on our tongue that respond to molecules in the
substances that touch the tongue. The taste buds also sort the molecules
into different types, giving us the variety—like sweetness and
bitterness—that we are able to taste.
- Our sense of smell is based on specialized detectors in our nasal cavity
that detect different kinds of molecules floating in the air. Like taste,
smell categorizes the molecules into different types to give of the
wonderful range of odors we can detect.
Where Do the Nerves from the Senses Go?
There is no difference between an action potential coming from one sense (e.g., the eye) and
an action potential coming from a different sense (e.g., the ear). The way your
brain knows if it is processing visual information or sound is by the location
that receives the signal. If the action potential ends in the occipital lobe,
your brain experiences it as visual information. If the action potential ends in
the temporal lobe, then the brain interprets it as sound information.
In Unit 4, Brains, Bodies, and Behavior, you learned that different parts of the brain serve
different functions. Let’s see where in the brain each of the senses sends its
messages. First, all of the senses—except the sense of smell—send action
potentials to the THALAMUS, in the middle of the brain, deep under the cortex.
Then the different senses go to different parts of the brain.
- Visual signals go down the OPTIC NERVE to the THALAMUS and then to the
OCCIPITAL LOBES.
- Sound signals go down the COCHLEAR NERVE to the THALAMUS and then to the
TEMPORAL LOBES.
- Smell signals, the only ones that do not first pass through the thalamus, go
down the OLFACTORY NERVE directly to the LIMBIC SYSTEM under the
cortex.
- Taste signals go down the GUSTATORY NERVE to the THALAMUS and then to the
FRONTAL LOBES.
- Skin sensations go down the SENSORY NERVES to the THALAMUS and then to the
PARIETAL LOBES.
- Balance sensations go down the VESTIBULAR NERVE to the THALAMUS and then to
the CEREBELLUM at the rear of the brain.
learn by doing
For this exercise, put together the information you just learned about the pathway from
the sensory sytem to the brain.
To explore the various senses further, go to this website of the BBC (British Broadcasting System) and click
on each of the senses listed.
 Web page from BBC Science.
Web page from BBC Science.
did I get this
For each sensory system, determine
- the type of energy that starts transduction.
- the process that detects this energy to start transduction.
- which of the three types of reaction—photochemical, mechanical, or molecular—the
transduction uses.
- the kind of neural impulse that is produced by transduction.
- the name of the nerve that carries the signal to the brain.
- whether or not the sensory pathway goes through the thalamus.
- the primary brain region that receives the sensory signal.
We Experience Our World Through Sensation
Humans possess powerful sensory capacities that allow us to sense the
kaleidoscope of sights, sounds, smells, and tastes that surround us. Our eyes
detect light energy and our ears pick up sound waves. Our skin senses touch,
pressure, hot, and cold. Our tongues react to the molecules of the foods we eat,
and our noses detect scents in the air. The human perceptual system is wired for
accuracy, and people are exceedingly good at making use of the wide variety of
information available to them. [1]
In many ways our senses are quite remarkable. The human eye can detect the
equivalent of a single candle flame burning 30 miles away and can distinguish
among more than 300,000 different colors. The human ear can detect sounds as low
as 20 hertz (vibrations per second) and as high as 20,000 hertz, and it can hear
the tick of a clock about 20 feet away in a quiet room. We can taste a teaspoon
of sugar dissolved in 2 gallons of water, and we are able to smell one drop of
perfume diffused in a three-room apartment. We can feel the wing of a bee on our
cheek dropped from 1 centimeter above. [2]
Although there is much that we do sense, there is even more that we do not. Dogs,
bats, whales, and some rodents all have much better hearing than we do, and many
animals have a far richer sense of smell. Birds are able to see the ultraviolet
light that we cannot (see the figure below) and can also sense the pull of the
earth’s magnetic field. Cats have an extremely sensitive and sophisticated sense
of touch, and they are able to navigate in complete darkness using their
whiskers. The fact that different organisms have different sensations is part of
their evolutionary adaptation. Each species is adapted to sensing the things
that are most important to them, while being blissfully unaware of the things
that don’t matter.
References
- Stoffregen, T. A., and Bardy, B. G.
(2001).
"On specification and the senses." Behavioral and Brain Sciences. Volume 24. Number 2. 195–261 Pages.
- Galanter, E.
(1989).
New Directions in Psychology. Chapter
Contemporary psychophysics. Holt, Rinehart, & Winston. New York.
Edition 3. R. Brown, E. Galanter, E. H. Hess, and G. Mandler (Eds.).
Psychophysics
Psychophysics is the branch of psychology that
studies the effects of physical stimuli on sensory perceptions and mental
states. The field of psychophysics was founded by the German
psychologist Gustav Fechner (1801–1887), who was the first to study the
relationship between the strength of a stimulus and a person’s ability to detect
the stimulus.
The measurement techniques developed by Fechner and his colleagues are designed in part to
help determine the limits of human sensation. One important criterion is the
ability to detect very faint stimuli. The absolute
threshold of a sensation is the intensity of a
stimulus that allows an organism to just barely detect it.
In a typical psychophysics experiment, an individual is presented with a series of trials in
which a signal is sometimes presented and sometimes not, or in which two stimuli
are presented that are either the same or different. Imagine, for instance, that
you were asked to take a hearing test. On each of the trials, your task is to
indicate either yes if you heard a sound or no if you did not. The signals are
purposefully made to be very faint, making accurate judgments difficult.
The problem for you is that the very faint signals create uncertainty. Because our ears are
constantly sending background information to the brain, you will sometimes think
that you heard a sound when no sound was made, and you will sometimes fail to
detect a sound that was made. Your must determine whether the neural activity
that you are experiencing is due to the background noise alone or is a result of
a signal within the noise.
Signal Detection Analysis
The responses you give on the hearing test can be analyzed using signal detection analysis.
Signal detection analysis is a technique used to determine the ability of the
perceiver to separate true signals from background
noise. [1] [2]
As you can see in the figure below, each judgment trial creates four
possible outcomes: A hit occurs when you, as the
listener, correctly say yes when there was a sound. A false alarm occurs when you respond yes to no signal. In the
other two cases, you respond no—either a miss
(saying no when there was a signal) or a correct
rejection (saying no when there was in fact no signal).
The analysis of the data from a psychophysics experiment creates two
measures. One measure, known as sensitivity,
refers to the true ability of the individual to detect the presence or
absence of signals. People who have better hearing will have higher
sensitivity than will those with poorer hearing. The other measure,
response bias, refers to a behavioral tendency to respond “yes” to the
trials, which is independent of sensitivity.
Imagine for instance that rather than taking a hearing test, you are a
soldier on guard duty, and your job is to detect the very faint sound of
the breaking of a branch that indicates that an enemy is nearby. You can
see that in this case making a false alarm by alerting the other
soldiers to the sound might not be as costly as a miss (a failure to
report the sound), which could be deadly. Therefore, you might well
adopt a very lenient response bias in which whenever you are at all
unsure, you send a warning signal. In this case, your responses may not
be very accurate (your sensitivity may be low because you are making
many false alarms) and yet the extreme response bias can save lives.
Another application of signal detection occurs when medical technicians
study body images for the presence of cancerous tumors. Again, a miss
(in which the technician incorrectly determines that there is no tumor)
can be very costly, but false alarms (referring patients who do not have
tumors to further testing) also have costs. The ultimate decisions that
the technicians make are based on the quality of the signal (clarity of
the image), their experience and training (the ability to recognize
certain shapes and textures of tumors), and their best guesses about the
relative costs of misses versus false alarms.
learn by doing
Signal detection analysis is often used to study ABSOLUTE THRESHOLD—the minimum intensity
at which some sensory system works. In this demonstration, we use signal
detection analysis, but not with absolute threshold, because absolute
threshold is difficult to show under uncontrolled conditions. Instead,
you will simply search for a target from within a field of objects that
makes it hard to find.
You will see a set of blue crosses on a white background. The stimulus will be present for
only 1 second and then it disappears. You must decide if there is a
single blue L among the crosses. For example, here is a screen you might
see for 1 second:
In this case, there is an L-shape in the figure, so you would click on
the YES button. In case you don’t see it, here is where it is:
On other trials, there will be no L-shape, so you click on the NO
button. Here is an example of a screen with no L-shape:
This demonstration takes about a minute—there are 12 trials in total. After each trial, you
will learn if you were correct or incorrect in your decision. Then you
will see your results in a signal detection report.
When you are ready to begin, click the Start button.
Just Noticeable Difference (JND)
Although we have focused to this point on the absolute threshold, a
second important criterion concerns the ability to assess differences
between stimuli. The difference threshold (or just
noticeable difference [JND]), refers to the
change in a stimulus that can just barely be detected by the
organism. The German physiologist Ernst Weber (1795–1878) made
an important discovery about the JND: that the ability to detect
differences depends not so much on the size of the difference but on
the size of the difference in relationship to the absolute size of the
stimulus. Weber’s law maintains that the
just noticeable difference of a stimulus is a constant
proportion of the original intensity of the timulus. As an example,
if you have a cup of coffee that has only a very little bit of sugar in
it (say, 1 teaspoon), adding another teaspoon of sugar will make a big
difference in taste. But if you added that same teaspoon to a cup of coffee
that already had 5 teaspoons of sugar in it, then you probably wouldn’t taste
the difference as much (in fact, according to Weber’s law, you would have to
add 5 more teaspoons to make the same difference in taste).
One interesting application of Weber’s law is in our everyday shopping behavior. Our
tendency to perceive cost differences between products is dependent not
only on the amount of money we will spend or save but also on the amount
of money saved relative to the price of the purchase. I would venture to
say that if you were about to buy a soda or candy bar in a convenience
store and the price of the items ranged from $1 to $3, you would think
that the $3 item cost a lot more than the $1 item. But now imagine that
you were comparing two music systems, one that cost $397 and one that
cost $399. Probably you would think that the cost of the two systems was
about the same even though buying the cheaper one would still save you
$2.
learn by doing
Weber’s law states that our ability to detect the difference between two stimuli is
proportional to the magnitude of the stimuli. This may sound difficult,
but consider this example. Imagine that you have a 1-pound weight in one
hand. I put a 2-pound weight in your other hand. Do you think you could
tell the difference? Probably so. These weights are light (low
magnitude) so a difference of 1 pound is very easily detected. Now I put
a 50-pound weight in one hand and a 51-pound weight in the other hand.
Now do you think you could tell the difference? Probably not. When the
weight is heavy (high magnitude), the 1-pound difference is not so
easily detected.
Weber’s law focuses on one of the oldest variables in psychology, the JND. These letters
stand for just noticeable difference, which is the smallest difference
between two stimuli that you can reliably detect. Using this term,
Weber’s law says that the size of the JND will increase as the magnitude
of the stimulus increases. In the weight example, the JND when you have
a 50-pound weight in your hand is much greater (2 pounds? 5 pounds?
1pounds?) than when you have a 1-pound weight in your hand (1 pound? ½
pound? ¼ pound?).
In this activity, we will try to determine your JND for some visual stimuli. For example,
look at the two colored circles below. Your task is to decide if they
are exactly the same or if they are different from one another. If they
are the same, click the SAME button. If they are different, click the
DIFFERENT button. As soon as you finish a judgment, you will see the
next trial. You will see a total of 24 pairs to judge.
References
- Macmillan, N. A., and Creelman, C. D.
(2005).
Detection Theory: A User’s Guide. Lawrence Erlbaum Associates. Mahwah, NJ. Edition 2.
- Wickens, T. D.
(2002).
Elementary Signal Detection Theory. Oxford University Press. New York.
Whereas other animals rely primarily on hearing, smell, or touch to understand
the world around them, human beings rely in large part on vision. A large part
of our cerebral cortex is devoted to seeing, and we have substantial visual
skills. Seeing begins when light falls on the eyes, initiating the process of
transduction. Once this visual information reaches the visual cortex, it is
processed by a variety of neurons that detect colors, shapes, and motion, and
that create meaningful perceptions out of the incoming stimuli.
The air around us is filled with a sea of electromagnetic
energy—pulses of energy waves that can carry
information from place to place. As you can see in the figure below,
electromagnetic waves vary in their wavelength—the distance between one wave peak and the next wave
peak, with the shortest gamma waves being only a fraction of a
millimeter in length and the longest radio waves being hundreds of kilometers
long. Humans are blind to almost all of this energy—our eyes detect only the
range from about 400 to 700 billionths of a meter, the part of the
electromagnetic spectrum known as the visible spectrum.
As you can see in the above figure, light enters the eye through the cornea, a clear
covering that protects the eye and begins to focus the incoming light. The light then
passes through the pupil, a small opening in the center of the eye. The pupil is
surrounded by the iris, the colored part of the eye that controls the size of the pupil
by constricting or dilating in response to light intensity. When we enter a dark movie
theater on a sunny day, for instance, muscles in the iris open the pupil and allow more
light to enter. Complete adaptation to the dark may take up to 20 minutes.
Behind the pupil is the lens, a structure that focuses the incoming light on the retina,
the layer of tissue at the back of the eye that contains photoreceptor cells. As our
eyes move from near objects to distant objects, a process known as accommodation occurs.
Accommodation is the process of changing
the curvature of the lens to keep the light entering the eye focused on the
retina. Rays from the top of the image strike the bottom of the retina, and
vice versa, and rays from the left side of the image strike the right part of the
retina, and vice versa, causing the image on the retina to be upside down and backward.
Furthermore, the image projected on the retina is flat, and yet our final perception of
the image will be three dimensional.
Accommodation is not always perfect, and in some cases the light hitting the retina is a
bit out of focus. As you can see in the figure below, when the focus is in front of the
retina, we say that the person is nearsighted, and when the focus is behind the retina
we say that the person is farsighted. Eyeglasses and contact lenses correct this problem
by adding another lens in front of the eye. Laser eye surgery corrects the problem by
reshaping the eye's cornea, while another type of surgery involves replacing the eye's
own lens.
The retina contains layers of neurons specialized to respond to light (see the figure
below). As light falls on the retina, it first activates receptor cells known as rods
and cones. The activation of these cells then spreads to the bipolar cells and then to
the ganglion cells, which gather together and converge, like the strands of a rope,
forming the optic nerve. The optic nerve is a collection of millions of ganglion neurons
that sends vast amounts of visual information, via the thalamus, to the brain. Because
the retina and the optic nerve are active processors and analyzers of visual
information, it is not inappropriate to think of these structures as an extension of the
brain itself.
Rods are visual neurons that specialize in detecting black, white, and gray colors. There
are about 120 million rods in each eye. The rods do not provide a lot of detail about
the images we see, but because they are highly sensitive to shorter-waved (darker) and
weak light, they help us see in dim light, for instance, at night. Because the rods are
located primarily around the edges of the retina, they are particularly active in
peripheral vision (when you need to see something at night, try looking away from what
you want to see). Cones are visual neurons that are specialized in detecting fine detail
and colors. The 5 million or so cones in each eye enable us to see in color, but they
operate best in bright light. The cones are located primarily in and around the fovea,
which is the central point of the retina.
To demonstrate the difference between rods and cones in attention to detail, choose a
word in this text and focus on it. Do you notice that the words a few inches to the side
seem more blurred? This is because the word you are focusing on strikes the
detail-oriented cones, while the words surrounding it strike the less-detail-oriented
rods, which are located on the periphery.
As you can see in the figure below, the sensory information received by the retina is
relayed through the thalamus to corresponding areas in the visual cortex, which is
located in the occipital lobe at the back of the brain. (Hint: You can remember that the
occipital lobe processes vision because it starts with the letter O, which is round like
an eye.) Although the principle of contralateral control might lead you to expect that
the left eye would send information to the right brain hemisphere and vice versa, nature
is smarter than that. In fact, the left and right eyes each send information to both the
left and the right hemispheres, and the visual cortex processes each of the cues
separately and in parallel. This is an adaptational advantage to an organism that loses
sight in one eye, because even if only one eye is functional, both hemispheres will
still receive input from it.
learn by doing
Trace the path of visual information through the visual pathway.
The visual cortex is made up of specialized neurons that turn the sensations they receive
from the optic nerve into meaningful images. Because there are no photoreceptor cells at
the place where the optic nerve leaves the retina, a hole or blind spot in our vision is
created (see the figure below). When both of our eyes are open, we don’t experience a
problem because our eyes are constantly moving, and one eye makes up for what the other
eye misses. But the visual system is also designed to deal with this problem if only one
eye is open—the visual cortex simply fills in the small hole in our vision with similar
patterns from the surrounding areas, and we never notice the difference. The ability of
the visual system to cope with the blind spot is another example of how sensation and
perception work together to create meaningful experience.
learn by doing
You can get an idea of the extent of your blind spot (the place where the optic
nerve leaves the retina) by trying this demonstration. Close your left eye and
stare with your right eye at the cross in the diagram. You should be able to see
the elephant image to the right (don’t look at it, just notice that it is
there). If you can’t see the elephant, move closer or farther away until you
can. Now slowly move so that you are closer to the image while you keep looking
at the cross. At one distance (probably a foot or so), the elephant will
completely disappear from view because its image has fallen on the blind
spot.
 From Flat World Knowledge, Introduction to Psychology, v1.0, CC-BY-NC-SA.
From Flat World Knowledge, Introduction to Psychology, v1.0, CC-BY-NC-SA.
Perception is created in part through the simultaneous action of thousands of feature detector neurons—specialized neurons, located
in the visual cortex, that respond to the strength, angles, shapes, edges, and
movements of a visual
stimulus. [1] [2] The feature
detectors work in parallel, each performing a specialized function. When faced with a
red square, for instance, the parallel line feature detectors, the horizontal line
feature detectors, and the red color feature detectors all become activated. This
activation is then passed on to other parts of the visual cortex where other neurons
compare the information supplied by the feature detectors with images stored in memory.
Suddenly, in a flash of recognition, the many neurons fire together, creating the single
image of the red square that we experience. [3]
Some feature detectors are tuned to selectively respond to particularly important
objects, for instance, faces, smiles, and other parts of the
body. [4] [5]
When researchers disrupted face recognition areas of the cortex using the magnetic
pulses of transcranial magnetic stimulation (TMS), people were temporarily unable to
recognize faces, and yet they were still able to recognize
houses. [6] [7]
References
- Kelsey, C. A.
(1997).
The Perception of Visual Information.
Chapter Detection of visual information. Springer Verlag. New York.
Edition 2. Pages. W. R. Hendee and P. N. T. Wells (Eds.).
- Livingstone, M., and Hubel, D.
(1998).
"Segregation of form, color, movement, and depth: Anatomy,
physiology, and perception." Science. Volume 240. Number 4853. 740–749
Pages.
- Rodriguez, E., George, N., Lachaux,
J.-P., Martinerie, J., Renault, B., and Varela, F. J.
(1999).
"Perception’s shadow: Long-distance synchronization of human brain
activity." Nature. Volume 397. Number 6718. 430–433 Pages.
- Downing, P. E., Jiang, Y., Shuman, M., and Kanwisher, N.
(2001).
"A cortical area selective for visual processing of the human body." Science. Volume 293. Number 5539. 2470–2473 Pages.
- Haxby, J. V., Gobbini, M. I., Furey, M. L.,
Ishai, A., Schouten, J. L., and Pietrini, P.
(2001).
"Distributed and overlapping representations of faces and objects
in ventral temporal cortex." Science. Volume 293. Number 5539. 2425–2430
Pages.
- McKone, E., Kanwisher, N., and Duchaine, B.
C.
(2007).
"Can generic expertise explain special processing for faces?."
Trends in Cognitive Sciences. Volume 11. Number 1. 8–15 Pages.
- Pitcher, D., Walsh, V., Yovel, G., and
Duchaine, B.
(2007).
"TMS evidence for the involvement of the right occipital face area
in early face processing." Current Biology. Volume 17. Number 18.
1568–1573 Pages.
It has been estimated that the human visual system can detect and discriminate among 7
million color variations, [1] but these variations are all
created by the combinations of the three primary colors: red, green, and blue. The shade
of a color, known as hue, is conveyed by the wavelength of the light that enters the eye
(we see shorter wavelengths as more blue and longer wavelengths as more red), and we
detect brightness from the intensity or height of the wave (bigger or more intense waves
are perceived as brighter).
References
- Geldard, F. A.
(1972).
The Human Senses. Wiley. New York. Edition 2.
Trichromatic Color Theory
In his important research on color vision, Hermann von Helmholtz (1821–1894)
theorized that color is perceived because the cones in the retina come in three
types. One type of cone reacts primarily to blue light (short wavelengths),
another reacts primarily to green light (medium wavelengths), and a third reacts
primarily to red light (long wavelengths). The visual cortex then detects and
compares the strength of the signals from each of the three types of cones,
creating the experience of color. According to this Young-Helmholtz trichromatic color theory, what
color we see depends on the mix of the signals from the three types of
cones. If the brain is receiving primarily red and blue signals, for
instance, it perceives purple; if it is receiving primarily red and green
signals, it perceives yellow; and if it is receiving messages from all three
types of cones, it perceives white.
The different functions of the three types of cones are apparent in people who
experience colorblindness—the inability to detect either green and/or red
colors. About 1 in 50 people, mostly men, lack functioning in the red- or
green-sensitive cones, leaving them only able to experience either one or two
colors.
Opponent-Process Theory
The trichromatic color theory cannot explain all of human vision, however. For
one, although the color purple does appear to us as a mixing of red and blue,
yellow does not appear to be a mix of red and green. And people with
colorblindness, who cannot see either green or red, nevertheless can still see
yellow. An alternative approach to the Young-Helmholtz theory, known as the opponent-process color theory, proposes that we analyze sensory information not in terms of three colors
but rather in three sets of “opponent colors”: red-green, yellow-blue, and
white-black. Evidence for the opponent-process theory comes from the
fact that some neurons in the retina and in the visual cortex are excited by one
color (e.g., red) but inhibited by another color (e.g., green) as shown in the
following figure.
One example of opponent processing occurs in the experience of an afterimage. If
you stare at the flag on the left side of the figure below for about 30 seconds
(the longer you look, the better the effect), and then move your eyes to the
blank area to the right of it, you will see the afterimage. When we stare at the
green stripes, our green receptors habituate and begin to process less strongly,
whereas the red receptors remain at full strength. When we switch our gaze, we
see primarily the red part of the opponent process. Similar processes create
blue after yellow and white after black.
Watch the video below on aftereffect.
The tricolor and the opponent-process mechanisms work together to produce color
vision. When light rays enter the eye, the red, blue, and green cones on the
retina respond in different degrees, and send different strength signals of red,
blue, and green through the optic nerve. The color signals are then processed
both by the ganglion cells and by the neurons in the visual
cortex. [1]
References
- Gegenfurtner, K. R., and Kiper, D. C.
(2003).
"Color vision." Annual Review of Neuroscience. Volume 26. Number 3. 181–206 Pages.
One of the important processes required in vision is the perception of form.
German psychologists in the 1930s and 1940s, including Max Wertheimer
(1880–1943), Kurt Koffka (1886–1941), and Wolfgang Köhler (1887–1967), argued
that we create forms out of their component sensations based on the idea of the
gestalt, a meaningfully organized whole. The idea of the gestalt is that the
“whole is more than the sum of its parts.” Some examples of how gestalt
principles lead us to see more than what is actually there are summarized in the
following table.
Depth perception is the ability to
perceive three-dimensional space and to accurately judge distance.
Without depth perception, we would be unable to drive a car, thread a needle, or
simply navigate our way around the
supermarket. [1]
Research has found that depth perception is in part based on innate capacities
and in part learned through
experience. [2]
Psychologists Eleanor Gibson and Richard Walk [3] tested the ability to perceive depth in 6- to 14-month-old
infants by placing them on a visual cliff, a mechanism that gives the perception
of a dangerous drop-off, in which infants can be safely tested for their
perception of depth (see video below). The infants were placed on one side of
the “cliff” while their mothers called to them from the other side. Gibson and
Walk found that most infants either crawled away from the cliff or remained on
the board and cried because they wanted to go to their mothers, but the infants
perceived a chasm that they instinctively could not cross. Further research has
found that even very young children who cannot yet crawl are fearful of
heights. [4] On the other hand, studies
have also found that infants improve their hand-eye coordination as they learn
to better grasp objects and as they gain more experience in crawling, indicating
that depth perception is also learned. [5]
Here is a video showing some of the babies in the original study. Notice how the
mothers helped the experimenter to learn what the babies would and would not
do.
Depth perception is the result of our use of depth cues, messages from our bodies
and the external environment that supply us with information about space and
distance. Binocular depth cues are depth cues that are created by retinal image
disparity—that is, the space between our eyes, and thus require the coordination
of both eyes. One outcome of retinal disparity is that the images projected on
each eye are slightly different from each other. The visual cortex automatically
merges the two images into one, enabling us to perceive depth. Three-dimensional
movies make use of retinal disparity by using 3-D glasses that the viewer wears
to create a different image on each eye. The perceptual system quickly, easily,
and unconsciously turns the disparity into three dimensions.
An important binocular depth cue is convergence, the inward turning of our eyes
that is required to focus on objects that are less than about 50 feet away from
us. The visual cortex uses the size of the convergence angle between the eyes to
judge the object’s distance. You will be able to feel your eyes converging if
you slowly bring a finger closer to your nose while continuing to focus on it.
When you close one eye, you no longer feel the tension—convergence is a
binocular depth cue that requires both eyes to work.
The visual system also uses accommodation to help determine depth. As the lens
changes its curvature to focus on distant or close objects, information relayed
from the muscles attached to the lens helps us determine an object’s distance.
Accommodation is only effective at short viewing distances, however, so while it
comes in handy when threading a needle or tying shoelaces, it is far less
effective when driving or playing sports.
Although the best cues to depth occur when both eyes work together, we are able
to see depth even with one eye closed. Monocular depth cues are depth cues that
help us perceive depth using only one
eye. [6] Some of the most important are
summarized in the following table.
References
- Howard, I. P., and Rogers, B. J.
(2001).
Seeing in Depth: Basic Mechanisms, Vol. 1. Porteous. Toronto. Edition 2.
- Witherington, D. C.
(2005).
"The development of prospective grasping control between 5 and 7
months: A longitudinal study." Infancy. Volume 7. Number 2. 143–161
Pages.
- Gibson, E. J., and Walk, R. D.
(1960).
"The “visual cliff”." Scientific American. Volume 206. Number 4. 64–71 Pages.
- Campos, J. J., Langer, A., and Krowitz, A.
(1970).
"Cardiac responses on the visual cliff in prelocomotor human infants." Science. Volume 170. Number 3954. 196–197 Pages.
- Adolph, K. E.
(2000).
"Specificity of learning: Why infants fall over a veritable cliff."
Psychological Science. Volume 11. Number 4. 290–295 Pages.
- Sekuler, R., and Blake, R.
(2006).
Perception. McGraw-Hill. New York. Edition 5.
Creative artists have taken advantage of the cues that the
brain uses to perceive motion, starting in the early days of motion
pictures and continuing to the present with modern computerized visual effects.
The general phenomenon is called apparent motion. One
example of apparent motion can be seen if two bright circles, one on the left of
the screen and the other on the right of the screen, are flashed on and off in
quick succession. At the right speed, your brain creates a
blur that seems to move back and forth between the two circles. This is
called the phi phenomenon. A similar, but different
phenomenon occurs if a series of circles are flashed on and off in sequence,
though the flashing occurs more slowly than in the phi phenomenon. The circle
appears to move from one location to the next, though the connecting blur
associated with the phi phenomenon is not present.
It is not necessary to use circles. Any visual shape can produce apparent
motion. Motion pictures, which use a sequence of still images, each similar to
but slightly different from the one before, to create the experience of smooth
movement. At the frame speeds of modern motion pictures, the phi phenomenon is
the best explanation for our experience of smooth and natural movement. However,
as visual artists discovered more than a century ago, even at slower change
rates, the beta effect can produce the experience of a
moving image.
Like vision and all the other senses, hearing begins with transduction. Sound waves
collected by our ears are converted to neural impulses, which are sent to the brain
where they are integrated with past experience and interpreted as the sounds we
experience. The human ear is sensitive to a wide range of sounds, ranging from the faint
tick of a clock in a nearby room to the roar of a rock band at a nightclub, and we have
the ability to detect very small variations in sound. But the ear is particularly
sensitive to sounds in the same frequency as the human voice. A mother can pick out her
child’s voice from a host of others, and when we pick up the phone we quickly recognize
a familiar voice. In a fraction of a second, our auditory system receives the sound
waves, transmits them to the auditory cortex, compares them to stored knowledge of other
voices, and identifies the identity of the caller.
Sound Waves
Just as the eye detects light waves, the ear detects sound waves. Vibrating
objects (such as the human vocal cords or guitar strings) cause air molecules to
bump into each other and produce sound waves, which travel from their source as
peaks and valleys much like the ripples that expand outward when a stone is
tossed into a pond. Unlike light waves, which can travel in a vacuum, sound
waves are carried within mediums such as air, water, or metal, and it is the
changes in pressure associated with these mediums that the ear detects.
As with light waves, we detect both the wavelength and the amplitude of sound
waves. The wavelength of the sound wave (known as frequency) is measured in
terms of the number of waves that arrive per second and determines our
perception of pitch, the perceived frequency of a sound. Longer sound waves have
lower frequency and produce a lower pitch, whereas shorter waves have higher
frequency and a higher pitch.
The amplitude, or height of the sound wave, determines how much energy it
contains and is perceived as loudness (the degree of sound volume). Larger waves
are perceived as louder. Loudness is measured using the unit of relative
loudness known as the decibel. Zero decibels represents the absolute threshold
for human hearing, below which we cannot hear a sound. Each increase in 10
decibels represents a tenfold increase in the loudness of the sound. This means
that 20 decibels is 10 times louder than 10 decibels, and 30 decibels is 100
times louder (10 X 10) than 10 decibels. The sound of a typical conversation
(about 60 decibels) is 1,000 times louder than the sound of a faint whisper (30
decibels), whereas the sound of a jackhammer (130 decibels) is 10 billion times
louder than the whisper.
Audition begins in the pinna, or auricle, the
external and visible part of the ear, which is shaped like a funnel to
draw in sound waves and guide them into the auditory canal. At the end of the
canal, the sound waves strike the tightly stretched, highly
sensitive membrane known as the tympanic membrane (or
eardrum), which vibrates with the waves. The resulting vibrations are
relayed into the middle ear through three tiny bones,
known as the ossicles—the hammer (or
malleus), anvil (or incus), and stirrup (or stapes)—to the cochlea, a snail-shaped liquid-filled tube in the inner ear. The
vibrations cause the oval window, the membrane covering the opening of the
cochlea, to vibrate, disturbing the fluid inside the cochlea.
The movements of the fluid in the cochlea bend the hair cells of the inner ear,
much in the same way that a gust of wind bends over wheat stalks in a field. The
movements of the hair cells trigger nerve impulses in the attached neurons,
which are sent to the auditory nerve and then to the auditory cortex in the
brain. The cochlea contains about 16,000 hair cells, each of which holds a
bundle of fibers known as cilia on its tip. The cilia are so sensitive that they
can detect a movement that pushes them the width of a single atom. To put things
in perspective, cilia swaying at the width of an atom is equivalent to the tip
of the Eiffel Tower swaying by half an
inch. [1]
learn by doing
Watch the video below, then answer the questions that follow.
Although loudness is directly determined by the number of hair cells that are
vibrating, two different mechanisms are used to detect pitch. The frequency
theory of hearing proposes that whatever the pitch of a sound wave, nerve
impulses of a corresponding frequency will be sent to the auditory nerve. For
example, a tone measuring 600 hertz will be transduced into 600 nerve impulses a
second. This theory has a problem with high-pitched sounds, however, because the
neurons cannot fire fast enough. About 1,000 nerve impulses a second is the
maximum firing rate for the fastest neurons. To reach the necessary speed for
higher frequency (pitch) sounds, the neurons work together in a sort of volley
system in which different neurons fire in sequence, allowing us to detect sounds
up to about 4,000 hertz.
Not only is frequency important, but location is critical as well. The cochlea
relays information about the specific area, or place, in the cochlea that is
most activated by the incoming sound. The place theory of hearing proposes
sounds of different frequencies set off waves in the cochlea that peak at
different locations along the tube that makes up the coclea. Higher tones peak
at areas closest to the opening of the cochlea (near the oval window). Lower
tones peak at areas near the narrow tip of the cochlea, at the opposite end.
Pitch is therefore determined in part by the area of the cochlea where the wave
of energy reaches its maximum point.
Just as having two eyes in slightly different positions allows us to perceive
depth, so the fact that the ears are placed on either side of the head enables
us to benefit from stereophonic, or three-dimensional, hearing. If a sound
occurs on your left side, the left ear will receive the sound slightly sooner
than the right ear, and the sound it receives will be more intense, allowing you
to quickly determine the location of the sound. Although the distance between
our two ears is only about 6 inches, and sound waves travel at 750 miles an
hour, the time and intensity differences are easily
detected. [2] When a sound is
equidistant from both ears, such as when it is directly in front, behind,
beneath or overhead, we have more difficulty pinpointing its location. It is for
this reason that dogs (and people, too) tend to cock their heads when trying to
pinpoint a sound, so that the ears receive slightly different signals.
References
- Corey, D. P., García-Añoveros, J., Holt, J. R.,
Kwan, K. Y., Lin, S.-Y., Vollrath, M. A., Amalfitano, A., et al.
(2004).
"TRPA1 is a candidate for the mechano-sensitive transduction
channel of vertebrate hair cells." Nature. Volume 432. Number 7018.
723–730 Pages.
- Middlebrooks, J. C., and Green, D. M.
(1991).
"Sound localization by human listeners." Annual Review of Psychology. Volume 42. Number 1. 135–159 Pages.
More than 31 million Americans suffer from some kind of hearing impairment. [1] Conductive hearing loss is caused by physical damage to the
ear (such as to the eardrums or ossicles) that reduce the ability of the ear to
transfer vibrations from the outer ear to the inner ear. Sensorineural hearing
loss, which is caused by damage to the cilia or to the auditory nerve, is less
common overall but frequently occurs with age. [2] The cilia
are extremely fragile, and by the time we are 65 years old, we will have lost
40% of them, particularly those that respond to high-pitched sounds. [3]
Prolonged exposure to loud sounds will eventually create sensorineural hearing
loss as the cilia are damaged by the noise. People who constantly operate noisy
machinery without using appropriate ear protection are at high risk of hearing
loss, as are people who listen to loud music on their headphones or who engage
in noisy hobbies, such as hunting or motorcycling. Sounds that are 85 decibels
or more can cause damage to your hearing, particularly if you are exposed to
them repeatedly. Sounds of more than 130 decibels are dangerous even if you are
exposed to them infrequently. People who experience tinnitus (a ringing or a
buzzing sensation) after being exposed to loud sounds have very likely
experienced some damage to their cilia. Taking precautions when being exposed to
loud sound is important, as cilia do not grow back.
While conductive hearing loss can often be improved through hearing aids that
amplify the sound, they are of little help to sensorineural hearing loss. But if
the auditory nerve is still intact, a cochlear implant may be used. A cochlear
implant is a device made up of a series of electrodes that are placed inside the
cochlea. The device serves to bypass the hair cells by stimulating the auditory
nerve cells directly. The latest implants utilize place theory, enabling
different spots on the implant to respond to different levels of pitch. The
cochlear implant can help children hear who would normally be deaf, and if the
device is implanted early enough, these children can frequently learn to speak,
often as well as normal children do. [4] [5]
References
- Kochkin, S.
(2005).
"MarkeTrak VII: Hearing loss population tops 31 million people." Hearing Review. Volume 12. Number 7. 16–29 Pages.
- Tennesen, M.
(2007).
"Gone today, hear tomorrow." New Scientist. Volume 193. Number 2594. 42–45 Pages.
- Chisolm, T. H., Willott, J. F., and Lister, J.
J.
(2003).
"The aging auditory system: Anatomic and physiologic changes and
implications for rehabilitation." International Journal of Audiology.
Volume 42. Number Suppl. 2. 2S3–2S10 Pages.
- Dettman, S. J., Pinder, D., Briggs, R. J. S.,
Dowell, R. C., and Leigh, J. R.
(2007).
"Communication development in children who receive the cochlear
implant younger than 12 months: Risk versus benefits." Ear and Hearing.
Volume 28. Number Suppl. 2. 11S–18S Pages.
- Dorman, M. F., and Wilson, B. S.
(2004).
"The design and function of cochlear implants." American Scientist. Volume 92. Number 5. 436–445 Pages.
Although vision and hearing are by far the most important, human sensation is rounded out
by four other senses, each of which provides an essential avenue to a better
understanding of and response to the world around us. These other senses are touch,
taste, smell, and our sense of body position and movement (proprioception).
Tasting
Taste is important not only because it allows us to enjoy the food we eat, but
even more crucial, because it leads us toward foods that provide energy (sugar,
for instance) and away from foods that could be harmful. Many children are picky
eaters for a reason—they are biologically predisposed to be very careful about
what they eat. Together with the sense of smell, taste helps us maintain
appetite, assess potential dangers (such as the odor of a gas leak or a burning
house), and avoid eating poisonous or spoiled food.
Our ability to taste begins at the taste receptors on the tongue. The tongue
detects six different taste sensations, known respectively as sweet, salty,
sour, bitter, piquancy (spicy), and umami (savory). Umami is a meaty taste
associated with meats, cheeses, soy, seaweed, and mushrooms, and particularly
found in monosodium glutamate (MSG), a popular flavor enhancer. [1] [2]
Our tongues are covered with taste buds, which are designed to sense chemicals in
the mouth. Most taste buds are located in the top outer edges of the tongue, but
there are also receptors at the back of the tongue as well as on the walls of
the mouth and at the back of the throat. As we chew food, it dissolves and
enters the taste buds, triggering nerve impulses that are transmitted to the
brain. [3] Human tongues are covered with 2,000 to
10,000 taste buds, and each bud contains between 50 and 100 taste receptor
cells. Taste buds are activated very quickly; a salty or sweet taste that
touches a taste bud for even one tenth of a second will trigger a neural
impulse. [4] On
average, taste buds live for about 5 days, after which new taste buds are
created to replace them. As we get older, however, the rate of creation
decreases making us less sensitive to taste. This change helps explain why some
foods that seem so unpleasant in childhood are more enjoyable in adulthood.
The area of the sensory cortex that responds to taste is in a very similar
location to the area that responds to smell, a fact that helps explain why the
sense of smell also contributes to our experience of the things we eat. You may
remember having had difficulty tasting food when you had a bad cold, and if you
block your nose and taste slices of raw potato, apple, and parsnip, you will not
be able to taste the differences between them. Our experience of texture in a
food (the way we feel it on our tongues) also influences how we taste it.
Smelling
As we breathe in air through our nostrils, we inhale airborne chemical molecules,
which are detected by the 10 million to 20 million receptor cells embedded in
the olfactory membrane of the upper nasal passage. The olfactory receptor cells
are topped with tentacle-like protrusions that contain receptor proteins. When
an odor receptor is stimulated, the membrane sends neural messages up the
olfactory nerve to the brain.
We have approximately 1,000 types of odor receptor cells, [5] and it is
estimated that we can detect 10,000 different odors. [6] The receptors come in
many different shapes and respond selectively to different smells. Like a lock
and key, different chemical molecules “fit” into different receptor cells, and
odors are detected according to their influence on a combination of receptor
cells. Just as the 10 digits from 0 to 9 can combine in many different ways to
produce an endless array of phone numbers, odor molecules bind to different
combinations of receptors, and these combinations are decoded in the olfactory
cortex. Women tend to have a more acute sense of smell than men. The sense of
smell peaks in early adulthood and then begins a slow decline. By ages 60 to 70,
the sense of smell has become sharply diminished.
References
- Ikeda, K.
(2002).
"[New seasonings]." Chemical Senses. Volume 27. Number 9. 847–849
Pages. Trans. and ed. by Y. Ogiwara and Y. Ninomiya, Journal of the
Chemical Society of Tokyo 30, 820–836. (Original work published 1909)..
- Sugimoto, K., and Ninomiya, Y.
(2005).
"Introductory remarks on umami research: Candidate receptors and
signal transduction mechanisms on umami." Chemical Senses. Volume 30.
Number Suppl. 1. i21–i22 Pages.
- Northcutt, R. G.
(2004).
"Taste buds: Development and evolution." Brain, Behavior and Evolution. Volume 64. Number 3. 198–206 Pages.
- Kelling, S. T., and Halpern, B. P.
(1983).
"Taste flashes: Reaction times, intensity, and quality." Science. Volume 219. Number 4583. 412–414 Pages.
- Bensafi, M., Zelano, C., Johnson, B., Mainland, J., Kahn, R., and Sobel, N.
(2004).
The Cognitive Neurosciences. Chapter Olfaction: From sniff to percept. MIT Press. Cambridge, MA. Edition 3. M. S. Gazzaniga (Ed.).
- Malnic, B., Hirono, J., Sato, T., and Buck, L. B.
(1999).
"Combinatorial receptor codes for odors." Cell. Volume 96. Number 5. 713–723 Pages.
Touching
The sense of touch is essential to human development. Infants thrive when they
are cuddled and attended to, but not if they are deprived of human
contact. [1] [2] [3]
Touch communicates warmth, caring, and support, and is an essential part of the
enjoyment we gain from our social interactions with close
others. [4] [5]
The skin, the largest organ in the body, is the sensory organ for touch. The skin contains a variety
of nerve endings, combinations of which respond to particular types of pressures
and temperatures. When you touch different parts of the body, you will find that
some areas are more ticklish, whereas other areas respond more to pain, cold, or
heat.
The thousands of nerve endings in the skin respond to four basic sensations:
pressure, hot, cold, and pain, but only the sensation of pressure has its own
specialized receptors. Other sensations are created by a combination of the
other four. For instance:
- The experience of a tickle is caused by the stimulation of neighboring
pressure receptors.
- The experience of heat is caused by the stimulation of hot and cold
receptors.
- The experience of itching is caused by repeated stimulation of pain
receptors.
- The experience of wetness is caused by repeated stimulation of cold and
pressure receptors.
Balancing and Tracking Our Body Position
Once the nerve endings receive sensory information, such as pain or heat, the
information travels along sensory pathways to the central nervous system.
Although some sensations may stop at the spinal cord, resulting in a reflex
response, most continue on towards the brain for interpretation. The brain will
then process the information and direct your body to respond based on the
sensory information (i.e., your brain recognizes that you have felt the
sensation of pain when a mosquito bit you and now sends the message to your
muscles to slap your arm).
The skin is important not only in providing information about touch and
temperature but also in proprioception—the ability to sense the position and
movement of our body parts. Proprioception is accomplished by specialized
neurons located in the skin, joints, bones, ears, and tendons, which send
messages about the compression and the contraction of muscles throughout the
body. Without this feedback from our bones and muscles, we would be unable to
play sports, walk, or even stand upright. In fact, learning any new motor skill
involves your proprioceptive sense. Imagine trying to hit a baseball if you had
to watch your feet too? How would you be able to keep your eye on the ball
coming at you? Fortunately, proprioception is automatic in many ways that it
normally operates without us even noticing it.
The ability to keep track of where the body is moving is also provided by the
vestibular system, a set of liquid-filled areas in the inner ear that monitors
the head’s position and movement, maintaining the body’s balance. As you can see
in the figure below, the vestibular system includes the semicircular canals and
the vestibular sacs. These sacs connect the canals with the cochlea. The
semicircular canals sense the rotational movements of the body and the
vestibular sacs sense linear accelerations. The vestibular system sends signals
to the neural structures that control eye movement and to the muscles that keep
the body upright.
learn by doing
Watch the following video on the proprioception and then respond to the
question below.
Experiencing Pain
We do not enjoy it, but the experience of pain is how the body informs us that we
are in danger. The burn when we touch a hot radiator and the sharp stab when we
step on a nail lead us to change our behavior, preventing further damage to our
bodies. People who cannot experience pain are in serious danger of damage from
wounds that others with pain would quickly notice and attend to.
The gate-control theory of pain proposes that pain is determined by the operation
of two types of nerve fibers in the spinal cord. One set of smaller nerve fibers
carries pain from the body to the brain, whereas a second set of larger fibers
is designed to stop or start (as a gate would) the flow of
pain. [6] It is for this reason that
massaging an area where you feel pain may help alleviate it—the massage
activates the large nerve fibers that block the pain signals of the small nerve
fibers. [7]
Experiencing pain is a lot more complicated than simply responding to neural
messages, however. It is also a matter of perception. We feel pain less when we
are busy focusing on a challenging
activity, [8]
which can help explain why sports players may feel their injuries only after the
game. We also feel less pain when we are distracted by
humor. [9] Our
experience of pain is also affected by our expectations and moods. So, for
example, if you were having a bad day and feeling frustrated, stubbing your toe
may feel especially painful. Thankfully, our bodies have a way of dealing with
pain, soothing it by the brain’s release of endorphins, which are natural
hormonal pain killers. The release of endorphins can explain the euphoria
experienced in the running of a
marathon. [10]
References
- Baysinger, C. M., Plubell, P. E., and Harlow, H.
F.
(1973).
"A variable-temperature surrogate mother for studying attachment in
infant monkeys." Behavior Research Methods & Instrumentation.
Volume 5. Number 3. 269–272 Pages.
- Feldman, R.
(2007).
Low-Cost Approaches to Promote Physical and Mental Health: Theory, Research, and Practice.
Chapter Maternal-infant contact and child development: Insights from
the kangaroo intervention. Springer. New York. Edition 3. 323–351 Pages.
L. L’Abate (Ed.).
- Haradon, G., Bascom, B., Dragomir, C., and
Scripcaru, V.
(1994).
"Sensory functions of institutionalized Romanian infants: A pilot
study." Occupational Therapy International. Volume 1. Number 4. 250–260
Pages.
- Field, T., Lasko, D., Mundy, P., Henteleff,
T., Kabat, S., Talpins, S., and Dowling, M.
(1997).
"Brief report: Autistic children’s attentiveness and responsivity
improve after touch therapy." Journal of Autism and Developmental
Disorders. Volume 27. Number 3. 333–338 Pages.
- Keltner, D.
(2009).
Born to Be Good: the Science of a Meaningful Life. Norton. New York.
- Melzack, R., and Wall, P.
(1996).
The Challenge of Pain. Penguin. London.
- Wall, P.
(2000).
Pain: The Science of Suffering. Columbia University Press. New York.
- Bantick, S. J., Wise, R. G., Ploghaus, A.,
Clare, S., Smith, S. M., and Tracey, I.
(2002).
"Imaging how attention modulates pain in humans using functional
MRI." Brain: A Journal of Neurology. Volume 125. Number 2. 310–319
Pages.
- Zweyer, K., Velker, B., and Ruch, W.
(2004).
"Do cheerfulness, exhilaration, and humor production moderate pain
tolerance? A FACS study." Humor: International Journal of Humor
Research. Volume 17. Number 1–2. 85–119 Pages.
- Sternberg, W. F., Bailin, D., Grant, M.,
and Gracely, R. H.
(1998).
"Competition alters the perception of noxious stimuli in male and
female athletes." Pain. Volume 76. Number 1–2. 231–238 Pages.
The eyes, ears, nose, tongue, and skin sense the world around us, and in some cases
perform preliminary information processing on the incoming data. But by and large, we do
not experience sensation—we experience the outcome of perception—the total package that
the brain puts together from the pieces it receives through our senses and that the
brain creates for us to experience. When we look out the window at a view of the
countryside, or when we look at the face of a good friend, we don’t just see a jumble of
colors and shapes—we see, instead, an image of a countryside or an image of a
friend. [1]
Our perception is also influenced by psychological factors such as our belief system and
our expectations. For example, every so often, we may hear of people spotting UFO’s in
the sky, only to discover later that they were hot air balloons or military air craft.
Similarly, some people believe that they have seen images of divinity in unexpected
places, such as the 10 year old who saw the Virgin Mary on his grilled cheese sandwich.
Our beliefs, expectations, and culture therefore influence how we perceive sensory
information.
How the Perceptual System Interprets the Environment
This meaning-making involves the automatic operation of a variety of essential perceptual
processes. One of these is sensory interaction-the working together
of different senses to create experience. Sensory interaction is involved when
taste, smell, and texture combine to create the flavor we experience in food. It is also
involved when we enjoy a movie because of the way the images and the music work
together.
Although you might think that we understand speech only through our sense of hearing, it
turns out that the visual aspect of speech is also important. One example of sensory
interaction is shown in the McGurk effect—an error in perception that occurs when we
misperceive sounds because the audio and visual parts of the speech are mismatched.
learn by doing
The McGurk effect is a great example of sensory interaction, the mixing of
information from more than one sensory system. The McGurk effect is an example
of a phenomenon that does not occur in the natural world, but it still tells us
about normal, natural information processing. In the natural world, what a
person says and how that person’s lips move as he is talking are completely
linked. You cannot move your lips one way and say something that doesn’t conform
to the way your lips move. The closest thing to an exception is ventriloquism,
where a person talks without moving his lips.
The McGurk effect is possible because we can use computer-based video editing to
create an artificial experience. A psychologist can film a person saying various
things, and then separate and recombine sound segments and visual segments. To
keep the experience simple, the McGurk effect is usually created by having a
person say simple nonsense sounds, like /GA/ or /BA/.
Watch the video below. Be sure you follow the instructions of the narrator,
watching the screen when you are instructed to do that and not watching the
screen when you are instructed to close your eyes. As instructed, write down
what you actually hear in each condition. After you have completed this
exercise, we will discuss the results.
See the video below on the McGurk effect:
To fully appreciate the McGurk effect, notice how you make the /BA/ sound. Try
it. You close your lips and then open them to say /BA/. So you close and then
open your air passage at the front of your mouth, at the lips. Now make the /GA/
sound. Notice that you close the air passage at the back of your mouth by
touching the middle of your tongue to the back of your mouth. So /BA/ is made by
closing the front of the air passage and /GA/ is made by closing the back of the
air passage.
And /DA/? Notice that you make the /DA/ sound by putting the tip of your tongue
on the top of your mouth near the middle of the air passage. What you hear is a
compromise: Your ears HEAR a sound made by closing the front of the mouth and
SEE a sound made by closing the back of your mouth, so your brain—your
perceptual system—splits the difference and PERCEIVES a sound made by closing
the middle of the mouth.
What does the McGurk effect tell us about normal processing? This automatic
combination of visual and auditory information is not something that your brain
throws together to make psychologists happy. The McGurk effect tells us that we
always combine visual and auditory information when we are conversing with
another person. Of course, in normal life, both senses tell us the same
story—the mouth is making the movements that really do match the sounds. But
this integration of sound and sight may be very useful in a noisy environment or
if the person speaking doesn’t speak clearly. Our use of visual information
allows us to automatically fill in the gaps, allowing us to perceive what a
persons says more clearly than our auditory system could have done alone.
References
- Goodale, M., and Milner, D.
(2006).
"One brain—Two visual systems." Psychologist. Volume 19. Number 11. 660–663 Pages.
Other examples of sensory interaction include the experience of nausea that can occur
when the sensory information being received from the eyes and the body does not match
information from the vestibular system [1] and synesthesia—an experience in which one sensation (e.g.,
hearing a sound) creates experiences in another (e.g., vision). Most people do
not experience synesthesia, but those who do link their perceptions in unusual ways, for
instance, by experiencing color when they taste a particular food or by hearing sounds
when they see certain objects. [2]
learn by doing
Synesthesia is a phenomenon that has received a lot of attention in recent years.
It occurs when sensory input stimulates both normal sensory experiences as well
as sensory experiences either from a different sense or another dimension of
that same sense. An example of the first type is sound-color synesthesia: Sounds
lead to the perception of those sounds, but also to visual experiences of
colors, almost like fireworks. An example of the second type is number-color
synesthesia: Looking at numbers not only leads to the visual experience of those
numbers, but the numbers are experienced in particular colors, so, for instance,
9 might be red and 5 might be yellow, and so on.
Watch the two videos below and then we will analyze synesthesia more fully.
See the video below on number-color synesthesia:
See the video below on color-sound synesthesia:
References
- Flanagan, M. B., May, J. G., and Dobie, T. G.
(2004).
"The role of vection, eye movements, and postural instability in
the etiology of motion sickness." Journal of Vestibular Research:
Equilibrium and Orientation. Volume 14. Number 4. 335–346 Pages.
- Ramachandran, V. S., Hubbard, E. M., Robertson, L. C., and Sagiv, N.
(2005).
Synesthesia: Perspectives from Cognitive Neuroscience. Chapter The emergence of the human mind: Some clues from synesthesia. Oxford University Press. New York. 147–190 Pages.
Another important perceptual process is selective attention—the
ability to focus on some sensory inputs while tuning out others. View the
videos in the exercise below. You will see how surprisingly little we
notice about things happening right in front of our faces. Perhaps the process of
selective attention can help you see why the security guards completely missed the fact
that the Chaser group’s motorcade was a fake—they focused on some aspects of the
situation, such as the color of the cars and the fact that they were there at all, and
completely ignored others (the details of the security information).
learn by doing
See the video below on selective attention:
In the video below, the researcher who created the gorilla video and used it in
his research, Dan Simons, explains more about his work.
Next, watch the video below with British illusionist Derren Brown demonstrating
how little we actually see.
Now watch this British safe driving advertisement:
Selective attention also allows us to focus on a single talker at a party while ignoring
other conversations that are occurring around us. [1]
Without this automatic selective attention, we’d be unable to focus on the single
conversation we want to hear. However, selective attention is not complete; we also at
the same time monitor what is happening in the channels we are not focusing on. Perhaps
you have had the experience of being at a party and talking to someone in one part of
the room, when suddenly you hear your name being mentioned by someone in another part of
the room. This cocktail party phenomenon shows us that, although selective attention is
limiting what we process, we are nevertheless at the same time doing a lot of
unconscious monitoring of the world around us—you did not know you were attending to the
background sounds of the party, but evidently you were.
References
- Broadbent, D. E.
(1958).
Perception and Communication. Pergamon. New York.
One of the major problems in perception is to ensure that we always perceive the
same object in the same way, despite the fact that the sensations that it
creates on our receptors changes dramatically. The ability to perceive a
stimulus as constant despite changes in sensation is known as perceptual constancy. Consider our image of a door as it swings. When
it is closed, we see it as rectangular, but when it is open, we see only its
edge and it appears as a line. But we never perceive the door as changing shape
as it swings—perceptual mechanisms take care of the problem for us by allowing
us to see a constant shape.
The figure below illustrates this point. In natural circumstances, it never
occurs to us that a door is changing shapes as it opens in front of our eyes. As
the figure shows, the shape that hits the retina undergoes a significant
transformation, but our perceptual system simply interprets it as a rectangular
door that is changing in its orientation to us.
The visual system also corrects for color constancy. Imagine that you are wearing
blue jeans and a bright white t-shirt. When you are outdoors, both colors will
be at their brightest, but you will still perceive the white t-shirt as bright
and the blue jeans as darker. When you go indoors, the light shining on the
clothes will be significantly dimmer, but you will still perceive the t-shirt as
bright. This is because we put colors in context and see that, compared to its
surroundings, the white t-shirt reflects the most light. [1] In
the same way, a green leaf on a cloudy day may reflect the same wavelength of
light as a brown tree branch does on a sunny day. Nevertheless, we still
perceive the leaf as green and the branch as brown.
To see an example of color constancy, look at the picture of the hot air balloon
below. If you were looking at it in a natural setting, not thinking about your
psychology class, you would simply think of the main colors: green, red, white,
and blue. However, our camera allows us to take a picture frozen in time to
analyze. What we can easily see is that the four colors are extremely variable.
Look at the color patches to the right. They are all taken from the three bands
of color-green, white, and blue-in the lower half of the picture. Notice how the
actual hues vary considerably, although we would simply perceive them as the
same color if we were not concentrating on their variability. Color constancy is
produced by your perceptual system, taking sensory input and compensating for
changes in lighting.
A third kind of constancy is size constancy. Our eyes see objects that differ
radically in size, but our perceptual system compensates for this. In the
classroom scene below, notice the huge difference in actual size of people in
the picture as you go from front to back. This is what the retina detects. But
your perceptual system compensates for these differences, using the knowledge
that all of the people are approximately the same size.
Our perceptual system compensates for distance, using depth cues from the space
around objects to help it make adjustments. The figure below shows how physical
context influences our perceptual system. On the left, the monster in front
seems smaller than the one in the back because our perceptual system adjusts the
perceived size to take the distance into the tunnel into account. On the right,
we remove the tunnel, and the two monsters are easily seen as being identical in
size.
learn by doing
Instructions: The image below illustrates the
results of our perceptual system’s attempt to make sense of a complicated
pattern—a pattern designed to fool the perceptual system. This is an example of
color constancy.
Click and drag to move the rows of the figure (marked a through f) around to help you answer these
questions.
learn by doing
Instructions: The picture below is another
illustration of our perceptual system’s attempt to compensate for a
complex world. In this case, it appears that some squares are in a
shadow. Rather than assuming that those squares are actually different
from the rest of the checkerboard, the perceptual system compensates for
the shadow.
Click and drag to move squares A and B around to help you answer these questions.
References
- McCann, J. J.
(1992).
"Rules for color constancy." Ophthalmic and Physiologic Optics. Volume 12. Number 2. 175–177 Pages.
Although our perception is very accurate, it is not perfect. Illusions occur when the
perceptual processes that normally help us correctly perceive the world around us are
fooled by a particular situation so that we see something that does not exist or that is
incorrect. We will look at some perceptual illusions in the exercises below to see what
we can learn from them.
learn by doing
Instructions: For the figures below, adjust the length of
the center bar on the top figure so it looks to you to be the same length as the
middle bar in the lower figure. Simply rely on what your perceptual system tells
you looks equal. Don’t try to compensate for any illusions or use a straightedge
to help you make the judgement. Just use your visual system.
The figures you just worked with form the Mueller-Lyer illusion (see also the
figure below). The middle line on the figure with the arrows pointing in (
>--< ) looks longer to most people than the middle line on the one with
the arrows pointing out (<-->) when they are both actually the same
length.
Many psychologists believe that this illusion is, in part, the result of the way
we interpret the angled lines at the ends of the figure. Based on our experience
with rooms (see figure below), when we see lines pointing out away from the
center line (building on the left), we tend to interpret that as meaning that
the center line is close to us and the angled lines are going away into the
distance. But when the angled lines on the end point in toward the center line
(room interior on the right), we interpret that as meaning that the center line
is far away and the angled lines are coming toward us. Our perceptual system
then compensates for these assumptions and gives us the experience of perceiving
the “more distant line” (the one on the right) as being longer than it really
is.

The moon illusion refers to the fact that the moon is perceived to be
about 50% larger when it is near the horizon than when it is seen
overhead, despite the fact that both moons are the same size and cast
the same size retinal image. The monocular depth cues of position and
aerial perspective create the illusion that things
that are lower and more hazy are farther away. The skyline of the
horizon (trees, clouds, outlines of buildings) also gives a cue that the
moon is far away, compared to a moon at its zenith. If we look at a
horizon moon through a tube of rolled up paper, taking away the
surrounding horizon cues, the moon will immediately appear smaller.
learn by doing
The Moon Illusion
The moon always looks larger on the horizon than when it is high
above. But if we take away the surrounding distance cues of the
horizon, the illusion disappears. It seems that the long
curvature of the earth on the horizon makes the moon, by
comparison, look smaller. It appears that our perceptual system
compares the curvature of the moon to the curvature of the earth
and then exaggerates the smaller curvature of the moon to make
it seem even smaller. Without those cues, when the moon is high
in the sky, the perceptual system no longer exaggerates the
moon’s relatively small size.
 From Flat World Knowledge Introduction to Psychology, v1.0: © Thinkstock.
From Flat World Knowledge Introduction to Psychology, v1.0: © Thinkstock.
We can’t create the moon illusion in this course, but a similar
illusion is one called the Ebbinhaus illusion.
Instructions: Adjust the two center circles
so that they appear to you to be the same size. Don’t use any
aids to measure the size or try to compensate for the illusion.
Rely on your visual system.
learn by doing
Instructions: Adjust the horizontal black lines in the
figure below until they appear to be straight. Do not try to compensate for any
illusion.
learn by doing
The figure below is called the Wundt illusion after its creator, 19th-century
German psychologist Wilhelm Wundt.
 Courtesy of Fibonacci, Wundt Illusion, CC-BY-SA.
Courtesy of Fibonacci, Wundt Illusion, CC-BY-SA.
learn by doing
The Ponzo illusion operates on the same principle. The
monocular depth cue of linear perspective leads us to believe that,
given two similar objects, the distant one can only cast the same size
retinal image as the closer object if it is larger. The topmost bar
therefore appears longer.
The Ponzo illusion is caused by a failure of the monocular depth cue of
linear perspective: Both bars are the same size even though the top one
looks larger.
Instructions: In the figure above, the bottom
yellow line is fixed. Your task is to adjust the top yellow line until
it LOOKS the same length as the bottom one. Please use only your eyes to
guide your decision. Don’t try to compensate for the illusion. Just
adjust the line until your perceptual system tells you that the lines
look to be the same length.
Illusions demonstrate that our perception of the world around us may be
influenced by our prior knowledge. But the fact that some illusions exist in some cases
does not mean the perceptual system is generally inaccurate—in fact, humans normally
become so closely in touch with their environment that the physical body and the
particular environment we sense and perceive become embodied—that is, built into and
linked with—our cognition, such that the worlds around us become part of our brain. [1] The close relationship
between people and their environments means that, although illusions can be created in
the lab and under some unique situations, they may be less common with active observers
in the real world. [2]
Here is a great spot to see many more illusions and to learn more about why they occur.
A Google image search will also turn up interesting illusions.
References
- Calvo, P., and Gomila, T.
(2008).
Handbook of Cognitive Science: An Embodied Approach. Elsevier. San Diego.
- Runeson, S.
(1988).
"The distorted room illusion, equivalent configurations, and the
specificity of static optic arrays." Journal of Experimental Psychology:
Human Perception and Performance. Volume 14. Number 2. 295–304 Pages.
My Story of Posttraumatic Stress Disorder
It is a continuous challenge living
with post-traumatic stress disorder (PTSD), and I’ve suffered from it for most of my life.
I can look back now and gently laugh at all the people who thought I had the perfect life.
I was young, beautiful, and talented, but unbeknownst to them, I was terrorized by an
undiagnosed debilitating mental illness.
Having been properly diagnosed with PTSD at age
35, I know that there is not one aspect of my life that has gone untouched by this mental
illness. My PTSD was triggered by several traumas, most importantly a sexual attack at
knifepoint that left me thinking I would die. I would never be the same after that attack.
For me there was no safe place in the world, not even my home. I went to the police and
filed a report. Rape counselors came to see me while I was in the hospital, but I declined
their help, convinced that I didn’t need it. This would be the most damaging decision of my
life.
For months after the attack, I couldn’t close my eyes without envisioning the face of
my attacker. I suffered horrific flashbacks and nightmares. For four years after the attack
I was unable to sleep alone in my house. I obsessively checked windows, doors, and locks.
By age 17, I’d suffered my first panic attack. Soon I became unable to leave my apartment
for weeks at a time, ending my modeling career abruptly. This just became a way of life.
Years passed when I had few or no symptoms at all, and I led what I thought was a fairly
normal life, just thinking I had a “panic problem.”
Then another traumatic event
retriggered the PTSD. It was as if the past had evaporated, and I was back in the place of
my attack, only now I had uncontrollable thoughts of someone entering my house and harming
my daughter. I saw violent images every time I closed my eyes. I lost all ability to
concentrate or even complete simple tasks. Normally social, I stopped trying to make
friends or get involved in my community. I often felt disoriented, forgetting where, or
who, I was. I would panic on the freeway and became unable to drive, again ending a career.
I felt as if I had completely lost my mind. For a time, I managed to keep it together on
the outside, but then I became unable to leave my house again.
Around this time I was
diagnosed with PTSD. I cannot express to you the enormous relief I felt when I discovered
my condition was real and treatable. I felt safe for the first time in 32 years. Taking
medication and undergoing behavioral therapy marked the turning point in my regaining
control of my life. I’m rebuilding a satisfying career as an artist, and I am enjoying my
life. The world is new to me and not limited by the restrictive vision of anxiety. It
amazes me to think back to what my life was like only a year ago, and just how far I’ve
come. For me there is no cure, no final healing. But there are things I can do to ensure
that I never have to suffer as I did before being diagnosed with PTSD. I’m no longer at the
mercy of my disorder, and I would not be here today had I not had the proper diagnosis and
treatment. The most important thing to know is that it’s never too late to seek help. [1]
In the early part of the 20th century, Russian physiologist Ivan Pavlov (1849–1936)
was studying the digestive system of dogs when he noticed an interesting
behavioral phenomenon: The dogs began to salivate when the lab technicians who normally fed
them entered the room, even though the dogs had not yet received any food. Pavlov realized
that the dogs were salivating because they knew that they were about to be fed; the dogs
had begun to associate the arrival of the technicians with the food that soon followed
their appearance in the room.
With his team of researchers, Pavlov began studying this process in more detail. He
conducted a series of experiments in which, over a number of trials, dogs were exposed to a
sound immediately before receiving food. He systematically controlled the onset of the
sound and the timing of the delivery of the food, and recorded the amount of the dogs’
salivation. Initially the dogs salivated only when they saw or smelled the food, but after
several pairings of the sound and the food, the dogs began to salivate as soon as they
heard the sound. The animals had learned to associate the sound with the food that
followed.
learn by doing
Use the next exercise to sort out the sometimes tricky terminology of classical
conditioning.
In the first step, we focus on the initial conditions before conditioning has taken
place. After looking at the pictures below, determine the unconditioned stimulus and
the unconditioned response that results.
Now you must predict what should happen when a hungry dog is presented with food.
In this step, we find a neutral stimulus—a stimulus that produces no response. After
looking at the pictures below, determine what the neutral stimulus is and the
response that it causes. In this test, the dog is not
hungry.
Now you must predict what should happen when a hungry dog hears the neutral stimulus:
a tone.
In this step, we go through the actual conditioning process, associating a
conditioned stimulus (CS) with an unconditioned stimulus (US). When we are finished,
the neutral stimulus (NS) will have become the conditioned stimulus. After looking at
the pictures below, determine the conditioned and unconditioned stimuli and the
unconditioned response that they cause. Note that this sequence differs from the
first one you did because there are always two stimuli present: first a CS and then a
US.
This is the last part of this exercise. We want to see if conditioning—associative
learning—has taken place. In the previous exercise, the US was always present, so it
could produce the UR. Now we remove the US to see if the animal has learned to
produce the same response when only the CS is present. If so, we will rename the
response, when produced only by the CS, the Conditioned Response (CR). After looking
at the pictures below, determine what the conditioned stimulus is and the conditioned
response that it causes.
This exercise is best understood related to the previous exercise on learning.
Imagine a series of learning trials in which the CS is followed by the US, and the UR
is measured. Now, in this exercise, suppose on the next trial, we present only the CS
without the US. What happens? So in Trial 1 we pair the CS and US only one time
before presenting the CS alone. In Trial 2 we pair the CS and US two times before
presenting the CS alone. In Trial 3 we pair the CS and US three times before
presenting the CS alone.
Pavlov identified a fundamental associative learning process called classical conditioning.
Classical conditioning refers to learning that
occurs when a neutral stimulus (e.g., a tone) becomes associated with a stimulus (e.g.,
food) that naturally produces a specific behavior. After the association is
learned, the previously neutral stimulus is sufficient to produce the behavior. As you can
see in the following figure, psychologists use
specific terms to identify the stimuli and the responses in classical conditioning. The unconditioned stimulus (US) is something (such as
food) that triggers a natural occurring response, and the unconditioned response (UR) is the naturally occurring response
(such as salivation) that follows the unconditioned stimulus. The conditioned stimulus (CS) is a neutral stimulus that, after
being repeatedly presented prior to the unconditioned stimulus, evokes a response
similar to the response to the unconditioned stimulus. In Pavlov’s experiment, the
sound of the tone served as the conditioned stimulus that, after learning, produced the
conditioned response (CR), which is the acquired response to the formerly neutral stimulus.
Note that the UR and the CR are the same behavior—in this case salivation—but they are
given different names because they are produced by different stimuli (the US and the CS,
respectively).
Conditioning is evolutionarily beneficial because it allows organisms to develop
expectations that help them prepare for both good and bad events. Imagine, for instance,
that an animal first smells a new food, eats it, and then gets sick. If the animal can
learn to associate the smell (CS) with the food (US), then it will quickly learn that the
food creates the negative outcome and will not eat it next time.
did I get this
A researcher is testing young children to see if they can learn to associate a red
circle with an event that the child enjoys. She sets up an experiment where a toy
bear dances. The infants predictably love the toy bear and stare at it when it makes
noise and dances. She then trains the child by showing a big red circle on a screen
in front of the child and, immediately after that, the bear appears and dances off to
the side. The bear is only visible right after the red circle appears and the child
must turn his or her head to see the bear.
 Teddy bear photo by falcon1961;
baby photo by Tammra
McCauley, CC-BY-2.0.
Teddy bear photo by falcon1961;
baby photo by Tammra
McCauley, CC-BY-2.0.
References
- Philips, P. K.
(2010).
My story of survival: Battling PTSD.
Anxiety Disorders Association of America. Retrieved from
http://www.adaa.org/living-with-anxiety/personal-stories/my-story-survival-battling-ptsd.
After he had demonstrated that learning could occur through association, Pavlov moved on
to study the variables that influenced the strength and the persistence of conditioning.
In some studies, after the conditioning had taken place, Pavlov presented the sound
repeatedly but without presenting the food afterward.
As you
can see, after the initial acquisition (learning) phase in which the conditioning
occurred, when the CS was then presented alone, the behavior rapidly decreased—the dogs
salivated less and less to the sound, and eventually the sound did not elicit salivation
at all. Extinction is the reduction in
responding that occurs when the conditioned stimulus is presented repeatedly without
the unconditioned stimulus.
Although at the end of the first extinction period the CS was no longer producing
salivation, the effects of conditioning had not entirely disappeared. Pavlov found that,
after a pause, sounding the tone again elicited salivation, although to a lesser extent
than before extinction took place. The increase in responding to the CS following a
pause after extinction is known as spontaneous recovery. When
Pavlov again presented the CS alone, the behavior again showed extinction.
learn by doing
For each example, select the term that best describes
it.
Although the behavior has disappeared, extinction is never complete. If conditioning is
again attempted, the animal will learn the new associations much faster than it did the
first time. Pavlov also experimented with presenting new stimuli that were similar, but
not identical to, the original conditioned stimulus. For instance, if the dog had been
conditioned to being scratched before the food arrived, the stimulus would be changed to
being rubbed rather than scratched. He found that the dogs also salivated upon
experiencing the similar stimulus, a process known as generalization. Generalization refers to the tendency to respond to stimuli that resemble the
original conditioned stimulus. The ability to generalize has important evolutionary
significance. If we eat some red berries and they make us sick, it would be a good idea
to think twice before we eat some purple berries. Although the berries are not exactly
the same, they nevertheless are similar and may have the same negative properties.
Lewicki [1] conducted research that demonstrated the influence of stimulus
generalization and how quickly and easily it can happen. In his experiment, high school
students first had a brief interaction with a female experimenter who had short hair and
glasses. The study was set up so that the students had to ask the experimenter a
question, and (according to random assignment) the experimenter responded either in a
negative way or a neutral way toward the students. Then the students were told to go
into a second room in which two experimenters were present, and to approach either one
of them. However, the researchers arranged it so that one of the two experimenters
looked a lot like the original experimenter, while the other one did not (she had longer
hair and no glasses). The students were significantly more likely to avoid the
experimenter who looked like the earlier experimenter when that experimenter had been
negative to them than when she had treated them more neutrally. The participants showed
stimulus generalization such that the new, similar-looking experimenter created the same
negative response in the participants as had the experimenter in the prior session.
The flip side of generalization is discrimination—the tendency to
respond differently to stimuli that are similar but not identical. Pavlov’s dogs quickly
learned, for example, to salivate when they heard the specific tone that had preceded
food, but not upon hearing similar tones that had never been associated with food.
Discrimination is also useful—if we do try the purple berries, and if they do not make
us sick, we will be able to make the distinction in the future. And we can learn that
although the two people in our class, Courtney and Sarah, may look a lot alike, they are
nevertheless different people with different personalities.
In some cases, an existing conditioned stimulus can serve as an unconditioned stimulus
for a pairing with a new conditioned stimulus—a process known as second-order conditioning. In one of Pavlov’s studies, for instance, he first
conditioned the dogs to salivate to a sound, and then repeatedly paired a new CS, a
black square, with the sound. Eventually he found that the dogs would salivate at the
sight of the black square alone, even though it had never been directly associated with
the food. Secondary conditioners in everyday life include our attractions to things that
stand for or remind us of something else, such as when we feel good on a Friday because
it has become associated with the paycheck that we receive on that day, which itself is
a conditioned stimulus for the pleasures that the paycheck buys us.
References
- Lewicki, P.
(1985).
"Nonconscious biasing effects of single instances on subsequent
judgments." Journal of Personality and Social Psychology. Volume 48.
Number 3. 563–574 Pages.
Scientists associated with the behaviorist school argued that all learning is driven by
experience, and that nature plays no role. Classical conditioning, which is based on
learning through experience, represents an example of the importance of the environment.
But classical conditioning cannot be understood entirely in terms of experience. Nature
also plays a part, as our evolutionary history has made us better able to learn some
associations than others.
Clinical psychologists make use of classical conditioning to explain the learning of a
phobia—a strong and irrational fear of a
specific object, activity, or situation. For example, driving a car is a
neutral event that would not normally elicit a fear response in most people. But if a
person were to experience a panic attack in which he suddenly experienced strong
negative emotions while driving, he may learn to associate driving with the panic
response. The driving has become the CS that now creates the fear response.
Psychologists have also discovered that people do not develop phobias to just anything.
Although people may in some cases develop a driving phobia, they are more likely to
develop phobias toward objects (such as snakes, spiders, heights, and open spaces) that
have been dangerous to people in the past. In modern life, it is rare for humans to be
bitten by spiders or snakes, to fall from trees or buildings, or to be attacked by a
predator in an open area. Being injured while riding in a car or being cut by a knife
are much more likely. But in our evolutionary past, the potential of being bitten by
snakes or spiders, falling out of a tree, or being trapped in an open space were
important evolutionary concerns, and therefore humans are still evolutionarily prepared
to learn these associations over
others. [1] [2]
Another evolutionarily important type of conditioning is conditioning related to food. In
his important research on food conditioning, John Garcia and his
colleagues [3] [4]
attempted to condition rats by presenting either a taste, a sight, or a sound as a
neutral stimulus before the rats were given drugs (the US) that made them nauseous.
Garcia discovered that taste conditioning was extremely powerful—the rat learned to
avoid the taste associated with illness, even if the illness occurred several hours
later. But conditioning the behavioral response of nausea to a sight or a sound was much
more difficult. These results contradicted the idea that conditioning occurs entirely as
a result of environmental events, such that it would occur equally for any kind of
unconditioned stimulus that followed any kind of conditioned stimulus. Rather, Garcia’s
research showed that genetics matters—organisms are evolutionarily prepared to learn
some associations more easily than others. You can see that the ability to associate
smells with illness is an important survival mechanism, allowing the organism to quickly
learn to avoid foods that are poisonous.
Classical conditioning has also been used to help explain the experience of posttraumatic stress disorder (PTSD), as in the case of P. K.
Philips described at the beginning of this module. PTSD is a severe
anxiety disorder that can develop after exposure to a fearful event, such as the
threat of death. [5] PTSD occurs when the
individual develops a strong association between the situational factors that surrounded
the traumatic event (e.g., military uniforms or the sounds or smells of war) and the US
(the fearful trauma itself). As a result of the conditioning, being exposed to, or even
thinking about the situation in which the trauma occurred (the CS), becomes sufficient
to produce the CR of severe anxiety. [6]
PTSD develops because the emotions experienced during the event have produced neural
activity in the amygdala and created strong conditioned learning. In addition to the
strong conditioning that people with PTSD experience, they also show slower extinction
in classical conditioning tasks. [7] In short, people
with PTSD have developed very strong associations with the events surrounding the trauma
and are also slow to show extinction to the conditioned stimulus.
learn by doing
Instructions: John Garcia’s experiment, described in the
text above, was based on the idea that it is easy to condition some
associations, but others are difficult to condition. He injected a rat with a
chemical that made the rat nauseous.
Let’s reconstruct Garcia’s experiment, so we’re sure that its implications are
clear. Here is our subject, a rat.
 Rat photo by asplosh, CC-BY-2.0
Rat photo by asplosh, CC-BY-2.0
Task #1: Conditioning the rat to a light. Does it work?
Answer each question to fill in the boxes. The emoticon faces represent whether
the rat is happy or sick. You will have one emoticon face left over.
Now show what happened when Garcia tested to see if conditioning had been
successful after only a few of the training trials above. As before, you will
have an emoticon face left over. You will only use one of the stimuli, so pick
the right one to see if classical conditioning has occurred.
Task #2: Conditioning the rat to a distinctive taste (e.g., salt). Does it work?
Answer the questions to fill in the learning phase of the experiment. What are
the conditioned and unconditioned stimuli, and what is the unconditioned
response? You will have one of the emoticon faces left over.
Now show what happened when Garcia tested to see if conditioning had been
successful after only a few of the training trials above. As before, you will
have an emoticon face left over. You will only use one of the stimuli, so pick
the right one to see if classical conditioning has occurred.
Task #3: Conditioning the rat to a tone. Does it work?
Answer the questions to put the pictures in the appropriate locations to show the
learning phase of the experiment. What are the conditioned and unconditioned
stimuli, and what is the unconditioned response? You will have one of the
emoticon faces left over.
Now show what happened when Garcia tested to see if conditioning had been
successful after only a few of the training trials above. As before, you will
have an emoticon face left over. You will only use one of the stimuli, so pick
the right one to see if classical conditioning has occurred.
Images in this activity courtesy of qtipd, inky2010, azieser, rgesthuizen (Public Domain), and L. Marie (CC-BY-2.0).
References
- Öhman, A., and Mineka, S.
(2001).
"Fears, phobias, and preparedness: Toward an evolved module of fear
and fear learning." Psychological Review. Volume 108. Number 3. 483–522
Pages.
- LoBue, V., and DeLoache, J. S.
(2010).
"Superior detection of threat-relevant stimuli in infancy." Developmental Science. Volume 13. Number 1. 221–228 Pages.
- Garcia, J., Kimeldorf, D. J., and Koelling,
R. A.
(1955).
"Conditioned aversion to saccharin resulting from exposure to gamma
radiation." Science. Volume 122. Number 3160. 157–158 Pages.
- Garcia, J., Ervin, F. R., and Koelling, R. A.
(1966).
"Learning with prolonged delay of reinforcement." Psychonomic Science. Volume 5. Number 3. 121–122 Pages.
- American Psychiatric Association
(2000).
Diagnostic and Statistical Manual of Mental Disorders. Author. Washington, DC. Edition 4, text rev.
- Keane, T. M., Zimering, R. T., and Caddell,
J. M.
(1985).
"A behavioral formulation of posttraumatic stress disorder in
Vietnam veterans." Behavior Therapist. Volume 8. Number 1. 9–12 Pages.
- Milad, M. R., Pitman, R. K., Ellis, C. B.,
Gold, A. L., Shin, L. M., Lasko, N. B., et al.
(2009).
"Neurobiological basis of failure to recall extinction memory in
posttraumatic stress disorder." Biological Psychiatry. Volume 66. Number
12. 9–12 Pages.
In this module, you learn about a different kind of conditioning called operant conditioning.
First, remember how classical conditioning works. In classical conditioning, the
individual learns to associate new stimuli with natural, biological responses, such as
salivation or fear. The organism does not learn a new behavior but rather learns to
perform an existing behavior in the presence of a new signal. For example, remember how
Pavlov’s dogs learned to salivate when a bell was rung. This learning occurred because
the dog learned to associate a new stimulus (e.g., the bell) with an existing stimulus
(e.g., the meat), so now the bell produced the same response (the CR: salivation)
originally produced only by the meat.
Operant conditioning, on the other hand, is learning
that occurs on the bases of the consequences of behavior and can involve the
learning of new behaviors. For operant conditioning, the process starts with
doing something—behavior—and then noticing the consequences of that behavior. For
example, operant conditioning occurs when a dog rolls over on command because it has
been praised for doing so in the past. We go into the details of how this learning
happens later in this module, but the important point is that an animal that never
rolled over on command can learn this new behavior because it notices that its actions
lead to rewards—treats or praise.
In summary, classical conditioning is a process in which an individual learns a new cue
for an existing behavior by associating the new cue (the CS) with the existing cue (US).
Operant conditioning is the process of learning a new behavior by noticing the
consequences of that behavior.
Psychologist Edward L. Thorndike (1874–1949) was the first scientist to systematically study
operant conditioning. In his research Thorndike [1] observed cats who had
been placed in a “puzzle box” from which they tried to
escape.
At first the cats scratched, bit, and swatted haphazardly, without any idea how to get
out. But eventually, and accidentally, they pressed the lever that opened the door and
exited to their prize, a scrap of fish. The next time the cat was constrained within the
box, it attempted fewer of the ineffective responses before carrying out the successful
escape, and after several trials the cat learned to almost immediately make the correct
response.
Observing these changes in the cats’ behavior led Thorndike to develop his law of effect, the principle that responses
that create a typically pleasant outcome in a particular situation are more likely
to occur again in a similar situation, whereas responses that produce a typically
unpleasant outcome are less likely to occur again in the
situation. [2] The essence of the law of effect is
that successful responses, because they are pleasurable, are “stamped in” by experience
and thus occur more frequently. Unsuccessful responses, which produce unpleasant
experiences, are “stamped out” and subsequently occur less frequently.
Whem Thorndike placed his cats in a puzzle box, he found that they learned to
engage in the important escape behavior faster after each trial. Thorndike described
the learning that follows reinforcement in terms of the law of effect.
The influential behavioral psychologist B. F. Skinner (1904–1990) expanded on Thorndike’s ideas
to develop a more complete set of principles to explain operant conditioning. Skinner
created specially designed environments known as operant chambers (usually called
Skinner boxes) to systemically study learning. A Skinner box (operant
chamber) is a structure that is big enough to fit a rodent
or bird and that contains a bar or key that the organism can press or peck to
release food or water. It also contains a device to record the animal’s
responses.
The most basic of Skinner’s experiments was quite similar to Thorndike’s research with
cats. A rat placed in the chamber reacted as one might expect, scurrying about the box
and sniffing and clawing at the floor and walls. Eventually the rat chanced upon a
lever, which it pressed to release pellets of food. The next time around, the rat took a
little less time to press the lever, and on successive trials, the time it took to press
the lever became shorter and shorter. Soon the rat was pressing the lever as fast as it
could eat the food that appeared. As predicted by the law of effect, the rat had learned
to repeat the action that brought about the food and cease the actions that did not.
Skinner studied, in detail, how animals changed their behavior through reinforcement and
punishment, and he developed terms that explained the processes of operant learning as
shown in the table below.. Skinner used
the term reinforcer to refer to any event that
strengthens or increases the likelihood of a behavior and the term punisher to refer to any event that weakens or
decreases the likelihood of a behavior. And he used the terms positive and
negative to refer to whether a reinforcement was presented or removed, respectively.
| How Positive and Negative Reinforcement and Punishment Influence Behavior |
|---|
| From Flat World Knowledge, Introduction to Psychology, v1.0, CC-BY-NC-SA. |
| Operant Conditioning term |
Description |
Outcome |
Example |
| Positive reinforcement |
Add or increase a pleasant stimulus |
Behavior is strengthened |
Giving a student a prize after he gets an A on a test |
| Negative reinforcement |
Reduce or remove an unpleasant stimulus |
Behavior is strengthened |
Taking painkillers that eliminate pain increases the likelihood that you will
take painkillers again |
| Positive punishment |
Present or add an unpleasant stimulus |
Behavior is weakened |
Giving a student extra homework after she misbehaves in class |
| Negative Punishment |
Reduce or remove a pleasant stimulus |
Behavior is weakened |
Taking away a teen’s computer after he misses curfew |
|
Reinforcement, either positive or negative, works by increasing the likelihood of a
behavior. Punishment, on the other hand, refers to any event that weakens or reduces the
likelihood of a behavior. Positive punishment weakens a response
by presenting something unpleasant after the response, whereas negative
punishment weakens a response by reducing or removing something pleasant. A
child who is yelled at after fighting with a sibling (positive
punishment) or who loses out on the opportunity to go to recess after getting a poor
grade (negative punishment) is less likely to repeat these behaviors.
learn by doing
For each example below, select which terms best describe
it.
Although the distinction between reinforcement (which increases behavior) and punishment
(which decreases it) is usually clear, in some cases it is difficult to determine
whether a reinforcer is positive or negative. On a hot day a cool breeze could be seen
as a positive reinforcer (because it brings in cool air) or a negative reinforcer
(because it removes hot air). In other cases, reinforcement can be both positive and
negative. One may smoke a cigarette both because it brings pleasure (positive
reinforcement) and because it eliminates the craving for nicotine (negative
reinforcement).
It is important to note that reinforcement and punishment are not simply opposites. The
use of positive reinforcement in changing behavior is almost always more effective than
using punishment. This is because positive reinforcement makes the person or animal feel
better, helping create a positive relationship with the person providing the
reinforcement. Types of positive reinforcement that are effective in everyday life
include verbal praise or approval, the awarding of status or prestige, and direct
financial payment. Punishment, on the other hand, is more likely to create only
temporary changes in behavior because it is based on coercion and typically creates a
negative and adversarial relationship with the person providing the reinforcement. When
the person who provides the punishment leaves the situation, the unwanted behavior is
likely to return.
References
- Thorndike, E. L.
(1898).
Animal Intelligence: An Experimental Study of the Associative Processes in Animals. American Psychological Association. Washington, DC.
- Thorndike, E. L.
(1911).
Animal Intelligence: Experimental Studies. Macmillan. New York. Retrieved from http://www.archive.org/details/animalintelligen00thor .
Perhaps you remember watching a movie or being at a show in which an animal—maybe a dog, a
horse, or a dolphin—did some pretty amazing things. The trainer gave a command and the
dolphin swam to the bottom of the pool, picked up a ring on its nose, jumped out of the
water through a hoop in the air, dived again to the bottom of the pool, picked up another
ring, and then took both of the rings to the trainer at the edge of the pool. The animal
was trained to do the trick, and the principles of operant conditioning were used to train
it. But these complex behaviors are a far cry from the simple stimulus-response
relationships that we have considered thus far. How can reinforcement be used to create
complex behaviors such as these?
One way to expand the use of operant learning is to modify the schedule on which the
reinforcement is applied. To this point we have only discussed a continuous reinforcement schedule, in which the desired
response is reinforced every time it occurs; whenever the dog sits, for instance,
it gets a biscuit. This type of reinforcement schedule can be depicted as follows.
Continuous reinforcement results in relatively fast learning but also rapid extinction of
the desired behavior once the reinforcer disappears. The problem is that because the
organism is used to receiving the reinforcement after every behavior, the responder may
give up quickly when it doesn’t appear.
Most real-world reinforcers are not continuous; they occur on a partial
(or intermittent) reinforcement schedule—a schedule in which the
responses are sometimes reinforced, and sometimes not. In comparison to continuous
reinforcement, partial reinforcement schedules lead to slower initial learning, but they
also lead to greater resistance to extinction. Because the reinforcement does not appear
after every behavior, it takes longer for the learner to determine that the reward is no
longer coming, and thus extinction is slower.
The four types of partial reinforcement schedules are summarized in the following
table.
| Four Types of Partial Reinforcement Schedules |
|---|
| From Flat World Knowledge, Introduction to Psychology, v1.0, CC-BY-NC-SA. |
| Reinforcement Schedule |
Explanation |
Real-world Example |
| Fixed-ratio |
Behavior is reinforced after a specific number of responses |
Factory workers who are paid according to the number of products they produce |
| Variable-ratio |
Behavior is reinforced after an average, but unpredictable, number of responses |
Payoffs from slot machines and other games of chance |
| Fixed-interval |
Behavior is reinforced for the first response after a specific amount of time has
passed |
People who earn a monthly salary |
| Variable-interval |
Behavior is reinforced for the first response after an average, but unpredictable,
amount of time has passed |
Person who checks voice mail for messages |
|
Partial reinforcement schedules are determined by whether the reinforcement is presented on
the basis of the time that elapses between reinforcement (interval) or on the basis of the
number of responses that the organism engages in (ratio), and by whether the reinforcement
occurs on a regular (fixed) or unpredictable (variable) schedule.
In a fixed-interval schedule, reinforcement occurs
for the first response made after a specific amount of time has passed. For
instance, on a one-minute fixed-interval schedule the animal receives a reinforcement every
minute, assuming it engages in the behavior at least once during the minute.
In a variable-interval schedule, the reinforcers
appear on an interval schedule, but the timing is varied around the average interval,
making the actual appearance of the reinforcer unpredictable. An example might be
checking your e-mail: You are reinforced by receiving messages that come, on average, say
every 30 minutes, but the reinforcement occurs only at random times. Interval reinforcement
schedules tend to produce slow and steady rates of responding.
In a fixed-ratio schedule, a behavior is
reinforced after a specific number of responses. For instance, a rat’s behavior may
be reinforced after it has pressed a key 20 times, or a salesperson may receive a bonus
after she has sold 10 products.
A variable-ratio schedule provides reinforcers after a specific but
average number of responses. Winning money from slot machines or on a lottery ticket are
examples of reinforcement that occur on a variable-ratio schedule. For instance, a slot
machine may be programmed to provide a win every 20 times the user pulls the handle, on
average.
Complex behaviors are also created through shaping, the process of guiding an organism’s behavior to the desired outcome
through the use of successive approximation to a final desired behavior. Skinner
made extensive use of this procedure in his boxes as shown in the video
below. For instance, he could train
a rat to press a bar two times to receive food, by first providing food when the animal
moved near the bar. Then when that behavior had been learned he would begin to provide food
only when the rat touched the bar. Further shaping limited the reinforcement to only when
the rat pressed the bar, to when it pressed the bar and touched it a second time, and
finally, to only when it pressed the bar twice. Although it can take a long time, in this
way operant conditioning can create chains of behaviors that are reinforced only when they
are completed.
Reinforcing animals if they correctly discriminate between similar stimuli allows
scientists to test the animals’ ability to learn, and the discriminations that they can
make are sometimes quite remarkable. Pigeons have been trained to distinguish between
images of Charlie Brown and the other Peanuts characters, [1] and
between different styles of music and art. [2] [3]
Behaviors can also be trained through the use of secondary reinforcers. Whereas a primary reinforcer includes stimuli that are naturally preferred or
enjoyed by the organism, such as food, water, and relief from pain, a secondary reinforcer (sometimes called conditioned reinforcer) is a neutral event
that has become associated with a primary reinforcer through classical conditioning. An
example of a secondary reinforcer would be the whistle given by an animal trainer, which
has been associated over time with the primary reinforcer, food. An example of an everyday
secondary reinforcer is money. We enjoy having money, not so much for the stimulus itself,
but rather for the primary reinforcers (the things that money can buy) with which it is
associated.
learn by doing
You want to teach your dog to turn on the light in your living room when you command
him to. Using shaping, put in order the behaviors you would reward. Remember: in
shaping, you are rewarding successive approximations. Start out rewarding the most
general behavior, and as the learning progresses, start rewarding behaviors that look
more and more like the desired behavior.
References
- Cerella, J.
(1980).
"The pigeon’s analysis of pictures." Pattern Recognition. Volume 12. Number 1. 1–16 Pages.
- Porter, D., and Neuringer, A.
(1984).
"Music discriminations by pigeons." Journal of Experimental
Psychology: Animal Behavior Processes. Volume 10. Number 2. 138–148
Pages.
- Watanabe, S., Sakamoto, J., and Wakita, M.
(1995).
"Pigeons’ discrimination of painting by Monet and Picasso." Journal
of the Experimental Analysis of Behavior. Volume 63. Number 2. 165–174
Pages.
Ivan Pavlov, John Watson, and B. F. Skinner were scientists who believed that all learning
could be explained by the processes of conditioning. To critical features of their ideas
about conditioning are useful to keep in mind as you study this section. First, they
thought of learning as being the same thing as behavior change. Don’t confuse this with
the idea that you figure out some idea first and then change your behavior. Second, they
believed that learning (i.e., behavior change) occurs only when the individual directly
and personally experiences the impact of some reward or punishment.
In this section, you will encounter some kinds of learning are difficult to explain using the
ideas that learning occurs only with behavior change and that personal experience is
required for learning. Although classical and operant conditioning play key roles in
learning, they constitute only a part of the total picture.
In the preceding module, where you learned about operant conditioning, you read about Edward
Thorndike’s work with trial-and-error learning. This kind of learning was described in
the video that showed how a cat was able to learn to escape from a puzzle box.
Trial-and-error leads to learning, according to Thorndike, because of the law of effect:
individuals notice the consequences of their actions. They repeat actions that lead to
desirable outcomes and avoid those that lead to undesirable results. Trial-and-error
learning is the basis of operant conditioning.
One type of learning that is not determined by classical conditioning (learned
associations) or operant conditioning (based on trial-and-error) occurs when we suddenly
find the solution to a problem, as if the idea just popped into our head. This type of
learning is known as insight, the sudden understanding of a
solution to a problem. The German psychologist Wolfgang Köhler [1]
carefully observed what happened when he presented chimpanzees with a problem that was
not easy for them to solve, such as placing food in an area that was too high in the
cage to be reached. He found that the chimps first engaged in trial-and-error attempts
at solving the problem, but when these failed they seemed to stop and contemplate for a
while. Then, after this period of contemplation, they would suddenly seem to know how to
solve the problem, for instance by using a stick to knock the food down or by standing
on a chair to reach it. Köhler argued that it was this flash of insight, not the prior
trial-and-error approaches, which were so important for conditioning theories, that
allowed the animals to solve the problem.
References
- Köhler, W.
(1925).
The Mentality of Apes. Harcourt Brace Jovanovich. New York. Trans. E. Winter.
Edward Tolman [1] was studying traditional
trial-and-error learning when he realized that some of his research subjects (rats)
actually knew more than their behavior initially indicated. In one of Tolman’s classic
experiments, he observed the behavior of three groups of hungry rats that were learning to
navigate mazes.
The first group always received a food reward at the end of the maze, so the payoff for
learning the maze was real and immediate. The second group never received any food reward,
so there was no incentive to learn to navigate the maze effectively. The third group was
like the second group for the first 10 days, but on the 11th day, food was now placed at
the end of the maze.
As you might expect when considering the principles of conditioning, the rats in the first
group quickly learned to negotiate the maze, while the rats of the second group seemed to
wander aimlessly through it. The rats in the third group, however, although they wandered
aimlessly for the first 10 days, quickly learned to navigate to the end of the maze as soon
as they received food on day 11. By the next day, the rats in the third group had caught up
in their learning to the rats that had been rewarded from the beginning. It was clear to
Tolman that the rats that had been allowed to experience the maze, even without any
reinforcement, had nevertheless learned something, and Tolman called this latent learning.
Latent learning is to learning that is not
reinforced and not demonstrated until there is motivation to do so. Tolman argued
that the rats had formed a “cognitive map” of the maze but did not demonstrate this
knowledge until they received reinforcement.
In the Learn by Doing exercise below, go through Tolman’s experiment with his three groups
of rats. Keep in mind that Tolman, as a good scientist, was testing an idea that was
controversial at the time: the idea that we can learn something without our behavior
immediately revealing that we have learned it. It is the delay between the learning and the
revealing behavior that is the basis for the name: latent (or “hidden”) learning.
learn by doing
Your task here is to predict what is going to happen on Trial 12 for the “no food
until Trial 11” group.
Option A: Notice that this result is the same as the “no food
on any trial” group. So, if you choose option A, you think that they will not act
differently now than they acted on the first 11 trials and they will continue to make
a lot of wrong turns.
Option B: This option suggests that they are now motivated to
learn the path to the food, but that they will do so in small steps, just as we have
seen for all three groups up to this point. Option B says that they are moving in the
direction of the “food on every trial” group, but that it will take some extra
learning to get there.
Option C: This option says that they already know the path to
the food and, now that they are motivated to get there, they will show that they
already know just as much as the “food on every trial” group. Their performance on
Trial 12 will be the same as the low-error performance of the “food on every trial”
group.
References
- Tolman, E. C., and Honzik, C. H.
(1930).
Introduction and Removal of Reward and Maze Performance in Rats. University of California Press. Berkeley.
Tolman’s studies of latent learning show that animals, and people, can learn during
unrewarded experience, but this learning only shows itself when rewards or punishment
provide motivation to use some knowledge. However, Tolman’s rats at least had the
opportunity to wander through the maze, and the rats in the critical condition did this for
10 days before food provided them with motivation to find an efficient path through the
maze. So we could still hold onto the theory that learning only takes place if you actually
do something, even it it is unrewarded. The direct connection between learning and
behavior—even if the behavior seems aimless—has not been disproved. But in the 1960s,
Albert Bandura conducted a series of experiments showing that learning can and does occur
even when the learner is merely a passive spectator. Learning can occur when someone else is doing all the behaving and receiving all the rewards
and punishments.
One of the best known and most influential experiments in the history of psychology
involved some adults, some children, and a big inflatable doll called a Bobo doll. Bandura
and his colleagues [1]
allowed children to watch an adult—a man or a woman in different conditions of
the study—“playing” with a Bobo doll, an inflatable balloon with a weight in the bottom
that makes it pop back up when you knock it down. Bandura wanted to know if watching the
adults would influence the way the children behaved.
The motivation for Bandura’s study was not that of solving some abstract scientific
question, but a real debate that continues to this day. Many people felt that children who
were “raised properly” would not be influenced very strongly by seeing someone—an
unfamiliar adult, for instance—behave in a mean or hostile way. The children might be upset
by what they saw, but surely they would not imitate poor behavior. As you learned when you
studied about Tolman’s rats, many learning specialists believed that learning (i.e.,
behavior based on experience) only occurs for the individual who is actually doing the
behavior. This theory held by the learning specialists supported the belief that the
children would not learn by watching, because they would not be doing anything and they
would not receive rewards or punishment. Bandura—along with many parents and some other
psychologists—suspected that learning might occur merely by watching the actions of others
and the consequences of those actions.
Watch the following video as Dr. Bandura explains his study to you.
In the following activity, you will go through one of Bandura’s
classic studies.
learn by doing
Phase 1 of the Experiment
Bandura studied the impact of an adult’s behavior on the behavior of children who saw
them. One of his independent variables was whether or not the
adult was hostile or agressive toward the Bobo doll, so for
some children the adults acted aggressively (treatment condition) and for others they
did not (control condition 1) and for yet other children there were no adults at all
(control condition 2). He was also interested to learn if the sex of the child and/or
the sex of the adult model influenced what the child learned.
To give you a good view of how the experiment was organized or “designed,” the first
thing you will do is put all the individuals involved—the adult models and the
children—into the correct places in the study.
Instructions: The boxes show the labels for the three different
modeling conditions: aggressive behavior, non-aggressive behavior (control condition
1), and no model (control condition 2). Organize the study by putting the adult
models and children in the proper boxes. Be sure you distribute the children so that
the same number of boys and girls are in all the conditions with a model. Put the
rest of the children in the No Model boxes.
learn by doing
Phase 1 of the Experiment: The Observation
Phase
The observation phase of the experiment is when the children see the
behavior of the adults. Each child was shown into a room where an adult
was already sitting near the Bobo doll. The child was positioned so he or
she could easily see the adult.
Instructions: There are three people involved in
the first phase of the experiment: an adult model, a child subject or
participant, and an experimenter. Demonstrate your understanding of the
first step of the experiment by moving each of the three characters
(adult, experimenter, and child) to the correct location in the
Experimentation Room depicted below.
Phase 2 of the Experiment: Frustration
Dr. Bandura thought that the children might be a bit more likely to show
aggressive behavior if they were frustrated. The second phase of the
experiment was designed to produce this frustration. After a child had
watched the adult in phase 1, he or she was taken to another room, one
that also contained a lot of attractive, fun toys and was told that is
was fine to play with the toys. As soon as the child started to enjoy
playing with the toys, the experimenter said something.
Phase 3 of the Experiment: The Testing
Phase
After the child was told to stop playing with “the very best toys,” the experimenter
said that he or she could play with any of the toys in the next room. Then the child was taken to a third room. This room
contained a variety of toys. Many of the toys were engaging and interactive, but not
the type that encouraged aggressive play. Critically, the Bobo doll and the hammer
that the model had used in the first phase were now in this new play room. The goal
of this phase in the experiment was to see how the child would react without a model
around.
Instructions: The figure below represents the third room. Three
individuals from the study are indicated by the boxes below the diagram. Drag each of
them to the proper locations to indicate your understanding of the experimental
procedure. One of three individuals does not appear in phase 3 of the study, so put
this individual in the black box that says, “Not in this phase.”
The child was allowed to play freely for 20 minutes. Note that an adult did stay in
the room so the child would not feel abandoned or frightened. However, this adult
worked inconspicuously in a corner and interacted with the child as little as
possible.
During the 20 minutes that the child played alone in the third room, the
experimenters observed his or her behavior from behind a see-through mirror. Using a
complex system that we won’t go into here, the experimenters counted the number of
various types of behaviors that the child showed during this period. These behaviors
included ones directed at the Bobo doll, as well as those involving any of the other
toys. They were particularly interested in the number of behaviors the child showed
that clearly imitated the actions of the adults that the child had observed earlier,
in phase 1.
Below are the results for the number of imitative physically
aggressive acts the children showed on average toward the Bobo doll. These
acts included hitting and punching the Bobo doll. On the left, you see the two
modeling conditions: aggression by the model in phase 1 or no aggression by the model
in phase 1. Note: Children in the no-model conditions showed very few physically
aggressive acts and their results do not change the interpretation, so we will keep
the results simple by leaving them out of the table.
The story is a slightly, though not completely, different when we look at
imitative verbal aggression, rather than physical aggression. The table
below shows the number of verbally aggressive statements by the boys and
girls under different conditions in the experiment. Verbally aggressive
statements were ones like the models had made: for example, “Sock him”
and “Kick him down!”
Note: Just as was true for the physically aggressive
acts, children in the no model conditions showed very few verbally
aggressive acts either and their results do not change the
interpretation, so we will keep the results simple by leaving them out of
the table.
Images in this activity courtesy of Gioppino, klaasvangend, Machovka, Gerald_G, Dug, Machovka (Public Domain); steve greer, Sacheverelle, and Horia Varlan (CC-BY-2.0).
Bandura and his colleagues did other studies in which they had children observe
adults on television performing the acts rather than watching them in person.
The effects of aggressive modeling were weaker when the adult was not
physically present, but the same general pattern of results were found with
television models. In yet another variation, Bandura had the children watch
cartoon models rather than real adults. These results were even weaker than the
television adult model results, but the pattern was still there and the
aggressive modeling effect was still statically significant. Children even
imitated the aggressive behavior of cartoon characters.
Observational learning is useful for animals and for people because it allows
us to learn without having to actually engage in what might be a risky
behavior. Monkeys that see other monkeys respond with fear to the sight of a
snake learn to fear the snake themselves, even if they have been raised in a
laboratory and have never actually seen a
snake. [2] As Bandura put it, “the prospects
for [human] survival would be slim indeed if one could learn only by suffering
the consequences of trial and error. For this reason, one does not teach
children to swim, adolescents to drive automobiles, and novice medical students
to perform surgery by having them discover the appropriate behavior through the
consequences of their successes and failures. The more costly and hazardous the
possible mistakes, the heavier is the reliance on observational learning from
competent learners. [3]
Although modeling is normally adaptive, it can be problematic for children who
grow up in violent families. These children are not only the victims of
aggression, but they also see it happening to their parents and siblings.
Because children learn how to be parents in large part by modeling the actions
of their own parents, it is no surprise that there is a strong correlation
between family violence in childhood and violence as an adult. Children who
witness their parents being violent or who are themselves abused are more
likely as adults to inflict abuse on intimate partners or their children, and
to be victims of intimate violence. [4] In
turn, their children are more likely to interact violently with each other and
to aggress against their
parents. [5]
References
- Bandura, A., Ross, D., and Ross, S. A.
(1963).
"Imitation of film-mediated aggressive models." Journal of Abnormal
and Social Psychology. Volume 66. Number 1. 3–11 Pages.
- Cook, M., and Mineka, S.
(1990).
"Selective associations in the observational conditioning of fear
in rhesus monkeys." Journal of Experimental Psychology: Animal Behavior
Processes. Volume 16. Number 4. 372–389 Pages.
- Bandura, A.
(1977).
"Self-efficacy: Toward a unifying theory of behavior change." Psychological Review. Volume 84. Number 2. 191–215 Pages.
- Heyman, R. E., and Slep, A. M. S.
(2002).
"Do child abuse and interparental violence lead to adulthood family
violence?." Journal of Marriage and Family. Volume 64. Number 4.
864–871 Pages.
- Patterson, G. R., Dishion, T. J., and Bank, L.
(1984).
"Family interaction: A process model of deviancy training." Aggressive Behavior. Volume 10. Number 3. 253–267 Pages.
The average American child watches more than 4 hours of television every day, and two out
of three programs they watch contain aggression. It has been estimated that by the age of
12, the average American child has seen more than 8,000 murders and 100,000 acts of
violence. At the same time, children are also exposed to violence in movies, video games,
and virtual reality games, as well as in music videos that include violent lyrics and
imagery. [1] [2] [3]
It is clear that watching television violence can increase aggression, but what about
violent video games? These games are more popular than ever and also more graphically
violent. Youths spend countless hours playing these games, many of which involve engaging
in extremely violent behaviors. The games often require the player to take the role of a
violent person, to identify with the character, to select victims, and of course to kill
the victims. These behaviors are reinforced by winning points and moving on to higher
levels, and are repeated over and over.
In one experiment, Bushman and Anderson [4]
assessed the effects of viewing violent video games on aggressive thoughts and behavior.
Participants were randomly assigned to play either a violent or a nonviolent video game for
20 minutes. Each participant played one of four violent video
games or
one of four nonviolent video
games.
Participants then read a story, such as this one about Todd, and were asked to list 20
thoughts, feelings, and actions about how they would respond if they were Todd:
Todd was on his way home from work one evening when he had to brake quickly for
a yellow light. The person in the car behind him must have thought Todd was
going to run the light because he crashed into the back of Todd’s car, causing
a lot of damage to both vehicles. Fortunately, there were no injuries. Todd got
out of his car and surveyed the damage. He then walked over to the other
car.
learn by doing
Now it is your task to predict what will happen.
As you read in the text, Bushman and Anderson asked the participants what
they would do, what they would be thinking, and how they would feel if
they were in Todd’s position. The graph above is blank, so your task is
to put the correct results into it. Note that the green bars show the
results for people who had just played a nonviolent video game and the
red bars are for people who just played a violent video game. The Y-axis
shows how aggressive the response is, so a taller bar means MORE
aggressive and a shorter bar means less
aggressive.
It might not surprise you to hear that these exposures to violence have an
effect on aggressive behavior. The evidence is impressive and clear: The more
media violence people, including children, view, the more aggressive they are
likely to be. [5] [6] The
relationship between viewing television violence and aggressive behavior is
about as strong as the relation between smoking and cancer or between studying
and academic grades. People who watch more violence become more aggressive than
those who watch less violence.
As you have just read, playing violent video games also leads to aggressive
responses. A recent meta-analysis by Anderson and Bushman [7]
reviewed 35 research studies that had tested the effects of playing violent
video games on aggression. The studies included both experimental and
correlational studies, with both male and female participants in both
laboratory and field settings. They found that exposure to violent video games
is significantly linked to increases in aggressive thoughts, aggressive
feelings, psychological arousal (including blood pressure and heart rate), as
well as aggressive behavior. Furthermore, playing more video games was found to
relate to less altruistic behavior.
References
- The Henry J. Kaiser Family Foundation.
(2003).
Key facts: TV violence. Retrieved from http://www.kff.org/entmedia/upload/Key-Facts-TV-Violence.pdf.
- Schulenburg, C.
(2007).
Dying to entertain: Violence on prime time broadcast television, 1998 to 2006. Parents Television Council. Retrieved from http://www.parentstv.org/PTC/publications/reports/violencestudy/exsummary.asp.
- Coyne, S. M., and Archer, J.
(2005).
"The relationship between indirect and physical aggression on
television and in real life." Social Development. Volume 14. Number 2.
324–337 Pages.
- Bushman, B. J., and Anderson, C. A.
(2002).
"Violent video games and hostile expectations: A test of the
general aggression model." Personality and Social Psychology Bulletin.
Volume 28. Number 12. 1679–1686 Pages.
- Anderson, C. A., Berkowitz, L., Donnerstein, E.,
Huesmann, L. R., Johnson, J. D., Linz, D., et al.
(2003).
"The influence of media violence on youth." Psychological Science
in the Public Interest. Volume 4. Number 3. 81–110 Pages.
- Cantor, J., Bushman, B. J., Huesmann, L. R., Groebel, J., Malamuth, N. M., Impett, E. A., et al. (Eds.).
(2001).
Some Hazards of Television Viewing: Fears, Aggression, and Sexual Attitudes. Sage. Thousand Oaks, CA.
- Anderson, C. A., and Bushman, B. J.
(2001).
"Effects of violent video games on aggressive behavior, aggressive
cognition, aggressive affect, physiological arousal, and prosocial
behavior: A meta-analytic review of the scientific literature."
Psychological Science. Volume 12. Number 5. 353–359 Pages.
For some people, memory is truly amazing. Consider, for instance, the case of
Kim Peek, who was the inspiration for the Academy Award–winning film Rain
Man.
There are others who are capable of amazing feats of memory. The Russian psychologist A. R.
Luria [1] has described the abilities of a man known as “S,” who seems to
have unlimited memory. S remembers strings of hundreds of random letters for years at a
time, and seems in fact to never forget anything. As you watch the following video, you’ll
notice that at the beginning, Kim is referred to as an idiot savant. Idiot is an old term that was used to describe profound mental retardation. Now we
just say “profound mental retardation.” Kim and people like him are called savants.
The subject of this unit is memory. The term memory
refers to our capacity to acquire, store, and retrieve the
information and habits that guide our behavior. This capacity is
largely modulated by associative learning mechanisms like those discussed in
the unit on learning. Our memories allow us to do relatively simple things,
such as remembering where we parked our car or the name of the current
president of the United States. We can also form complex memories, such as how
to ride a bicycle or write a computer program. Moreover, our memories define us
as individuals—memories are the records of our experiences, our relationships,
our successes, and our failures. Perhaps the coolest aspect of memory is that
it provides us with the means to use mental time travel to access a lifetime of
experiences and learning.
This unit is about human memory, but in our culture we commonly hear the term memory used in conjunction with descriptions of computers. Computer
memory and human memory have some distinct differences and some similarities. Let's take a
look at some of these.
Differences between Brains and Computers
- In computers, information can be accessed only if one knows the exact
location of the memory. In the brain, information can be accessed
through spreading activation from closely related concepts.
- The brain operates primarily in parallel, meaning that it is
multitasking on many different actions at the same time. Although this
is changing as new computers are developed, most computers are
primarily serial—they finish one task before they start another.
- In the brain, there is no difference between hardware (the mechanical
aspects of the computer) and software (the programs that run on the
hardware).
- In the brain, synapses, which operate using an electrochemical
process, are much slower but also vastly more complex and useful than
the transistors used by computers.
- Computers differentiate memory (e.g., the hard drive) from processing
(the central processing unit), but in brains there is no such
distinction. In the brain (but not in computers) existing memory is
used to interpret and store incoming information, and retrieving
information from memory changes the memory itself.
- The brain is self-organizing and self-repairing, but computers are
not. If a person suffers a stroke, neural plasticity will help him or
her recover. If we drop our laptop and it breaks, it cannot fix
itself.
- The brain has significantly more circuitry than any current computer.
The brain is estimated to have 25,000,000,000,000,000 (25 million
billion) interactions among axons, dendrites, neurons, and
neurotransmitters, and that doesn’t include the approximately 1
trillion glial cells that may also be important for information
processing and memory.
Although we depend on computers in multiple aspects of our lives, and computers
eclipse human processing capacity in terms of speed and volume, at least for
some things, human memory is exponentially better than a
computer [2] . Once we learn a face, we can recognize that
face many years later—a task which computers have yet to master. Impressively,
our memories can be acquired rapidly and retained indefinitely. Mitchell [3]
contacted participants 17 years after they had been briefly
exposed to some line drawings in a lab and found that they still could identify
the images significantly better than participants who had never seen them.
In this unit we learn how psychologists use behavioral responses (such as memory tests and
reaction time) to draw inferences about what and how people remember. And we will see that
although we have very good memory for some things, our memories are far from perfect. [4] The errors we make are due to the
fact that our memories are not simply recording devices that input, store, and retrieve the
world around us. Rather, we actively process and interpret information as we remember and
recollect it, and these cognitive processes influence what we remember and how we remember
it. Because memories are constructed, not recorded, when we remember events we don’t
reproduce exact replicas of those events. [5]
We also learn that our prior knowledge can influence our memory. People who read the words
dream, sheets, rest, snore, blanket, tired, and bed and are then asked to
remember the words often think they saw the word sleep even though
that word was not in the list. [6] In other circumstances, we are influenced
by the ease with which we can retrieve information from memory or by the information that
we are exposed to after we first learn something.
Basic memory research has revealed profound inaccuracies in our memories and judgments.
Understanding these potential errors is the first step in learning to account for them in
our everyday lives.
References
- Luria, A.
(2004).
The Mind of a Mnemonist: A Little Book about a Vast Memory. Harvard University Press. Cambridge, MA.
- Bahrick, H. P.
(2000).
The Oxford Handbook of Memory. Chapter
Long-term maintenance of knowledge. Oxford University Press. New York.
347–362 Pages. E. Tulving and F. I. M. Craik (Eds.).
- Mitchell, D. B.
(2006).
"Nonconscious priming after 17 years: Invulnerable implicit
memory?." Psychological Science. Volume 17. Number 11. 925–928 Pages.
- Schacter, D. L.
(1996).
Searching for Memory: The Brain, the Mind, and the Past. Basic Books. New York.
- Bartlett, F. C.
(1932).
Remembering. Cambridge University Press. Cambridge.
- Roediger, H. L., and McDermott, K. B.
(1995).
"Creating false memories: Remembering words not presented in
lists." Journal of Experimental Psychology: Learning, Memory, and
Cognition. Volume 21. Number 4. 803–814 Pages.
| Types of Memory |
|---|
| Type |
Description |
| Explicit |
Semantic, episodic |
| Implicit |
Procedural, priming, classical conditioning |
|
Explicit Memory
Explicit memory refers to knowledge or experiences that can be consciously and intentionally
remembered. For instance, recalling when you have a dentist
appointment or what you wore to senior prom relies on explicit memory. As
you can see in the figure below, there are two types of explicit memory:
episodic and semantic. Episodic memory refers to
the firsthand experiences, or episodes, that we
have on a daily basis (e.g., recollections of our high school
graduation day or of the fantastic show we saw in New York last
summer). Semantic memory refers to our knowledge of facts and concepts about the world
(e.g., that the absolute value of −90 is greater than the absolute
value of 9 and that one definition of the word affect is “the
experience of feeling or emotion”).
Ways to Measure Memory
Memory is assessed using measures that require an individual to
consciously retrieve information. A recall test is
a measure of explicit memory that involves
retrieving information that has been previously learned, and it
requires us to use a search strategy to perform that retrieval. We rely
on our recall memory when we take an essay test, because the test
requires us to generate previously remembered information. A
multiple-choice test is an example of a recognition
memory test, a measure of memory that involves
determining whether information has been seen or learned
before.
learn by doing
Read about and view the following historical event, and then respond to
the questions below in terms of whether the information/memory in
question is semantic or episodic.
On April 29, 2011, England’s Prince William married his longtime
girlfriend, Kate Middleton, in Westminster Abbey. The Dean of Westminster,
the Very Reverend Dr. John Hall, expressed his delight at the couple’s
announcement of their choice of Westminster as the place to hold the
ceremony. In attendance were various political and religious leaders as
well as a number of celebrities such as Elton John and David Beckham,
although most of the guest were friends and family of the couple.
Watch these highlights of the ceremony.
Your own experiences taking tests will probably lead you to agree with the
scientific research finding that recall is more difficult than recognition.
Recall, such as required on essay tests, involves two steps: first generating
an answer and then determining whether it seems to be the correct one.
Recognition, as on multiple-choice tests, only involves determining which item
from a list seems most
correct. [1] Although they
involve different processes, recall and recognition memory measures tend to be
correlated. Students who do better on a multiple-choice exam will also, by and
large, do better on an essay
exam. [2]
A third way of measuring memory is known as relearning. [3]
Measures of relearning (or
savings)
assess how much more quickly information is processed or
learned when it is studied again after it has already been learned but then
forgotten. If you have taken some French courses in the past, for
instance, you might have forgotten most of the vocabulary you learned. But if
you were to work on your French again, you’d learn the vocabulary much faster
the second time around. Relearning can be a more sensitive measure of memory
than either recall or recognition because it allows assessing memory in terms
of “how much” or “how fast” rather than simply “correct” versus “incorrect”
responses. Relearning also allows us to measure memory for procedures like
driving a car or playing a piano piece, as well as memory for facts and
figures.
Implicit Memory
While explicit memory consists of the things that we can consciously report that we
know, implicit memory refers to knowledge that we cannot consciously access. However,
implicit memory is nevertheless exceedingly important to us because it has a direct
effect on our behavior. Implicit memory refers to the influence of experience on behavior, even if the individual is
not aware of those influences. As you can see above in the figure below,
there are three general types of implicit memory: procedural memory, classical
conditioning effects, and priming.
Procedural memory refers to our
often unexplainable knowledge of how to do things. When we walk
from one place to another, speak to another person in English, dial a
cell phone, or play a video game, we are using procedural memory.
Procedural memory allows us to perform complex tasks, even though we may
not be able to explain to others how we do them. It is difficult to tell
someone how to ride a bicycle; a person has to learn by doing it. The
idea of implicit memory helps explain how infants are able to learn. The
ability to crawl, walk, and talk are procedures, and these skills are
easily and efficiently developed while we are children despite the fact
that as adults we have no conscious memory of having learned them.
A second type of implicit memory is classical
conditioning effects, in which we learn, often
without effort or awareness, to associate neutral stimuli (such as a
sound or a light) with another stimulus (such as food), which creates
a naturally occurring response, such as enjoyment or salivation.
The memory for the association is demonstrated when the conditioned
stimulus (the sound) begins to create the same response as the
unconditioned stimulus (the food) did before the learning.
The final type of implicit memory is known as priming, or changes in behavior as a result
of experiences that have happened frequently or recently. Priming
refers both to the activation of knowledge (e.g., we can prime the
concept of “kindness” by presenting people with words related to
kindness) and to the influence of that activation on behavior (people who
are primed with the concept of kindness may act more kindly).
One measure of the influence of priming on implicit memory is the word fragment test, in which a person is asked to
fill in missing letters to make words. You can try this yourself: First,
try to complete the following word fragments, but work on each one for
only three or four seconds. Do any words pop into mind quickly?
_ i b _ a _ y
_ h _ s _ _ i _ n
_ o _ k
_ h _ i s _
Now read the following sentence carefully:
“He got his materials from the shelves, checked them
out, and then left the building.”
Then try again to make words out of the word fragments.
You might find that it is easier to complete fragments 1 and 3 as “library” and
“book,” respectively, after you read the sentence than it was before you read it.
However, reading the sentence didn’t really help you to complete fragments 2 and 4 as
“physician” and “chaise.” This difference in implicit memory probably occurred
because as you read the sentence, the concept of library (and perhaps book) was
primed, even though they were never mentioned explicitly. Once a concept is primed it
influences our behaviors, for instance, on word fragment tests.
Our everyday behaviors are influenced by priming in a wide variety of
situations. Seeing an advertisement for cigarettes may make us start
smoking, seeing the flag of our home country may arouse our patriotism,
and seeing a student from a rival school may arouse our competitive
spirit. And these influences on our behaviors may occur without our being
aware of them.
Research Focus: Priming outside Awareness Influences Behavior
One of the most important characteristics of implicit memories is that they are
frequently formed and used automatically, without much effort
or awareness on our part. In one demonstration of the automaticity and influence of
priming effects, John Bargh and his colleagues [4]
conducted a study in which they showed
college students lists of five scrambled words, each of which they were to make into
a sentence. Furthermore, for half of the research participants, the words were
related to stereotypes of the elderly. These participants saw words such as the
following:
in Florida retired live people
bingo man the forgetful plays
The other half of the research participants also made sentences, but from
words that had nothing to do with elderly stereotypes. The purpose of
this task was to prime stereotypes of elderly people in memory for some
of the participants but not for others.
The experimenters then assessed whether the priming of elderly stereotypes would have
any effect on the students’ behavior—and indeed it did. When the research participant
had gathered all of his or her belongings, thinking that the experiment was over, the
experimenter thanked him or her for participating and gave directions to the closest
elevator. Then, without the participants knowing it, the experimenters recorded the
amount of time that the participant spent walking from the doorway of the
experimental room toward the elevator. As you can see in the figure
below, participants
who had made sentences using words related to elderly stereotypes took on the
behaviors of the elderly—they walked significantly more slowly as they left the
experimental room.
To determine if these priming effects occurred out of the awareness of
the participants, Bargh and his colleagues asked still another group of
students to complete the priming task and then to indicate whether they
thought the words they had used to make the sentences had any
relationship to each other, or could possibly have influenced their
behavior in any way. These students had no awareness of the possibility
that the words might have been related to the elderly or could have
influenced their behavior.
References
- Haist, F., Shimamura, A. P., and Squire, L. R.
(1992).
"On the relationship between recall and recognition memory."
Journal of Experimental Psychology: Learning, Memory, and Cognition.
Volume 18. Number 4. 691–702 Pages.
- Bridgeman, B., and Morgan, R.
(1996).
"Success in college for students with discrepancies between
performance on multiple-choice and essay tests." Journal of Educational
Psychology. Volume 88. Number 2. 333–340 Pages.
- Nelson T. O.
(1985).
"Ebbinghaus’s contribution to the measurement of retention: Savings
during relearning." Journal of Experimental Psychology: Learning,
Memory, and Cognition. Volume 11. Number 3. 472–478 Pages.
- Bargh, J. A., Chen, M., and Burrows, L.
(1996).
"Automaticity of social behavior: Direct effects of trait construct
and stereotype activation on action." Journal of Personality and Social
Psychology. Volume 71. Number 2. 230–244 Pages.
Sensory and Short-Term Memory
Another way of understanding memory is to think about it in terms of stages that
describe the length of time information remains available to us. According to this
approach, as shown the following figure,
information begins in sensory memory, moves to short-term memory, and
eventually moves to long-term memory. But not all information
makes it through all three stages; most of it is forgotten. Whether the information
moves from shorter-duration memory into longer-duration memory or whether it is lost
from memory entirely depends on how the information is attended to and processed.
Sensory Memory
Sensory memory refers to the brief storage
of sensory information. Sensory memory is a memory buffer that lasts only
very briefly and then, unless it is attended to and passed on for more processing, is
forgotten. The purpose of sensory memory is to give the brain some time to process
the incoming sensations and to allow us to see the world as an unbroken stream of
events rather than as individual pieces.
Visual sensory memory is known as iconic
memory. Iconic memory was first studied by the psychologist George
Sperling. [1] In his research,
Sperling showed participants a display of letters in rows, similar to the figure
shown in the following activity.
However, the display lasted only about 50 milliseconds (1/20 of a second). Then,
Sperling gave his participants a recall test in which they were asked to name all the
letters that they could remember. On average, the participants could remember only
about one-quarter of the letters that they had seen.
learn by doing
 From Flat World Knowledge, Introduction to
Psychology, v1.0. Adapted from Sperling, G. (1960). The information
available in brief visual presentation. Psychological
Monographs, 74(11), 1–29.
From Flat World Knowledge, Introduction to
Psychology, v1.0. Adapted from Sperling, G. (1960). The information
available in brief visual presentation. Psychological
Monographs, 74(11), 1–29.
Sperling [1]
showed his participants displays such as this one for only 1/20
of a second. He found that when he cued the participants to report one of the
three rows of letters, they could do it, even if the cue was given shortly
after the display had been removed. The research demonstrated the existence of
iconic memory.
Instructions: You will now be a participant in a similar
experiment on the time course of iconic memory. You will see a brief grid of
letters and, after the letters are hidden, you will see a green diamond
signaling which row of letters to type. Press Start to begin.
Sperling reasoned that the participants had seen all the letters but could remember
them only very briefly, making it impossible for them to report them all. To test
this idea, in his next experiment he first showed the same letters, but then after the display had been removed, he signaled to the
participants to report the letters from either the first, second, or third row. In
this condition, the participants now reported almost all the letters in that row.
This finding confirmed Sperling’s hunch: Participants had access to all of the
letters in their iconic memories, and if the task was short enough, they were able to
report on the part of the display he asked them to. The “short enough” is the length
of iconic memory, which turns out to be about 250 milliseconds (¼ of a second).
Auditory sensory memory is known as echoic
memory. In contrast to iconic memories, which decay very rapidly, echoic
memories can last as long as 4 seconds. [2] This is convenient as it allows
you—among other things—to remember the words that you said at the beginning of a long
sentence when you get to the end of it, and to take notes on your psychology
professor’s most recent statement even after he or she has finished saying it.
learn by doing
Instructions: You will now hear a series of sound clips
containing white noise. It is hard to use words to describe different types of
white noise, which makes it hard to use short-term memory to help find patterns
within white noise. Some of the clips contain repeating patterns and others do
not. After listening to each clip, decide whether it contained a repeating
pattern or not.
In some people iconic memory seems to last longer, a
phenomenon known as eidetic imagery (or “photographic memory”)
in which people can report details of an image over long periods of time. These
people, who often suffer from psychological disorders such as autism, claim that they
can “see” an image long after it has been presented, and can often report accurately
on that image. There is also some evidence for eidetic memories in hearing; some
people report that their echoic memories persist for unusually long periods of time.
The composer Wolfgang Amadeus Mozart may have possessed eidetic memory for music,
because even when he was very young and had not yet had a great deal of musical
training, he could listen to long compositions and then play them back almost
perfectly. [3]
Short-Term Memory
Most of the information that gets into sensory memory is forgotten, but information
that we turn our attention to, with the goal of remembering it, may pass into
short-term memory. Short-term memory (STM) is the place where small amounts of information can be temporarily
kept for more than a few seconds but usually for less than one minute. [4] The
cognitive psychologist George Miller [5]
referred to “seven plus or minus two” pieces of information as the
“magic number” in short-term memory. Information in short-term memory is not stored
permanently but rather becomes available for us to process, and the processes that we use to make sense of, modify, interpret, and store
information in STM are known as working memory.
Although it is called “memory,” working memory is not a store of memory like STM but
rather a set of memory procedures or operations. Imagine, for instance, that you are
asked to participate in a task such as this one, which is a measure of working
memory. [6]
Each of the following questions appears individually on a computer screen and then
disappears after you answer the question:
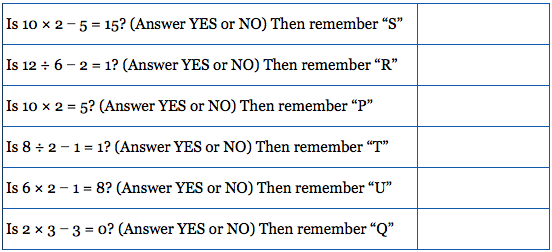 From Flat World Knowledge, Introduction to Psychology,
v1.0. Adapted from Unsworth, N., and Engle, R.W. (2007). On the
division of short-term and working memory: An examination of simple and
complex span and their relation to higher order abilities. Psychological Bulletin, 133(6),
1038-1066.
From Flat World Knowledge, Introduction to Psychology,
v1.0. Adapted from Unsworth, N., and Engle, R.W. (2007). On the
division of short-term and working memory: An examination of simple and
complex span and their relation to higher order abilities. Psychological Bulletin, 133(6),
1038-1066.
To successfully accomplish the task, you have to answer each of the math problems
correctly and at the same time remember the letter that follows the task. Then, after
the six questions, you must list the letters that appeared in each of the trials in
the correct order (in this case S, R, P, T, U, Q).
To accomplish this difficult task, you need to use a variety of skills. You clearly
need to use STM, as you must keep the letters in storage until you are asked to list
them. But you also need a way to make the best use of your available attention and
processing. For instance, you might decide to use a strategy of “repeat the letters
twice, then quickly solve the next problem, and then repeat the letters, including
the new one, twice again.” Keeping this strategy (or others like it) going is the
role of working memory’s central executive—the part of
working memory that directs attention and processing. The central executive will make
use of whatever strategies seem to be best for the given task. For instance, the
central executive will direct the rehearsal process and at the same time direct the
visual cortex to form an image of the list of letters in memory. You can see that
although STM is involved, the processes that we use to operate on the material in
memory are also critical.
STM is limited in both the length and the amount of information it can hold. Peterson
and Peterson [7]
found that when people were asked to remember a list of
three-letter strings and then were immediately asked to perform a distracting task
(counting backward by threes), the material was quickly forgotten, as shown the
figure below, such that by 18 seconds it was
virtually gone.
One way to prevent the decay of information from STM is to use working memory to
rehearse it. Maintenance rehearsal is the
process of repeating information mentally or out loud with the goal of keeping it
in memory. We engage in maintenance rehearsal to keep something that we want
to remember (e.g., a person’s name, e-mail address, or phone number) in mind long
enough to write it down, use it, or potentially transfer it to long-term memory.
If we continue to rehearse information, it will stay in STM until we stop rehearsing
it, but there is also a capacity limit to STM. Try reading each of the following rows
of numbers, one row at a time, at a rate of about one number each second. Then when
you have finished each row, close your eyes and write down as many of the numbers as
you can remember.
019
3586
10295
861059
1029384
75674834
657874104
6550423897
If you are like the average person, you will have found that on this test of working
memory, known as a digit span test, you did pretty well up to
about the fourth line, and then you started having trouble. I bet you missed some of
the numbers in the last three rows, and did pretty poorly on the last one.
The digit span of most adults is between five and nine digits, with an average of
about seven, as noted by Miller [5] .
But if we can only hold a maximum of about nine digits in short-term memory, then how
can we remember larger amounts of information than this? For instance, how can we
ever remember a 10-digit phone number long enough to dial it?
One way we are able to expand our ability to remember things in STM is by using a
memory technique called chunking. Chunking is the process of organizing information into
smaller groupings (chunks), thereby increasing the number of items that can be
held in STM. For instance, try to remember this string of 12 letters:
XOFCBANNCVTM
You probably won’t do that well because the number of letters is more than the magic
number of seven.
Now try again with this one:
MTVCNNABCFOX
Would it help you if I pointed out that the material in this string could be chunked
into four sets of three letters each? I think it would, because then rather than
remembering 12 letters, you would only have to remember the names of four television
stations. In this case, chunking changes the number of items you have to remember
from 12 to only four.
Experts rely on chunking to help them process complex information. Herbert Simon and
William Chase [8]
showed chess masters and chess novices various positions of pieces
on a chessboard for a few seconds each. The experts did a lot better than the novices
in remembering the positions because they were able to see the “big picture.” They
didn’t have to remember the position of each of the pieces individually, but chunked
the pieces into several larger layouts. But when the researchers showed both groups
random chess positions—positions that were unlikely to occur in real games—both
groups did equally poorly, because in this situation the experts lost their ability
to organize the layouts, as shown in the following
figure. The same
occurs for basketball. Basketball players recall actual basketball positions much
better than do nonplayers, but only when the positions make sense in terms of what is
happening on the court, or what is likely to happen in the near future, and thus can
be chunked into bigger units. [9]
If information makes it past STM it may enter long-term memory
(LTM), memory storage that can hold information for days,
months, and years. The capacity of long-term memory is large, and there is no
known limit to what we can remember. [10] Although we may
forget at least some information after we learn it, other things will stay with us
forever. In the next section we will discuss the principles of long-term memory.
References
- Sperling, G.
(1960).
"The information available in brief visual presentation." Psychological Monographs. Volume 74. Number 11. 1–29 Pages.
- Cowan, N., Lichty, W., and Grove, T. R.
(1990).
"Properties of memory for unattended spoken syllables." Journal of Experimental Psychology: Learning, Memory, and
Cognition. Volume 16. Number 2. 258–268 Pages.
- Solomon, M.
(1995).
Mozart: A Life. Harper Perennial. New York.
- Baddeley, A. D., Vallar, G., and Shallice, T.
(1990).
Neuropsychological Impairments of Short-Term Memory.
Chapter The development of the concept of working memory: Implications
and
contributions of neuropsychology. Cambridge University
Press. New York. 54–73 Pages. G. Vallar and T. Shallice (Eds.).
- Miller, G. A.
(1956).
"The magical number seven, plus or minus two: Some limits on our capacity for
processing information." Psychological Review. Volume 63. Number 2. 81–97 Pages.
- Unsworth, N., and Engle, R. W.
(2007).
"On the division of short-term and working memory: An examination
of simple
and complex span and their relation to higher order
abilities." Psychological Bulletin. Volume 133. Number 6. 1038–1066
Pages.
- Peterson, L., and Peterson, M. J.
(1959).
"Short-term retention of individual verbal items." Journal of
Experimental Psychology. Volume 58. Number 3. 193–198 Pages.
- Simon, H. A., and Chase, W. G.
(1973).
"Skill in chess." American Scientist. Volume 61. Number 4. 394–403 Pages.
- Didierjean, A., and Marmèche, E.
(2005).
"Anticipatory representation of visual basketball scenes by novice and expert
players." Visual Cognition. Volume 12. Number 2. 265–283 Pages.
- Wang, Y., Liu, D., and Wang, Y.
(2003).
"Discovering the capacity of human memory." Brain and Mind. Volume 4. Number 2. 189–198 Pages.
Although it is useful to hold information in sensory and short-term memory, we also rely on
our long-term memory (LTM). Long-term memory is relatively permanent storage. Explicit
memories stored there will stay with us throughout our lifetime (barring a brain disease or
injury) as long as we continue to use them. Most of us who teach psychology originally
learned the material many years ago. But because we continue to use the information, it
remains readily available to us. Once we stop using the material we have learned, it will
gradually fade. Implicit memories are less subject to fading with disuse, but over time,
they will fade too. If you learn to ski as a child, stop in your teens, and then resume it
again in your 40s, you will still remember some of what you learned, but you’ll have to
practice again to do it well.
We use long-term memory to remember the name of the new boy in the class, the name of the
movie we saw last week, and the material for our upcoming psychology test. Psychological
research has produced a great deal of knowledge about long-term memory, and this research
can be useful as you try to learn and remember new material. In this module we consider
this question in terms of the types of processing we do on the information we want to
remember. To be successful, the information we want to remember must be encoded and stored
and then retrieved. The rest of this module discusses these three
concepts.
Encoding is the process by which
we place our experiences into memory. Unless information is
encoded, it cannot be remembered. I’m sure you’ve been to a party where
you were introduced to someone, and then—maybe only seconds later—you
realized you did not remember the person’s name. It's not surprising that
you forgot the name, because you probably were distracted and never
encoded the name to begin with.
Not everything we experience can or should be encoded. We tend to encode
things that we need to remember and not bother to encode things that are
irrelevant. Look at figure below,
which shows
different images of U.S. pennies. Can you tell which one is the real one?
Nickerson and Adams [1] found that very few of the U.S.
participants they tested could identify the right one. We see pennies a
lot, but we don’t bother to encode their features.
One way to improve our memory is to use better encoding strategies. Some ways of studying
are more effective than others. Research has found that we are better able to remember
information if we encode it in a meaningful way. When we engage in elaborative encoding, we process new information in ways that
make it more relevant or
meaningful. [2] [3]
Imagine that you are trying to remember the characteristics of the different schools of
psychology we discussed in the first unit.
Rather
than simply trying to remember the schools and their characteristics, you might try to
relate the information to things you already know. For instance, you might try to remember
the fundamentals of the cognitive school of psychology by linking the characteristics to
the computer model. The cognitive school focuses on how information is input, processed,
and retrieved, and you might think about how computers do pretty much the same thing. You
might also try to organize the information into meaningful units. For instance, you might
link the cognitive school to structuralism because both are concerned with mental
processes. You also might try to use visual cues to help you remember the information. You
might look at the image of Freud and imagine what he looked like as a child. That image
might help you remember that childhood experiences were an important part of Freudian
theory. Each person has his or her unique way of elaborating on information; the important
thing is to try to develop unique and meaningful associations among the materials. These
suggestions are very good study hints.
learn by doing
We all have knowledge bases we can build upon. Some information connects in
meaningful ways to previous knowledge more easily than does other information—for
example, a Spanish speaker can connect knowledge of Spanish grammar to help remember
the rules of French grammar. Elaborative encoding makes use of these connections.
Research Focus: Elaboration and Memory
In an important study showing the effectiveness of elaborative encoding,
Rogers, Kuiper, and Kirker [4] studied how people recalled
information that they had learned under different processing conditions.
All the participants were presented with the same list of 40 adjectives
to learn, but through the use of random assignment, the participants were
given one of four different sets of instructions about how to process the
adjectives.
Participants assigned to the structural task condition
were asked to judge whether the word was printed in uppercase or
lowercase letters. Participants in the phonemic task
condition were asked whether or not the word rhymed with another
given word. In the semantic task condition, the
participants were asked if the word was a synonym of another word. And in
the self-reference task condition, participants
were asked to indicate whether or not the given adjective was or was not
true of themselves. After completing the specified task, each participant
was asked to recall as many adjectives as he or she could remember.
Rogers and his colleagues hypothesized that different types of processing would have
different effects on memory. As you can see in the following figure,
participants in the self-reference
task condition recalled significantly more adjectives than did participants in any
other condition. This finding, known as the self-reference
effect, is powerful evidence that the self-concept helps us organize and
remember information. The next time you are studying for an exam, you might try
relating the material to your own experiences. The self-reference effect suggests
that doing so will help you better remember the
information. [5]
References
- Nickerson, R. S., and Adams, M. J.
(1979).
"Long-term memory for a common object." Cognitive Psychology. Volume 11. Number 3. 287–307 Pages.
- Craik, F. I., and Lockhart, R. S.
(1972).
"Levels of processing: A framework for memory research." Journal of
Verbal Learning and Verbal Behavior. Volume 11. Number 6. 671–684
Pages.
- Harris, J. L., and Qualls, C. D.
(2000).
"The association of elaborative or maintenance rehearsal with age,
reading comprehension and verbal working memory performance."
Aphasiology. Volume 14. Number 5–6. 515–526 Pages.
- Rogers, T. B., Kuiper, N. A., and Kirker, W.
S.
(1977).
"Self-reference and the encoding of personal information." Journal
of Personality and Social Psychology. Volume 35. Number 9. 677–688
Pages.
- Symons, C. S., and Johnson, B. T.
(1997).
"The self-reference effect in memory: A meta-analysis." Psychological Bulletin. Volume 121. Number 3. 371–394 Pages.
Hermann Ebbinghaus (1850–1909) was a pioneer of the study of memory. In this section we
consider three of his most important findings, each of which can help you improve your
memory. In his research, in which he was the only research participant, Ebbinghaus
practiced memorizing lists of nonsense syllables, such as the following:
DIF, LAJ, LEQ, MUV, WYC, DAL, SEN, KEP, NUD
You can imagine that because the material he was trying to learn was not at
all meaningful, it was not easy to do. Ebbinghaus plotted how many of the
syllables he could remember against the time that had elapsed since he studied
them. He discovered an important principle of memory: Memory decays rapidly at
first, but the amount of decay levels off with time (see the Ebbinghaus
Forgetting Curve in the following figure). Although Ebbinghaus looked at
forgetting after days had elapsed, the same effect occurs on longer and shorter
time scales. Bahrick [1] found that students who took a Spanish
language course forgot about one half of the vocabulary they had learned within
3 years, but after that time, their memory remained pretty much constant.
Forgetting also drops off quickly on a shorter time frame, which suggests that
you should try to review the material you have already studied right before you
take an exam; that way, you will be more likely to remember the material during
the exam.
Ebbinghaus also discovered another important principle of learning, known as
the spacing effect. The spacing effect refers to the fact that learning is better when the same amount of
study is spread out over periods of time than it is when it occurs closer
together or at the same time. This means that even if you have only a
limited amount of time to study, you’ll learn more if you study continually
throughout the semester (a little bit every day is best) than if you wait to
cram at the last minute before your exam. Another good strategy is to study and
then wait as long as you can before you forget the material. Then review the
information and again wait as long as you can before you forget it. (This
probably will be a longer period of time than the first time.) Repeat and
repeat again. The spacing effect is usually considered in terms of the
difference between distributed practice (practice that
is spread out over time) and massed practice (practice
that comes in one block), with the former approach producing better memory.
Ebbinghaus also considered the role of overlearning—that is, continuing to practice and study even when we think that we have mastered
the material. Ebbinghaus and other researchers have found that overlearning helps
encoding. [2] Students frequently think
that they have already mastered the material but then discover when they get to the exam
that they have not. The point is clear: Try to keep studying and reviewing, even if you
think you already know all the material.
learn by doing
Instructions: Answer the first two questions on the
basis of what you know so far about the forgetting curve. Answer the
third and fourth questions on the basis of what you know about the
spacing effect and overlearning.
References
- Bahrick, H. P.
(1984).
"Semantic memory content in permastore: Fifty years of memory for
Spanish learned in school." Journal of Experimental Psychology: General.
Volume 113. Number 1. 1–29 Pages.
- Driskell, J. E., Willis, R. P., and Copper, C.
(1992).
"Effect of overlearning on retention." Journal of Applied Psychology. Volume 77. Number 5. 615–622 Pages.
Even when information has been adequately encoded and stored, it does not do us any good if
we cannot retrieve it. Retrieval is the process of
reactivating information that has been stored in memory.
We’ve all experienced retrieval failure in the form of the frustrating tip-of-the-tongue phenomenon in which we are certain that we
know something that we are trying to recall but cannot quite come up with it. You
can try this one on your friends as well. Read your friend the names of the 10 states
listed below, and ask him or her to name the capital city of each state. Now, for the
capital cities that your friend can’t name, provide just the first letter of the capital
city. You’ll probably find that having the first letters of the cities helps with
retrieval. The tip-of-the-tongue experience is a very good example of the inability to
retrieve information that is actually stored in memory.
Try this demonstration of the tip-of-the-tongue phenomenon with a classmate.
Follow the instructions from the paragraph above.
| States and Capital Cities |
|---|
| From Flat World Knowledge, Introduction to Psychology, v1.0, CC-BY-NC-SA. |
| State |
Capital |
| Georgia |
(Atlanta) |
| Maryland |
(Annapolis) |
| California |
(Sacramento) |
| Louisiana |
(Baton Rouge) |
| Florida |
(Tallahassee) |
| Colorado |
(Denver) |
| New Jersey |
(Trenton) |
| Arizona |
(Phoenix) |
| Nebraska |
(Lincoln) |
| Kentucky |
(Frankfort) |
|
learn by doing
You can get an idea of the difficulty posed by retrieval by simply
reading each of the words in the activity below. After you have read all
the words, you will be asked to recall them.
Instructions: On the next page you will have 2 minutes to memorize a list of words. After you read the list, you will be
given time to enter all the words that you can recall. Press Start to begin.
We are more likely to be able to retrieve items from memory when conditions at retrieval
are similar to the conditions under which we encoded them. Context-dependent learning refers to an increase in retrieval
when the external situation in which information is learned matches the situation in
which it is remembered. Godden and Baddeley [1]
conducted a study to test this idea using scuba divers. They asked the
divers to learn a list of words either when they were on land or when they were underwater.
Then they tested the divers on their memory, either in the same or the opposite situation.
As you can see in the following figure, the divers’ memory was better when they were tested
in the same context in which they had learned the words than when they were tested in the
other context.
You can see that context-dependent learning might also be important in
improving your memory. For instance, you might want to try to study for an exam
in a situation that is similar to the one in which you are going to take the
exam.
Whereas context-dependent learning refers to a match in the external situation between
learning and remembering, state-dependent learning refers to superior retrieval of memories when the individual is in the same
physiological or psychological state as during encoding. Research has found, for
instance, that animals that learn a maze while under the influence of one drug tend to
remember their learning better when they are tested under the influence of the same drug
than when they are tested without the drug. [2] And research with humans
finds that bilinguals remember better when tested in the same language in which they
learned the material. [3] Mood states may also produce
state-dependent learning. People who learn information when they are in a bad (rather than
a good) mood find it easier to recall these memories when they are tested while they are in
a bad mood, and vice versa. It is easier to recall unpleasant memories than pleasant ones
when we’re sad, and easier to recall pleasant memories than unpleasant ones when we’re
happy. [4] [5]
Variations in the ability to retrieve information are also seen in the serial position curve. When we give people a list of words one at a time (e.g., on
flashcards) and then ask them to recall them, the results look something like those in the
figure below. People are able to retrieve more words that were presented
to them at the beginning and the end of the list than they are words that were presented in
the middle of the list. This pattern, known as the serial position curve, is caused by two
retrieval phenomenon: The primacy effect is a
tendency to better remember stimuli that are presented early in a list. The recency effect is the tendency to better remember
stimuli that are presented later in a list.
There are a number of explanations for primacy and recency effects; one has to
do with the effects of rehearsal on short-term and long-term
memory. [6] Because we can
keep the last words we learned in the presented list in short-term memory by
rehearsing them before the memory test begins, they are relatively easily
remembered. The recency effect therefore can be explained in terms of
maintenance rehearsal in short-term memory. And the primacy effect may also be
due to rehearsal—when we hear the first word in the list, we start to rehearse
it, making it more likely that it will be moved from short-term to long-term
memory. The same is true for the other words that come early in the list. But
for the words in the middle of the list, this rehearsal becomes much harder,
making them less likely to be moved to long-term memory.
In some cases our existing memories influence our new learning. This may occur either in a
backward way or a forward way. Retroactive interference occurs when
learning something new impairs our ability to retrieve information
that was learned earlier. For example, if you have learned to program in one
computer language, and then you learn to program in another similar one, you may start to
make mistakes programming the first language that you never would have made before you
learned the new one. In this case the new memories work backward (retroactively) to
influence retrieval from memory that is already in place.
In contrast to retroactive interference, proactive interference
works in a forward direction. Proactive interference occurs when
earlier learning impairs our ability to encode information that we
try to learn later. For example, if you learned French as a second language, this
knowledge may make it more difficult, at least in some respects, to learn a third language
(say Spanish), which involves similar but not identical vocabulary.
References
- Godden, D. R., and Baddeley, A. D.
(1975).
"Context-dependent memory in two natural environments: On land and
underwater." British Journal of Psychology. Volume 66. Number 3. 325–331
Pages.
- Jackson, A., Koek, W., and Colpaert, F.
(1992).
"NMDA antagonists make learning and recall state-dependent." Behavioural Pharmacology. Volume 3. Number 4. 415 Pages.
- Marian, V., and Kaushanskaya, M.
(2007).
"Language context guides memory content." Psychonomic Bulletin and Review. Volume 14. Number 5. 925–933 Pages.
- Bower, G. H.
(1981).
"Mood and memory." American Psychologist. Volume 36. Number 2. 129–148 Pages.
- Eich, E.
(2008).
Memory and Mind: A Festschrift for Gordon H. Bower.
Chapter Mood and memory at 26: Revisiting the idea of mood mediation in
drug-dependent and place-dependent memory. Lawrence Erlbaum. Mahwah,
NJ. 247–260 Pages. M. A. Gluck, J. R. Anderson, and S. M. Kosslyn
(Eds.).
- Baddeley, A., Eysenck, M. W., and Anderson, M. C.
(2009).
Memory. Psychology Press. New York.
Memories stored in long-term memory are not isolated but rather are linked into
categories—networks of associated
memories that have features in common with each other. Forming
categories and using them to guide behavior is a fundamental part of human
nature. Associated concepts within a category are connected through spreading activation, which occurs when activating one
element of a category activates other associated elements. For instance,
because tools are associated in a category, reminding people of the word
screwdriver will help them remember the word wrench. And when people learn
lists of words that come from different categories (e.g., as in retrieval
exercise on the previous page), they do not recall the information haphazardly.
If they remember the word wrench, they are more likely to remember the word
screwdriver next than they are to remember the word dahlia because the
words are organized in memory by category and because screwdriver is
activated by spreading activation from
wrench. [1]
Some categories have defining features that must be
true of all members of the category. For instance, all members of the category
“triangles” have three sides, and all members of the category “birds” lay eggs.
But most categories are not so well defined; the members of the category share
some common features, but it is impossible to define which are or are not
members of the category. For instance, there is no clear definition of the
category “tool.” Some examples of the category, such as a hammer and a wrench,
are clearly and easily identified as category members, whereas other members
are not so obvious. Is an ironing board a tool? What about a car?
Members of categories (even those with defining features) can be compared to
the category prototype, which is the
member of the category that is most average or typical of the category.
Some category members are more prototypical of, or similar to, the category
than others. For instance, some category members (robins and sparrows) are
highly prototypical of the category “birds,” whereas other category members
(penguins and ostriches) are less prototypical. We retrieve information that is
prototypical of a category faster than we retrieve information that is less
prototypical. [2]
Mental categories are sometimes referred to as schemas—patterns of knowledge in long-term memory
that help us organize information. We have schemas about objects (that
a triangle has three sides and may take on different angles), about people
(that Sam is friendly, likes to golf, and always wears sandals), about events
(the particular steps involved in ordering a meal at a restaurant), and about
social groups (we call these group schemas stereotypes).
Schemas are important in part because they help us remember new information by
providing an organizational structure for it. Read the following
paragraph [3] and then try
to write down everything you can remember.
The procedure is actually quite simple. First you arrange things into
different groups. Of course, one pile may be sufficient depending on how
much there is to do. If you have to go somewhere else due to lack of
facilities, that is the next step; otherwise you are pretty well set. It is
important not to overdo things. That is, it is better to do too few things
at once than too many. In the short run this may not seem important, but
complications can easily arise. A mistake can be expensive as well. At first
the whole procedure will seem complicated. Soon, however, it will become
just another facet of life. It is difficult to foresee any end to the
necessity for this task in the immediate future, but then one never can
tell. After the procedure is completed, one arranges the materials into
different groups again. Then they can be put into their appropriate places.
Eventually they will be used once more and the whole cycle will then have to
be repeated. However, that is part of life.
It turns out that people’s memory for this information is quite poor unless they are told
before they read it that the information describes doing laundry, in which case their
memory for the material is much better. This demonstration of the role of schemas in memory
shows how our existing knowledge can help us organize new information and how this
organization can improve encoding, storage, and retrieval.
| From Flat World Knowledge, Introduction to Psychology, v1.0, CC-BY-NC-SA. |
| Technique |
Description |
Useful Example |
| Use elaborative encoding. |
Material is better remembered if it is processed more fully. |
“Proactive interference is like retroactive interference but it occurs
in a forward manner.” |
| Make use of the self-reference effect. |
Material is better remembered if it is linked to thoughts about the
self. |
“I remember a time when I knew the answer to an exam question but
couldn’t quite get it to come to mind. This was an example of the
tip-of-the-tongue phenomenon.” |
| Be aware of the forgetting curve. |
Our recall of information we have learned drops off rapidly with
time. |
Right before the exam, review the material you have already studied to
increase the likelihood it will remain in memory. |
| Make use of the spacing effect. |
Information is learned better when it is studied in shorter periods
spaced over time. |
Study a little bit every day; do not cram at the last minute. |
| Rely on overlearning. |
We can continue to learn even after we think we know the information
perfectly. |
Keep studying even if you think you already have it down. |
| Use context-dependent retrieval. |
We have better retrieval when it occurs in the same situation in which
we learned the material. |
If possible, study under conditions similar to the conditions under
which you will take the exam. |
| Use state-dependent retrieval. |
We have better retrieval when we are in the same psychological state as
we were when we learned the material. |
Many possibilities, but don’t study under the influence of drugs or
alcohol unless you plan to use them on the day of the exam (which is not
recommended). |
|
References
- Srull, T., and Wyer, R.
(1989).
"Person memory and judgment." Psychological Review. Volume 96. Number 1. 58–83 Pages.
- Rosch, E.
(1975).
"Cognitive representations of semantic categories." Journal of
Experimental Psychology: General. Volume 104. Number 3. 192–233 Pages.
- Bransford, J. D., and Johnson, M. K.
(1972).
"Contextual prerequisites for understanding: Some investigations of
comprehension and recall." Journal of Verbal Learning and Verbal
Behavior. Volume 11. Number 6. 717–726 Pages.
Just as information is stored on digital media such as DVDs and flash drives, the
information in LTM must be stored in the brain. How do different encoding and retrieval
strategies affect our brains at the neural level? We saw from previous sections on
elaborative encoding, categories and schemas that we give LTM a unique internal
organization. Does that mean that there must be a “memory center” of the brain where all
memories are organized for quick retrieval? Additionally, how do diseases such as
Alzheimer’s disease and conditions such as amnesia cause us to forget information we have
already stored in the brain? To answer these questions, we must think of the brain at two
different levels: at the level of neurons and at the level of brain areas.
The ability to maintain information in LTM involves a gradual strengthening of
the connections among the neurons in the brain. When pathways in these neural
networks are frequently and repeatedly fired, the synapses become more
efficient in communicating with each other, and these changes create memory.
This process, known as long-term potentiation (LTP),
refers to the strengthening of the synaptic connections
between neurons as result of frequent
stimulation. [1] Drugs that block LTP reduce
learning, whereas drugs that enhance LTP increase
learning. [2] Because the new patterns of
activation in the synapses take time to develop, LTP happens gradually. The period of time in which LTP occurs and in which memories
are stored is known as the period of
consolidation. Consolidation of memories formed during the day often
happens during sleep, and some theorize that this is one important function of
sleep.
Long-term potentiation occurs as a result of changes in the synapses, which
suggests that chemicals, particularly neurotransmitters and hormones, must be
involved in memory. There is quite a bit of evidence that this is true.
Glutamate, a neurotransmitter and a form of the amino acid glutamic acid, is
perhaps the most important neurotransmitter in
memory. [3] When animals, including people,
are under stress, more glutamate is secreted, and this glutamate can help them
remember. [4] The neurotransmitter serotonin is also
secreted when animals learn, and epinephrine may also increase memory,
particularly for stressful events. [5] [6]
Estrogen, a female sex
hormone, also seems critical, because women who are experiencing menopause,
along with a reduction in estrogen, frequently report memory difficulties. [7]
These changes occur through practice. Rehearsal is
important in learning. Each time we rehearse, the pathway is activated and each
activation strengthens the connections along that pathway.
Our knowledge of the role of biology in memory suggests that it might be
possible to use drugs to improve our memories, and Americans spend several
hundred million dollars per year on memory supplements with the hope of doing
just that. Yet controlled studies comparing memory enhancers, including
Ritalin, methylphenidate, ginkgo biloba, and amphetamines, with placebo drugs
find very little evidence for their effectiveness. [8] [9]
Memory supplements are usually no more effective than drinking a sugared soft
drink, which also releases glucose and thus improves memory slightly.
The following video demonstrates a metaphor for how long-term potentiation
creates strong, easily accessible memories. Please answer the following
questions about long-term potentiation based on the video and the reading.
Memory occurs through sophisticated interactions between new and old brain structures shown
the following figure.
One of the most important brain regions in explicit memory is the hippocampus, which serves as a preprocessor and elaborator of
information. [10] The hippocampus helps us encode
information about spatial relationships, the context in which events were experienced, and
the associations among memories. [11] The hippocampus also
serves in part as a switching point that holds the memory for a short time and then directs
the information to other parts of the brain, such as the cortex, to actually do the
rehearsing, elaboration, and long-term storage. [12]
Without the hippocampus, which might be
described as the brain’s “librarian,” our explicit memories would be inefficient and
disorganized. Even so, the older we get, the more susceptible we are to proactive and
retroactive interference, which shows that the “librarian” finds it harder to retrieve the
right memory from a pile of similar memories as we age. In people with Alzheimer’s disease,
a neurodegenerative disease which is most common in the elderly, the hippocampus is
severely atrophied. Unsurprisingly, one of the most common symptoms of this disease is the
inability to form new memories, followed by a loss of the most recent memories and,
finally, the loss of old memories.
While the hippocampus is handling explicit memory, the cerebellum and
the amygdala are concentrating on implicit and
emotional memories, respectively. Research shows that the cerebellum is more active
when we are learning associations and in priming tasks, and animals and humans with damage
to the cerebellum have more difficulty in classical conditioning
studies. [13] [14]
The cerebellum is also highly involved in the learning of procedural tasks which need fine
motor control, such as writing, riding a bike, and sewing. The storage of many of our most
important emotional memories, and particularly those related to fear, is initiated and
controlled by the amygdala. [15]
If both amygdalae are damaged, people do not lose their memories of positive or negative
emotional associations, but they lose the ability to create new positive or negative
associations with objects and events.
Although some brain structures are particularly important in memory, this does
not mean that all memories are stored in one place. The American psychologist
Karl Lashley [16] attempted to determine where memories were
stored in the brain by teaching rats how to run mazes, and then lesioning
different brain structures to see if they were still able to complete the maze.
This idea seemed straightforward, and Lashley expected to find that memory was
stored in certain parts of the brain. But he discovered that no matter where he
removed brain tissue, the rats retained at least some memory of the maze,
leading him to conclude that memory isn’t located in a single place in the
brain, but rather is distributed around it.
References
- Lynch, G.
(2002).
"Memory enhancement: The search for mechanism-based drugs." Nature
Neuroscience. Volume 5. Number Suppl.. 1035–1038 Pages.
- Lynch, G., Larson, J., Staubli, U., Ambros-Ingerson, J., Granger, R., Lister, R. G., et al.
(1991).
Perspectives on Cognitive Neuroscience.
Chapter Long-term potentiation and memory operations in cortical
networks. Oxford University Press. New York. 110–131 Pages. C. A.
Wickliffe, M. Corballis, and G. White (Eds.).
- McEntee, W., and Crook, T.
(1993).
"Glutamate: Its role in learning, memory, and the aging brain." Psychopharmacology. Volume 111. Number 4. 391–401 Pages.
- McGaugh, J. L.
(2003).
Memory and Emotion: The Making of Lasting Memories. Columbia University Press. New York.
- Maki, P. M., and Resnick, S. M.
(2000).
"Longitudinal effects of estrogen replacement therapy on PET
cerebral blood flow and cognition." Neurobiology of Aging. Volume 21.
Number 2. 373–383 Pages.
- Sherwin, B. B.
(1998).
"Estrogen and cognitive functioning in women." Proceedings of the
Society for Experimental Biological Medicine. Volume 217. 17–22 Pages.
- Chester, B.
(2001).
"Restoring remembering: Hormones and memory." McGill Reporter.
Volume 33. Number 10. Retrieved from
http://www.mcgill.ca/reporter/33/10/sherwin.
- Gold, P. E., Cahill, L., and Wenk, G. L.
(2002).
"Ginkgo biloba: A cognitive enhancer." Psychological Science in the Public Interest. Volume 3. Number 1. 2–11 Pages.
- McDaniel, M. A., Maier, S. F., and
Einstein, G. O.
(2002).
"“Brain-specific” nutrients: A memory cure?." Psychological Science
in the Public Interest. Volume 3. Number 1. 12–38 Pages.
- Squire, L. R.
(1992).
"Memory and the hippocampus: A synthesis from findings with rats,
monkeys, and humans." Psychological Review. Volume 99. Number 2. 195–231
Pages.
- Eichenbaum, H.
(1999).
"Conscious awareness, memory, and the hippocampus." Nature Neuroscience. Volume 2. Number 9. 775–776 Pages.
- Jonides, J., Lacey, S. C., and Nee, D. E.
(2005).
"Processes of working memory in mind and brain." Current Directions
in Psychological Science. Volume 14. Number 1. 2–5 Pages.
- Krupa, D. J., Thompson, J. K., and Thompson, R. F.
(1993).
"Localization of a memory trace in the mammalian brain." Science. Volume 260. Number 5110. 989–991 Pages.
- Woodruff-Pak, D. S., Goldenberg, G.,
Downey-Lamb, M. M., Boyko, O. B., and Lemieux, S. K.
(2000).
"Cerebellar volume in humans related to magnitude of classical
conditioning." Neuroreport: For Rapid Communication of Neuroscience
Research. Volume 11. Number 3. 609–615 Pages.
- Sigurdsson, T., Doyère, V., Cain, C. K.,
and LeDoux, J. E.
(2007).
"Long-term potentiation in the amygdala: A cellular mechanism of
fear learning and memory." Neuropharmacology. Volume 52. Number 1.
215–227 Pages.
- Lashley, K. S.
(1929).
Brain Mechanisms and Intelligence: A Quantitative Study of Injuries to the Brain.
Chapter The effects of cerebral lesions subsequent to the formation of
the maze habit: Localization of the habit. University of Chicago Press.
Chicago. 86–108 Pages.
Our memories are not perfect. They fail in part due to our inadequate encoding
and storage, and in part due to our inability to accurately retrieve stored
information. But memory is also influenced by the setting in which it occurs,
by the events that occur to us after we have experienced an event, and by the
cognitive processes that we use to help us remember. Although our cognition
allows us to attend to, rehearse, and organize information, cognition may also
lead to distortions and errors in our judgments and our behaviors.
In this section we consider some of the cognitive biases that are known to
influence humans. Cognitive biases are errors in memory or judgment that are caused by the inappropriate use of
cognitive
processes.
The study of cognitive biases is important both because it relates to the
important psychological theme of accuracy versus inaccuracy in perception, and
because being aware of the types of errors that we may make can help us avoid
them and therefore improve our decision-making skills.
Misinformation Effects
A particular problem for eyewitnesses such as Jennifer Thompson, who
misidentified her rapist in court resulting in his wrongful conviction,
is that our memories are often influenced by the things that occur to us
after we have learned the
information. [1] [2] [3]
This new information can distort our original memories such that we
are no longer sure what is the real information and what was provided
later. The misinformation effect refers to errors in memory that occur when new information
influences existing memories.
In an experiment by Loftus and Palmer, [4]
participants viewed a film of a traffic accident and then, according to
random assignment to experimental conditions, answered one of three
questions:
- About how fast were the cars going when they hit each other?
- About how fast were the cars going when they smashed each other?
- About how fast were the cars going when they contacted each other?
As you can see in the figure
below, although all the
participants saw the same accident, their estimates of the cars’ speed
varied by condition. Participants who had been asked about the cars
“smashing” each other estimated the highest average speed, and those who
had been asked the “contacted” question estimated the lowest average
speed.
In addition to distorting our memories for events that have actually
occurred, misinformation may lead us to falsely remember information that
never occurred. Loftus and her colleagues asked parents to provide them
with descriptions of events that did (e.g., moving to a new house) and
did not (e.g., being lost in a shopping mall) happen to their children.
Then (without telling the children which events were real or made-up) the
researchers asked the children to imagine both types of events. The
children were instructed to “think real hard” about whether the events
had
occurred. [5]
More than half of the children generated stories regarding at least one
of the made-up events, and they remained insistent that the events did in
fact occur even when told by the researcher that they could not possibly
have occurred. [6] Even
college students are susceptible to manipulations that make events that
did not actually occur seem as if they
did. [7]
The ease with which memories can be created or implanted is particularly problematic
when the events to be recalled have important consequences. Therapists often argue
that patients may repress memories of traumatic events they experienced as children,
such as childhood sexual abuse, and then recover the events years later as the
therapist leads them to recall the information—for instance, by using dream
interpretation and
hypnosis. [8]
But other researchers argue that painful memories such as sexual abuse
are usually very well remembered, that few memories are actually
repressed, and that even if they are, it is virtually impossible for
patients to accurately retrieve them years
later. [9] [10]
These researchers have argued that the procedures used by the therapists
to “retrieve” the memories are more likely to actually implant false
memories, leading the patients to erroneously recall events that did not
actually occur. Because hundreds of people have been accused, and even
imprisoned, on the basis of claims about “recovered memory” of child
sexual abuse, the accuracy of these memories has important societal
implications. Many psychologists now believe that most of these claims of
recovered memories are due to implanted, rather than real,
memories. [11]
Source Monitoring
One potential error in memory involves mistakes in differentiating the
sources of information. Source monitoring refers to the ability to accurately identify the source of a memory.
Perhaps you’ve had the experience of wondering whether you really
experienced an event or only dreamed or imagined it. If so, you wouldn’t
be alone. Rassin, Merkelbach, and Spaan [12]
reported that up to 25% of college students
reported being confused about real versus dreamed events. Studies suggest
that people who are fantasy-prone are more likely to experience source
monitoring
errors, [13] and
such errors also occur more often for both children and the elderly than
for adolescents and younger
adults. [14]
In other cases, we may be sure that we remembered the information from
real life but be uncertain about exactly where we heard it. Imagine that
you read a news story in a tabloid magazine such as the National Enquirer. Probably you would have
discounted the information because you know that its source is
unreliable. But what if later you were to remember the story but forget
the source of the information? If this happens, you might become
convinced that the news story is true because you forget to discount it.
The sleeper effect refers to an attitude change that occurs over time when we forget the source of
information. [15]
In still other cases we may forget where we learned information and
mistakenly assume that we created the memory ourselves. Kaavya
Viswanathan, the author of the book How Opal Mehta Got
Kissed, Got Wild, and Got a Life, was accused of plagiarism when
it was revealed that many parts of her book were very similar to passages
from other material. Viswanathan argued that she had simply forgotten
that she had read the other works, mistakenly assuming she had made up
the material herself. And the musician George Harrison claimed that he
was unaware that the melody of his song “My Sweet Lord” was almost
identical to an earlier song by another composer. The judge in the
copyright suit that followed ruled that Harrison didn’t intentionally
commit the plagiarism. (Please use this knowledge to become extra
vigilant about source attributions in your written work, not to try to
excuse yourself if you are accused of plagiarism.)
Overconfidence
Research reveals a
pervasive cognitive bias toward overconfidence,
which is the tendency for people to be too certain
about their ability to accurately remember events and to make
judgments. David Dunning and his
colleagues [16]
asked college students to predict how another student would react in
various situations. Some participants made predictions about a fellow
student whom they had just met and interviewed, and others made
predictions about their roommates whom they knew very well. In both
cases, participants reported their confidence in each prediction, and
accuracy was determined by the responses of the people themselves. The
results were clear: Regardless of whether they judged a stranger or a
roommate, the participants consistently overestimated the accuracy of
their own predictions.
Eyewitnesses to crimes are also frequently overconfident in their memories, and there
is only a small correlation between how accurate and how confident an eyewitness is.
A witness who claims to be absolutely certain about, for example, his or her
identification of a suspect or account of events is
not much more likely to be accurate than one who appears less sure, making it almost
impossible to determine whether or not a particular witness is accurate. [17]
I am sure that you have a clear memory of when you first heard about the
9/11 attacks in 2001, and perhaps also when you heard that Princess Diana
was killed in 1997 or when the verdict of the O. J. Simpson trial was
announced in 1995. This type of memory, which we experience along with a
great deal of emotion, is known as a flashbulb
memory—a vivid and emotional memory of an
unusual event that people believe they remember very
well. [18]
People are very certain of their memories of these important events, and frequently
overconfident. Talarico and Rubin [19] tested the accuracy of flashbulb memories by asking
students to write down their memory of how they had heard the news about either the
September 11, 2001, terrorist attacks or about an everyday event that had occurred to
them during the same time frame. These recordings were made on September 12, 2001.
Then the participants were asked again, either 1, 6, or 32 weeks later, to recall
their memories. The participants became less accurate in their recollections of both
the emotional event and the everyday events over time. But the participants’
confidence in the accuracy of their memory of learning about the attacks did not
decline over time. After 32 weeks, the participants were overconfident; they were
much more certain about the accuracy of their flashbulb memories than they should
have been. Schmolck, Buffalo, and Squire [20] found similar distortions in memories of news about
the verdict in the O. J. Simpson trial.
References
- Erdmann, K., Volbert, R., and Böhm, C.
(2004).
"Children report suggested events even when interviewed in a
non-suggestive manner: What are its implications for credibility
assessment?." Applied Cognitive Psychology. Volume 18. Number 8. 589–611
Pages.
- Loftus, E. F.
(1979).
"The malleability of human memory." American Scientist. Volume 67. Number 3. 312–320 Pages.
- Zaragoza, M. S., Belli, R. F., and Payment, K. E.
(2007).
Do Justice and Let the Sky Fall: Elizabeth Loftus and Her Contributions to Science, Law, and Academic Freedom.
Chapter Misinformation effects and the suggestibility of eyewitness
memory. Lawrence Erlbaum. Mahwah, NJ. 35–63 Pages. M. Garry and H. Hayne
(Eds.).
- Loftus, E. F., and Palmer, J. C.
(1974).
"Reconstruction of automobile destruction: An example of the
interaction between language and memory." Journal of Verbal Learning and
Verbal Behavior. Volume 13. Number 5. 585–589 Pages.
- Ceci, S. J., Huffman, M. L. C., Smith, E., and
Loftus, E. F.
(1994).
"Repeatedly thinking about a non-event: Source misattributions
among preschoolers." Consciousness and Cognition: An International
Journal. Volume 3. Number 3–4. 388–407 Pages.
- Loftus, E. F., and Pickerell, J. E.
(1995).
"The formation of false memories." Psychiatric Annals. Volume 25. Number 12. 720–725 Pages.
- Mazzoni, G. A. L., Loftus, E. F., and
Kirsch, I.
(2001).
"Changing beliefs about implausible autobiographical events: A
little plausibility goes a long way." Journal of Experimental
Psychology: Applied. Volume 7. Number 1. 51–59 Pages.
- Brown, D., Scheflin, A. W., and Hammond, D. C.
(1998).
Memory, Trauma Treatment, and the Law. Norton. New York.
- McNally, R. J., Bryant, R. A., and Ehlers,
A.
(2003).
"Does early psychological intervention promote recovery from
posttraumatic stress?." Psychological Science in the Public Interest.
Volume 4. Number 2. 45–79 Pages.
- Pope, H. G., Jr., Poliakoff, M. B., Parker, M.
P., Boynes, M., and Hudson, J. I.
(2007).
"Is dissociative amnesia a culture-bound syndrome? Findings from a
survey of historical literature." Psychological Medicine: A Journal of
Research in Psychiatry and the Allied Science. Volume 37. Number 2.
225–233 Pages.
- Loftus, E. F., and Ketcham, K.
(1994).
The Myth of Repressed Memory: False Memories and Allegations of Sexual Abuse. St. Martin’s Press. New York.
- Rassin, E., Merckelbach, H., and Spaan, V.
(2001).
"When dreams become a royal road to confusion: Realistic dreams,
dissociation, and fantasy proneness." Journal of Nervous and Mental
Disease. Volume 189. Number 7. 478–481 Pages.
- Winograd, E., Peluso, J. P., and Glover, T.
A.
(1998).
"Individual differences in susceptibility to memory illusions."
Applied Cognitive Psychology. Volume 12. Number Special issue. S5–S27
Pages.
- Jacoby, L. L., and Rhodes, M. G.
(2006).
"False remembering in the aged." Current Directions in Psychological Science. Volume 15. Number 2. 49–53 Pages.
- Pratkanis, A. R., Greenwald, A. G.,
Leippe, M. R., and Baumgardner, M. H.
(1988).
"In search of reliable persuasion effects: III. The sleeper effect
is dead: Long live the sleeper effect." Journal of Personality and
Social Psychology. Volume 54. Number 2. 203–218 Pages.
- Dunning, D., Griffin, D. W., Milojkovic, J.
D., and Ross, L.
(1990).
"The overconfidence effect in social prediction." Journal of
Personality and Social Psychology. Volume 58. Number 4. 568–581 Pages.
- Wells, G. L., and Olson, E. A.
(2003).
"Eyewitness testimony." Annual Review of Psychology. Volume 54. Number 1. 277–295 Pages.
- Brown, R., and Kulik, J.
(1977).
"Flashbulb memories." Cognition. Volume 5. Number 1. 73–99 Pages.
- Talarico, J. M., and Rubin, D. C.
(2003).
"Confidence, not consistency, characterizes flashbulb memories."
Psychological Science. Volume 14. Number 5. 455–461 Pages.
- Schmolck, H., Buffalo, E. A., and Squire,
L. R.
(2000).
"Memory distortions develop over time: Recollections of the O. J.
Simpson trial verdict after 15 and 32 months." Psychological Science.
Volume 11. Number 1. 39–45 Pages.
Confirmation Bias
If you’ve already covered the unit on how cognitive change proceeds in childhood,
this paragraph and the following Learn By Doing exercise will be a quick refresher on
schematic processing. If that material is yet to come, then this will serve as a
brief introduction to the topic. Schemata (plural of schema)
are mental representations of the world that are formed and
adjusted using the processes of assimilation and accommodation as a person
experiences life. Assimilation is the use of existing schema to interpret new
information and accommodation is the adjustment of existing schema to fit new
information. Generally, both processes are in action at the same time.
We have seen that schemas help us remember information by organizing material into
coherent representations. However, although schemas can improve our memories, they
may also lead to cognitive biases. Using schemas may lead us to falsely remember
things that never happened to us and to distort or misremember things that did. For
one, schemas lead to the confirmation bias, which is the tendency to verify and confirm our existing memories rather
than to challenge and disconfirm them. The confirmation bias occurs because
once we have schemas, they influence how we seek out and interpret new information.
The confirmation bias leads us to remember information that fits our schemas better
than we remember information that disconfirms them, [1] a process that makes our
stereotypes very difficult to change. And we ask questions in ways that confirm our
schemas. [2] If we think that a person is
an extrovert, we might ask her about ways that she likes to have fun, thereby making
it more likely that we will confirm our beliefs. In short, once we begin to believe
in something—for instance, a stereotype about a group of people—it becomes very
difficult to later convince us that these beliefs are not true; the beliefs become
self-confirming.
Darley and Gross [3] demonstrated
how schemas about social class could influence memory. In their research they gave
participants a picture and some information about a fourth-grade girl named Hannah.
To activate a schema about her social class, Hannah was pictured sitting in front of
a nice suburban house for one-half of the participants and pictured in front of an
impoverished house in an urban area for the other half. Then the participants watched
a video that showed Hannah taking an intelligence test. As the test went on, Hannah
got some of the questions right and some of them wrong, but the number of correct and
incorrect answers was the same in both conditions. Then the participants were asked
to remember how many questions Hannah got right and wrong. Demonstrating that
stereotypes had influenced memory, the participants who thought that Hannah had come
from an upper-class background remembered that she had gotten more correct answers
than those who thought she was from a lower-class background.
Our reliance on schemas can also make it more difficult for us to “think outside the
box.” Peter Wason [4] asked
college students to determine the rule that was used to generate the numbers 2-4-6 by
asking them to generate possible sequences and then telling them if those numbers
followed the rule. The first guess that students made was usually “consecutive
ascending even numbers,” and they then asked questions designed to confirm their
hypothesis (“Does 102-104-106 fit?” “What about 404-406-408?”). Upon receiving
information that those guesses did fit the rule, the students stated that the rule
was “consecutive ascending even numbers.” But the students’ use of the confirmation
bias led them to ask only about instances that confirmed their hypothesis, and not
about those that would disconfirm it. They never bothered to ask whether 1-2-3 or
3-11-200 would fit, and if they had, they would have learned that the rule was not
“consecutive ascending even numbers” but simply “any three ascending numbers.” Again,
you can see that once we have a schema (in this case a hypothesis), we continually
retrieve that schema from memory rather than other relevant ones, leading us to act
in ways that tend to confirm our beliefs.
Functional Fixedness
Functional fixedness occurs when people’s schemas prevent them
from using an object in new and nontraditional ways. Duncker [5] gave participants a candle, a
box of thumbtacks, and a book of matches, and asked them to attach the candle to the
wall so that it did not drip onto the table below
. Few of the participants realized that
the box could be tacked to the wall and used as a platform to hold the candle. The
problem again is that our existing memories are powerful, and they bias the way we
think about new information. Because the participants were “fixated” on the box’s
normal function of holding thumbtacks, they could not see its alternative use.
Salience and Selective Memory
Still another potential for bias in memory occurs because we are more likely to
attend to, and thus make use of and remember, some information more than other
information. For one, we tend to attend to and remember things that are highly salient, meaning that they attract our attention. Things that
are unique, colorful, bright, moving, and unexpected are more salient. [6] [7]
In one relevant study, Loftus, Loftus, and Messo [8] showed people images of a customer walking up to a
bank teller and pulling out either a pistol or a checkbook. By tracking eye
movements, the researchers determined that people were more likely to look at the gun
than at the checkbook, and that this reduced their ability to accurately identify the
criminal in a lineup that was given later. The salience of the gun drew people’s
attention away from the face of the criminal.
The salience of the stimuli in our social worlds has a big influence on our judgment,
and in some cases may lead us to behave in ways that we might better not have.
Imagine, for instance, that you wanted to buy a new music player for yourself. You’ve
been trying to decide what brand of tablet computer to buy. You checked Consumer Reports online and found that, although the brands
differed on many dimensions, including price, battery life, and so forth, Brand X was
nevertheless rated significantly higher by owners than were the other brands. As a
result, you decide to purchase Brand X the next day. That night, however, you go to a
party, and a friend shows you her new Brand Y tablet. You check it out, and it seems
really cool. You tell her that you were thinking of buying Brand X, and she tells you
that you are crazy. She says she knows someone who had one and it had a lot of
problems—it didn’t download files correctly, the battery died right after the
warranty expired, and so forth—and that she would never buy one. Would you still buy
Brand X, or would you switch your plans?
If you think about this question logically, the information that you just got from
your friend isn’t really all that important. You now know the opinion of one more
person, but that can’t change the overall rating of the brands very much. On the
other hand, the information your friend gives you, and the chance to use her Brand Y
tablet, are highly salient. The information is right there in front of you, in your
hand, whereas the statistical information from Consumer
Reports is only in the form of a table that you saw on your computer. The
outcome in cases such as this is that people frequently ignore the less salient but
more important information, such as the likelihood that events occur across a large
population (these statistics are known as base rates), in
favor of the less important but nevertheless more salient information. The situation
is further complicated by the fact that people tend to selectively remember certain
outcomes because they are salient while disregarding mundane ones. Moreover, people’s
first person perspective leads them to overestimate the degree to which they played a
role in an event or project, a phenomenon called cognitive accessibility.
References
- Stangor, C., and McMillan, D.
(1992).
"Memory for expectancy-congruent and expectancy-incongruent
information: A
review of the social and social developmental
literatures." Psychological Bulletin. Volume 111. Number 1. 42–61 Pages.
- Trope, Y., and Thompson, E.
(1997).
"Looking for truth in all the wrong places? Asymmetric search of
individuating
information about stereotyped group members." Journal of
Personality and Social Psychology. Volume 73. Number 2. 229–241 Pages.
- Darley, J. M., and Gross, P. H.
(1983).
"A hypothesis-confirming bias in labeling effect." Journal of
Personality and Social Psychology. Volume 44. Number 1. 20–33 Pages.
- Wason, P.
(1960).
"On the failure to eliminate hypotheses in a conceptual task."
Quarterly Journal of Experimental Psychology. Volume 12. Number 3.
129–140 Pages.
- Duncker, K., and Lees, L. S.
(1945).
"On problem-solving." Psychological Monographs. Volume 58. Number 5. i-113 Pages.
- McArthur, L. Z., and Post, D. L.
(1977).
"Figural emphasis and person perception." Journal of Experimental Social Psychology. Volume 13. Number 6. 520–535 Pages.
- Taylor, S. E., and Fiske, S. T.
(1978).
Advances in Experimental Social Psychology, Vol. 11. Chapter Salience, attention and attribution: Top of the head
phenomena. Academic Press. New York. 249–288 Pages. L. Berkowitz (Ed.).
- Loftus, E. F., Loftus, G. R., and Messo, J.
(1987).
"Some facts about weapon focus." Law and Human Behavior. Volume 11. Number 1. 55–62 Pages.
Heuristics, Probability, and the Gambler's Fallacy
Another way that our information processing may be biased occurs when we use heuristics, which are information-processing
strategies that are useful in many cases but may lead to errors when
misapplied. These strategies are in contrast to algorithms, which are recipe-style information-processing
strategies that guarantee a correct answer at all times. Two examples are
using the Pythagorean theorem for finding the length of the hypotenuse of a triangle
and using a formula to convert from Fahrenheit to Celsius (and vice versa), and there
are many others. The reason that people don’t always use algorithmic processing
is that there are not algorithmic solutions to most problems people encounter (or
even if there were, they may be too complicated), thus they resort to heuristics as
the next best alternative. Let’s consider two of the most frequently applied (and
misapplied) heuristics: the representativeness heuristic and
the availability heuristic.
In many cases we base our judgments on information that seems to
represent, or match, what we expect will happen, while ignoring other potentially
more relevant statistical information. When we do so, we are using the representativeness heuristic. Consider, for instance, the puzzle
presented in the following
table. Let’s say that
you went to a hospital, and you checked the records of the babies that were born
today. Which pattern of births do you think you are most likely to find?
| The Representativeness Heuristic |
|---|
| Adapted from Flat World Knowledge, Introduction to
Psychology, v1.0, CC-BY-NC-SA. |
| List A Time |
List A Gender |
List B Time |
List B Gender |
| 6:31 a.m. |
Girl |
6:31 a.m. |
Boy |
| 8:15 a.m. |
Girl |
8:15 a.m. |
Girl |
| 9:42 a.m. |
Girl |
9:42 a.m. |
Boy |
| 1:13 p.m. |
Girl |
1:13 p.m. |
Girl |
| 3:39 p.m. |
Boy |
3:39 p.m. |
Girl |
| 5:12 p.m. |
Boy |
5:12 p.m. |
Boy |
| 7:42 p.m. |
Boy |
7:42 p.m. |
Girl |
| 11:44 p.m. |
Boy |
11:44 p.m. |
Boy |
|
Using the representativeness heuristic may lead us to incorrectly believe that some
patterns of observed events are more likely to have occurred than others. In this case,
list B seems more random, and thus is judged as more likely to have occurred, but
statistically both lists are equally likely.
Most people think that list B is more likely, probably because list B looks more random,
and thus matches (is “representative of”) our ideas about randomness. But statisticians
know that any pattern of four girls and four boys is mathematically equally likely. The
problem is that we have a schema of what randomness should be like, which doesn’t always
match what is mathematically the case. Similarly, people who see a
flipped coin come up “heads” five times in a row will frequently predict, and perhaps
even wager money, that “tails” will be next. This behavior is known as the gambler’s fallacy. But mathematically, the gambler’s fallacy is an
error: The likelihood of any single coin flip being “tails” is always 50%, regardless of
how many times it has come up “heads” in the past. Probability, the
likelihood of something happening, is calculated solely by
dividing the total number of potential favorable outcomes by the total number of possible
outcomes (in our case ½ for both heads and tails). The previous history of events does not
affect future events. Another illustration of the gambler’s fallacy is the deceptive
phenomenon of streaky basketball shooters.
learn by doing
Imagine you are at a Laker game and are watching Dwight Howard shooting free throws.
Let’s assume he generally makes 6 out of 10 shots, so his accuracy is 60%. As the
game goes on, the other team continues to foul Dwight, so he takes many free throws
throughout the game. You start to wonder what are the chances of him making a certain
number of shots. You remember from your math class that one needs to multiply
individual probabilities of events together to calculate their combined
probability.
Our judgments can also be influenced by how easy it is to retrieve a memory.The tendency to make judgments of the frequency or likelihood that an
event occurs on the basis of the ease with which it can be retrieved from memory is
known as the availability heuristic. [1] [2]
Imagine, for instance, that I asked you to indicate whether there are more words in the
English language that begin with the letter “R” or that have the letter “R” as the third
letter. You would probably answer this question by trying to think of words that have each
of the characteristics, thinking of all the words you know that begin with “R” and all that
have “R” in the third position. Because it is much easier to retrieve words by their first
letter than by their third, we may incorrectly guess that there are more words that begin
with “R,” even though there are in fact more words that have “R” as the third letter.
The availability heuristic may also operate on episodic memory. We may think that our
friends are nice people, because we see and remember them primarily when they are around us
(their friends, who they are, of course, nice to). And the traffic might seem worse in our
own neighborhood than we think it is in other places, in part because nearby traffic jams
are more easily retrieved than are traffic jams that occur somewhere else.
Counterfactual Thinking
In addition to influencing our judgments about ourselves and others, the ease with
which we can retrieve potential experiences from memory can have an important effect
on our own emotions. If we can easily imagine an outcome that is better than what
actually happened, then we may experience sadness and disappointment; on the other
hand, if we can easily imagine that a result might have been worse than what actually
happened, we may be more likely to experience happiness and satisfaction. The tendency to think about and experience events according to
“what might have been” is known as counterfactual thinking. [3] [4]
Imagine, for instance, that you were participating in an important contest, and you
won the silver (second-place) medal. How would you feel? Certainly you would be happy
that you won the silver medal, but wouldn’t you also be thinking about what might
have happened if you had been just a little bit better—you might have won the gold
medal! On the other hand, how might you feel if you won the bronze (third-place)
medal? If you were thinking about the counterfactuals (the
“what might have beens”) perhaps the idea of not getting any medal at all would have
been highly accessible; you’d be happy that you got the medal that you did get,
rather than coming in fourth.
Tom Gilovich and his colleagues investigated this idea by videotaping the responses
of athletes who won medals in the 1992 Summer Olympic Games. [5]
They videotaped the athletes both as they learned that they had won a silver or a
bronze medal and again as they were awarded the medal. Then the researchers showed
these videos, without any sound, to raters who did not know which medal which athlete
had won. The raters were asked to indicate how they thought the athlete was feeling,
using a range of feelings from “agony” to “ecstasy.” The results showed that the
bronze medalists were, on average, rated as happier than were the silver medalists.
In a follow-up study, raters watched interviews with many of these same athletes as
they talked about their performance. The raters indicated what we would expect on the
basis of counterfactual thinking—the silver medalists talked about their
disappointments in having finished second rather than first, whereas the bronze
medalists focused on how happy they were to have finished third rather than
fourth.
You might have experienced counterfactual thinking in other situations. Once I was
driving across country, and my car was having some engine trouble. I really wanted to
make it home when I got near the end of my journey; I would have been extremely
disappointed if the car broke down only a few miles from my home. Perhaps you have
noticed that once you get close to finishing something, you feel like you really need
to get it done. Counterfactual thinking has even been observed in juries. Jurors who
were asked to award monetary damages to others who had been in an accident offered
them substantially more in compensation if they barely avoided injury than they
offered if the accident seemed inevitable. [6]
Psychology in Everyday Life: Cognitive Biases in the Real World
Perhaps you are thinking that the kinds of errors that we have been talking about
don’t seem that important. After all, who really cares if we think there are more
words that begin with the letter “R” than there actually are, or if bronze medal
winners are happier than the silver medalists? These aren’t big problems in the
overall scheme of things. But it turns out that what seem to be relatively small
cognitive biases on the surface can have profound consequences for people.
Why would so many people continue to purchase lottery tickets, buy risky investments
in the stock market, or gamble their money in casinos when the likelihood of them
ever winning is so low? One possibility is that they are victims of salience; they
focus their attention on the salient likelihood of a big win, forgetting that the
base rate of the event occurring is very low. The belief in astrology, which all
scientific evidence suggests is not accurate, is probably driven in part by the
salience of the occasions when the predictions are correct. When a horoscope comes
true (which will, of course, happen sometimes), the correct prediction is highly
salient and may allow people to maintain the overall false belief.
People may also take more care to prepare for unlikely events than for more likely
ones, because the unlikely ones are more salient. For instance, people may think that
they are more likely to die from a terrorist attack or a homicide than they are from
diabetes, stroke, or tuberculosis. But the odds are much greater of dying from the
latter than the
former.
Salience and accessibility also color how we perceive our social worlds, which may
have a big influence on our behavior. For instance, people who watch a lot of violent
television shows also view the world as more dangerous, [7] probably
because violence becomes more cognitively accessible for them. We also unfairly
overestimate our contribution to joint projects, [8]
perhaps in part because our own
contributions are highly accessible, whereas the contributions of others are much
less so.
Even people who should know better, and who need to know
better, are subject to cognitive biases. Economists, stock traders, managers,
lawyers, and even doctors make the same kinds of mistakes in their professional
activities that people make in their everyday lives. [9]
Just like us,
these people are victims of overconfidence, heuristics, and other biases.
Furthermore, every year thousands of individuals, such as Ronald Cotton, are charged
with and often convicted of crimes based largely on eyewitness evidence. When
eyewitnesses testify in courtrooms regarding their memories of a crime, they often
are completely sure that they are identifying the right person. But the most common
cause of innocent people being falsely convicted is erroneous eyewitness
testimony. [10] The many people who
were convicted by mistaken eyewitnesses prior to the advent of forensic DNA and who
have now been exonerated by DNA tests have certainly paid for all-too-common memory
errors. [11]
Although cognitive biases are common, they are not impossible to control, and
psychologists and other scientists are working to help people make better decisions.
One possibility is to provide people with better feedback about their judgments.
Weather forecasters, for instance, learn to be quite accurate in their judgments
because they have clear feedback about the accuracy of their predictions. Other
research has found that accessibility biases can be reduced by leading people to
consider multiple alternatives rather than focus only on the most obvious ones, and
particularly by leading people to think about opposite possible outcomes than the
ones they are expecting. [12]
Forensic psychologists are also working to reduce the incidence of false
identification by helping police develop better procedures for interviewing both
suspects and eyewitnesses. [13]
Belief in the Paranomal (Psi)
Another source of errors in cognition is belief in the paranormal. A Gallup poll in
2005 showed that 3 out of 4 Americans believe in the supernatural with over 40%
responding that they believe in extra-sensory perception (ESP), the ability to sense
things without being in physical proximity with the person, place, thing, or event.
There has been much research that has claimed to prove or disprove the existence of
such phenomena. While the paranomal is taken for granted by the general public, quite
the opposite is observed in the American Academy of Sciences, where only 4% members
believe in the existence of such phenomena.
The paranormal is a term that most people use to refer to a whole range of unusual
aspects of human perception and cognition. Parapsychologists, scientists that study
anomalous phenomena like ESP, generally use the term Psi, and have identified two
specific forms. Psi-gamma refers to those phenomena that involve anomalous
information transfer, like ESP, clairvoyance, and remote viewing. On the other hand,
psi-kappa refers to those phenomena that involve anomalous transfer of matter, such
as psychokinesis or telekinesis (the ability to move things with one’s mind), or even
anomalous transfer of energy, such as pyrokinsesis (the ability to set things aflame
with one’s mind). To date, the most rigorous set of studies were conducted at the
Princeton Engineering Anomalies Research (PEAR) at Princeton University. Despite
three decades of positive results, this research has not been accepted as a valid
avenue of empirical investigation by the mainstream scientific community. [14]
References
- MacLeod, C., and Campbell, L.
(1992).
"Memory accessibility and probability judgments: An experimental evaluation of
the availability heuristic." Journal of Personality and Social Psychology. Volume 63. Number 6. 890–902 Pages.
- Tversky, A., and Kahneman, D.
(1973).
"Availability: A heuristic for judging frequency and probability."
Cognitive Psychology. Volume 5. Number 2. 207–232 Pages.
- Kahneman, D., and Miller, D. T.
(1986).
"Norm theory: Comparing reality to its alternatives." Psychological Review. Volume 93. Number 2. 136–153 Pages.
- Roese, N.
(2005).
If Only: How to Turn Regret into Opportunity. Broadway Books. New York.
- Medvec, V. H., Madey, S. F., and Gilovich, T.
(1995).
"When less is more: Counterfactual thinking and satisfaction among Olympic
medalists." Journal of Personality and Social Psychology. Volume 69. Number 4. 603–610 Pages.
- Miller, D. T., Turnbull, W., and McFarland, C.
(1988).
"Particularistic and universalistic evaluation in the social comparison
process." Journal of Personality and Social Psychology. Volume 55. Number 6. 908–917 Pages.
- Doob, A. N., and MacDonald, G. E.
(1979).
"Television viewing and fear of victimization: Is the relationship
causal?." Journal of Personality and Social Psychology. Volume 37. Number 2. 170–179 Pages.
- Ross, M., and Sicoly, F.
(1979).
"Egocentric biases in availability and attribution." Journal of
Personality and Social Psychology. Volume 37. Number 3. 322–336 Pages.
- Gilovich, T., Griffin, D., and Kahneman, D.
(2002).
Heuristics and Biases: The Psychology of Intuitive Judgment. Cambridge University Press. New York.
- Wells, G. L., Wright, E. F., and Bradfield, A. L.
(1999).
Psychology and Law: The State of the Discipline.
Chapter Witnesses to crime: Social and cognitive factors governing the
validity of
people’s reports. Kluwer Academic Publishers. Dordrecht,
Netherlands. 53–87 Pages. R. Roesch, S. D. Hart, and J. R. P. Ogloff
(Eds.).
- Wells, G. L., Memon, A., and Penrod, S. D.
(2006).
"Eyewitness evidence: Improving its probative value." Psychological
Science in the Public Interest. Volume 7. Number 2. 45–75 Pages.
- Lilienfeld, S. O., Ammirati, R., and Landfield, K.
(2009).
"Giving debiasing away: Can psychological research on correcting cognitive
errors promote human welfare?." Perspectives on Psychological Science. Volume 4. Number 4. 390–398 Pages.
- Steblay, N., Dysart, J., Fulero, S., and Lindsay, R. C. L.
(2001).
"Eyewitness accuracy rates in sequential and simultaneous lineup
presentations: A meta-analytic comparison." Law and Human Behavior. Volume 25. Number 5. 459–473 Pages.
- Jahn, R., and Dunne, B.
(2009).
HMargins of Reality: The Role of Consciousness in the Physical World (2nd Ed). ICRL Press. Princeton, NJ.
Introduction: Language Comes in Many Forms
Virtually all animals have ways to communicate with other members of their own
species, whether it be through sounds, gestures, odors, or other means. Some animals,
like chimpanzees and dolphins, have rich and complicated communication systems. But
even the most sophisticated communication system of other species does not come close
to the complexity and subtlety of human language. It is not an exaggeration to claim
that the human language system takes communication to a very different level than
that found in any other creature on earth. Although the word language is often used broadly (e.g., “the language of the bees”), here we
restrict its use to a particular part of human communication—spoken language—and
consider it apart from other important aspects of human communication (e.g., body
language or emotional messages conveyed by facial expressions).
Language
involves both the ability to comprehend spoken and written words
and to produce meaningful communication when we speak or write. Most
languages first appear in their spoken form. Although speaking may seem simple, it is
a remarkably complex skill that involves a variety of cognitive, social, and
biological processes, including operation of the vocal cords and the coordination of
breath with movements of the throat, mouth, and tongue. A number of languages that
are primarily or entirely expressed in sign also exist. In sign languages,
communication is expressed by movements of the hands along with facial and bodily
gestures. The most common sign language is American Sign Language (ASL), currently
spoken by more than 500,000 people in the United States alone. Except for artificial
languages developed for technology and an occasional special-use language, languages
do not develop in written form. Although writing is generally derivative of spoken
language, it involves a complex set of processes, some of them unique to writing.
Language is often used for the transmission of factual information (“Turn right at
the next light, and then go straight,” “Place tab A into slot B”), but that is only
its most mundane function. Language also allows us to access existing knowledge, to
draw conclusions, to set and accomplish goals, and to understand and communicate
complex social relationships. Language is fundamental to our ability to think, and
without it we would be nowhere near as intelligent as we are.
Spoken languages can be conceptualized in terms of sounds, meaning, and the
environmental factors that help us understand it. Although we usually notice words
and sentences when we think about language, some of the most important psychological
research on language involves more basic elements that give form and content to words
and sentences. In the next section, we discuss phonemes, which are elementary units
of sound that make up words; morphemes, which are “word parts”—small but meaningful
sounds that alter and refine a word’s meaning; and finally, syntax, which is the set
of grammatical rules that control how words are put together into phrases and
sentences. Languages are governed by rules, but contextual information, the when,
where, and why of communication, is also necessary for understanding the meaning of
what a person says. The importance of context is also discussed in this section.
The Components of Language: Phonemes
A phoneme is the smallest unit of sound that
makes a meaningful difference in a language. Phonemes correspond to the
sounds associated with the letters of an alphabet, though there is not always a
one-to-one correspondence between sounds and letters. The word bit has three phonemes, /b/, /i/, and /t/ (in transcription, phonemes are
placed between slashes), and the word pit also has three:
/p/, /i/, and /t/. These two words differ by a single phoneme: /b/ versus /p/.
However, the six-letter word phrase has only four phonemes:
/f/, /r/, /long-a/, and /z/. In spoken languages, phonemes are produced by movements
of our lips, teeth, tongue, vocal cords, and throat (the vocal tract), whereas in
sign languages phonemes are defined by the shapes and movement of the hands.
Hundreds of unique phonemes can be made by human speakers, but most languages use
only a small subset of the possibilities. English uses about 45 phonemes, whereas
other languages have as few as 15 and others more than 60. For instance, the Hawaiian
language contains only about a dozen phonemes, including five vowels (a, e, i, o, and
u) and seven consonants (h, k, l, m, n, p, and w).
The fact that different languages use different sets of phonemes is the reason people
usually have accents in languages that are not their native language. It is difficult
to learn to make a new speech sound and use it regularly in words if you did not
learn it early in life. And accents are not the whole story. Because the phoneme is
actually a category of sounds—that is, many variations on a sound—and the members of
this category are treated alike by the brain, some languages group several sounds
together as a single phoneme, and others separate those same sounds as different
phonemes. Speakers of different languages can hear the difference only between the
sounds their language marks as different phonemes, and they cannot tell the
difference between two sounds that are grouped together as the same phoneme. This is
known as the categorical perception of speech sounds. For
example, English speakers can differentiate the /r/ phoneme from the /l/ phoneme, and
thus rake and lake are heard as
different words. In Japanese, however, /r/ and /l/ are the same phoneme, and thus
native speakers of Japanese cannot tell the difference between rake and lake. The /r/ versus /l/ difference is
obvious to native English speakers, but English speakers run into the same problem
when listening to speakers of other language. Try saying cool
and keep out loud. Can you hear the difference between the
two /k/ sounds? To English speakers, they both sound the same, but to speakers of
Arabic they are two different phonemes.
learn by doing
Let’s practice identifying the various components of language. The first part of this
activity focuses on phonemes, the smallest unit of sound. When you click the play
button, you will hear a speech sound. Your job is to drag and drop the grapheme, or
letter, of the phoneme you hear into the corresponding box.
Categorical Perception of Phonemes
Categorical perception is a way of
perceiving different sensory inputs and mapping them to the same category. It
explains why speakers of a particular language all group a variety of sounds into
a single phoneme, so each phoneme is actually a set of variations on a single
theme. This means that we hear different sounds as if they were the same, and
often we cannot tell the difference even if we try. To demonstrate this fact,
psychologists used computers to create a series of sounds, each made up of two
phonemes, that gradually—in precise steps—changed from a /ba/ sound to a /pa/ sound.
(Other two-phoneme sounds were tested as well, but we use /ba/ and /pa/ for our
explanation.)
The experimenters wanted to know what the people (in this case, adults) would
perceive when they heard the sounds. If you didn’t know about phonemes, you might
expect that they would hear a clear /ba/ sound that gradually became more like a /pa/
sound until it became a clear /pa/ sound. But that is not what happened.
The following figure shows the many variations of the /ba/ and /pa/ sounds on the
X-axis. The X-axis is labeled “Voice onset time (ms).” Voice onset time is a
technical unit, not critical for our discussion. Simply understand that the sounds,
created by a computer to guarantee precise differences, went from having strong
characteristics of /ba/ on the far left to strong characteristics of /pa/ on the far
right.
The two lines represent the percentage of participants who said they heard /pa/ and
the percentage who said they heard /ba/. Percentages are shown on the Y-axis.
Together the two lines add up to 100%, because participants always had to choose one
or the other. What the graph shows is that there was only a small region of
ambiguity, where the two lines cross. For most of the sounds, going left to right,
just about every participant on every trial chose either /ba/ on the left or /pa/ on
the right.
If the participants in the study had simply heard the differences, we would predice
that as the sounds became more mixed (this occurs the most in the very center of the
figure), the participants would be increasingly confused.
But that is not what happened. Instead, people perceived /ba/ unambiguously across
many variations. Then, in the center of the variations, where /ba/ and /pa/ sounds
were most mixed together, there was a bit of uncertainty, and then they unambiguously
heard /pa/ sounds. You can see this in the following figure, where there is only a
small range of sounds that led to any uncertainty about whether participants heard
/ba/ or /pa/. This sharp change from perceiving the sounds to be /ba/ to perceiving
the sounds to be /pa/ is called categorical perception, meaning that what we perceive
is far more sharply (or “categorically”) divided than what our ears actually
hear.
Infants are born able to understand all phonemes, but they lose their ability to do
so as they get older; by 10 months of age, a child’s ability to recognize phonemes
becomes similar to that of the adult speakers of the native language. Phonemes that
were initially differentiated come to be treated as equivalent. [1]
Morphemes
Phonemes are units of sound, but sound is simply used by language to convey meaning.
The basic meaningful units of words are called morphemes. A morpheme is a string of one or more phonemes that
make up word meanings and, if a morpheme is added, eliminated, or changed, the
meaning of the word changes. In some cases, an entire word is a morpheme. For
instance, the word painted has seven letters, six phonemes
(/p/, /long-a/, /n/, /t/, /e/, and /d/), and two morphemes (paint + ed, which is a morpheme that means that the
first morpheme occurred in the past). However, we can add morphemes—for instance, the
prefix re to make repainted—or
eliminate morphemes, taking the ed away to leave the single
morpheme word, paint. We can even add a morpheme to make up
new words, such as unrepainted or depainting, even if we aren’t quite sure what they mean. However, in
general, we know what the changed word means when we add a morpheme. For example, the
syllable re-, as in rewrite or repay, means “to do again,” and the suffix -est, as in happiest or coolest, means “to the maximum.”
learn by doing
In this activity, we look at morphemes, which consist of one or more phonemes.
un
over
dis
touch
agree
cook
ed
s
able
Syntax
Syntax is the set of rules of a language by
which we construct sentences. Each language has a different syntax. The
syntax of the English language requires that each sentence have a noun and a verb,
each of which may be modified by adjectives and adverbs. Some syntactical rules make
use of the order in which words appear, while others do not. In English, “The man
bites the dog” is different from “The dog bites the man.” Because the words are the
same in both sentences, the order of the words must convey the difference in meaning.
In German, however, only the article endings before the noun matter. “Der Hund beisst
den Mann” means “The dog bites the man” but so does “Den Mann beisst der Hund.” The
German word der goes with the subject of the sentence, while
den goes with the object. The order of the words in this
sentence is not as important as it would be in English.
learn by doing
In this activity, you create grammatical sentences. For each sentence, select the
word that best completes the sentence.
easily
armadillos
juicy
shelved
quickly
ordered
ripe
infants
The Importance of Context
Words, phrases, and entire sentences do not possess fixed meanings but change their
interpretation as a function of the context in which they are spoken. We use contextual information—the situation in which
language is being used, the topic, the things that were said previously, body
language, and so on—to help us interpret a word or sentence. For example,
imagine that you run into a friend who just saw a new high-tech movie and ask, “How
was it?” The friend replies with an enthusiastic look on his face, “Unbelievable!”
Now imagine that you run into a friend who just went to a lecture on “How to make a
million dollars in two days selling bottled air.” You ask, “How was it?” and your
friend rolls her eyes and groans, “Unbelievable!” In the first case, “unbelievable”
means “very good,” and in the second case, “unbelievable” means “very bad.” We use
context so naturally that we seldom notice how much it impacts our interpretation of
language.
Examples of contextual information include our own knowledge, our assumptions about
other people's knowledge, and nonverbal expressions such as facial expressions,
postures, gestures, and tone of voice. Misunderstandings can easily arise if people
aren’t attentive to contextual information or if some of it is missing, such as it
may be in newspaper headlines or in text messages.
Examples in Which Syntax Is Correct but the Interpretation Can Be
Ambiguous:
- Grandmother of Eight Makes Hole in One
- Milk Drinkers Turn to Powder
- Farmer Bill Dies in House
- Old School Pillars Are Replaced by Alumni
- Two Convicts Evade Noose, Jury Hung
- Include Your Children when Baking Cookies
learn by doing
Now let’s take a look at the role of contextual information in language. In English,
some words have multiple meanings. To determine which meaning of a word is the most
appropriate, we must consider contextual information. For each of the following
sentences, select which meaning of the italicized word is most appropriate given the
context.
did I get this
For each of the following definitions, select the language-related term it
describes.
References
- Werker, J. F., and Tees, R. C.
(2002).
"Cross-language speech perception: Evidence for perceptual
reorganization during the first year of life." Infant Behavior and
Development. Volume 25. Number 1. 121–133 Pages.
Anyone who has tried to master a second language as an adult knows the difficulty of
language learning. And yet children learn languages easily and naturally. Children who are
not exposed to language early in their lives will likely never learn one. Documented case
studies of such children include Victor the “Wild Child,” who was abandoned as a baby in
France and not discovered until he was 12, and Genie, a child whose parents kept her locked
in a closet from 18 months until 13 years of age. Both of these children made some progress
in socialization after they were rescued and even learned many words and simple phrases,
but neither of them ever developed language even to the level of a typical
3-year-old. [1]
The cases of Victor and Genie illustrate the importance of early experience of language
with people, usually adults, who are fluent in the language. There is one group of children
who are in danger of isolation even though they are born to completely normal and loving
families: congenitally deaf children or children who lose their hearing very early in life.
The parents of these children are seldom deaf themselves and often have no warning that
their newborn will be deaf. These parents are seldom fluent or even novices in sign
language, a language that, like any other language, takes years of practice to achieve
competency. Deaf children who are not exposed to sign language during their early years are
likely to have difficulty mastering it when they are
older. [2] Deaf children have a much better
chance of later acquiring other languages, even spoken languages, if they have early
exposure to fluent signing.
Deaf children and children like Victor and Genie have shown us that language is a complex
ability that is most likely to mature in a normal way if the child is raised in an
environment rich in language experiences. There is probably a “sensitive period,” usually
associated with the period of childhood, when exposure to language must occur for the brain
systems associated with language to develop properly. If exposure does not occur until
later, as happened to Genie and Victor and as once regularly happened to deaf children in
isolated communities, then the ability to acquire true language abilities may be extremely
difficult or even impossible. The brain may lose its ability to form the necessary neural
networks to permit language to develop.
For most people, language processing is dominated by the left hemisphere, but many people
have a reversal of this pattern, so the right hemisphere dominates language. For instance,
a study that looked at the relationship between handedness and the dominant hemisphere for
language found that only 4% of people who are strongly right handed have right hemisphere
dominance for language, while 15% of ambidextrous individuals and 27% of strong left
handers had right hemisphere dominance for language. [3]
These differences in hemispheric dominance can easily be seen in the results of
neuroimaging studies that show that listening to and producing language creates greater
activity in the left hemisphere than in the right. As shown in the following figure, the
Broca area, an area in front of the left
hemisphere near the motor cortex, is responsible for language production. This area
was first localized in the 1860s by the French physician Paul Broca, who studied patients
with lesions to various parts of the brain. The Wernicke area, an area of the brain next to the auditory cortex, is responsible for
language comprehension.
Evidence for the importance of the Broca and Wernicke areas in language is seen in patients
who experience aphasia, a condition in which language functions are severely impaired.
People with Broca aphasia have difficulty producing speech. They speak haltingly, using the
minimum number of words to convey an idea. Frequently, they struggle to say a word even
though they know the word they are looking for. Other times, they appear to search for a
word but fail to find it. People with damage to Wernicke area can produce speech, but what
they say is often confusing, and they have trouble understanding what other people are
saying to them. Wernicke aphasia is sometimes called fluent aphasia
because the person appears to speak in a relatively normal, fluent way, but the content of
the sentences may be imprecise or even nonsensical. People with both types of aphasia have
difficulty understanding what other people say to them, but this problem tends to be deeper
and more serious in cases of Wernicke aphasia. People with Broca aphasia may have
comprehension problems because they have difficulty understanding a particular word here
and there, but people with Wernicke aphasia have trouble making sense of the meaning of
entire sentences and also may have trouble keeping track of the point of the
conversation.
learn by doing
The following video shows one man who suffers from Wernicke aphasia and another man
who suffers from Broca aphasia. Watch the video and take note of the speech behaviors
that are characteristic to each man’s type of aphasia.
Now that you’ve seen examples of people with damage to the Wernicke and Broca areas,
let’s see if you can match the area of the brain to its appropriate role in
language.
did I get this
Let’s see how well you remember the parts of the brain that are important
for language.
References
- Rymer, R.
(1993).
Genie: An abused Child’s Flight from Silence. HarperCollins. New York.
- Mayberry, R. I., Lock, E., and Kazmi, H.
(2002).
"Development: Linguistic ability and early language exposure." Nature. Volume 417. Number 6884. 38 Pages.
- Knecht, S., Dräger, B., Deppe, M., Bobe, L., Lohmann, H., Flöel, A., et al.
(2000).
"Handedness and hemispheric language dominance in healthy humans." Brain. Volume 123. Number 12. 2512 Pages.
Learning Language
Language learning begins even before birth, because the fetus can hear muffled
versions of speaking from outside the womb. Moon, Cooper, and Fifer [1]
found that infants only two days old sucked harder on a
pacifier when they heard their mother's native language being spoken than when
they heard a foreign language, even when both the native and foreign languages
were spoken by strangers. Babies are also aware of the patterns of their native
language, showing surprise when they hear speech that has a different pattern of
phonemes than those they are used to. [2]
During the first year or so after birth, and long before they speak their first
words, infants are already learning language. One aspect of this learning is
practice in producing speech. By the time they are 6 to 8 weeks old, babies
start making vowel sounds, called cooing (“ooohh,”
“aaahh,” “goo”) as well as a variety of cries and squeals to help them
practice.
Between 5 and 7 months of age, most infants begin babbling,
engaging in intentional vocalizations that lack specific
meaning. Babbling sounds usually involve a combination of consonant and
vowel sounds. In the early months these sounds are often simple consonant vowel
pairs that are repeated, such as guh-guh-guy or ba-ba. This is called repetitive babbling. Over the next few months, the sound
combinations become more complex, with different consonants and vowels mixed
together, such as ma-ba-guh or aah-ga-mee. This is called variegated
babbling.
Children seem to be naturally motivated to make speech sounds, because they will
often vocalize when they are alone and not in distress. This natural motivation
has an important function because it encourages the baby to practice making and
distinguishing speech sounds, a skill that will be very important as language
emerges.
Babbling
can also serve an important social function for the infant. Parents and infants
frequenty engage in "conversational exchanges" of sounds, where the adult will
say something to the child, such as "You're such a sweet baby, yes you are, such a sweet
baby." The infant will watch and listen and then, when it is his or her turn,
make a babbling response. This can be an enjoyable interaction between adult and
infant, serving a bonding function, and it also allows the infant to practice
the skills of conversation prior to the appearance of words and sentences.
On the average, infants produce their first word at around 1 year of age. There
is a great deal of variability in the timing of first words, so some children
may start months earlier and others may not utter a distinguishable first word
for another 6 months or more. The timing of first words typically has no
relationship to later language abilities, though it is true that some disorders
can lead to a delay in speech production.
At the same time infants are practicing their speaking skills by babbling, they
are also learning to better understand sounds and eventually the words of
language. One of the first words children understand is their own name, usually
by about 6 months, followed by commonly used words like bottle, mama, and doggie by 10 to 12 months. [3]
At about 1 year of age, children begin to understand that words are more than
sounds—they refer to particular objects and ideas. By the time children are 2
years old, they have a vocabulary of several hundred words, and by kindergarten,
their vocabularies have increased to several thousand words. During the first
decade of life, pronunciation of phonemes becomes increasingly precise (and
understandable), and the use of morphemes and syntax becomes increasingly
sophisticated.
The early utterances of children contain many errors, for instance, confusing /b/
and /d/, or /c/ and /z/. And the words that children create are often
simplified, in part because they are not yet able to make the more complex
sounds of the real language. [4] Children may say “keekee” for
kitty, “nana” for banana, and “vesketti” for spaghetti, in part because it is
easier. Often these early words are accompanied by gestures that may also be
easier to produce than the words themselves.
Most of a child’s first words are nouns, and early sentences may include only the
noun. “Ma” may mean “more milk please,” and “da” may mean “look, there’s Fido.”
Eventually, typically by 18 months of age, the length of the utterances
increases to two words (“ma ma” or “da bark”), and these primitive sentences
begin to follow the appropriate syntax of the native language. By age 2, more
complex sentences start to appear, and there is rapid increase in vocabulary and
variations in language structure. Here, as was indicated earlier, there is a
great deal of variability among perfectly normal children in the timing of
language development, so a child who is ahead of the milestones discussed here
is not neceassarily going to remain advanced, and a child who misses them, even
by months, is not likely to remain behind his or her peers linguistically or
intellectually.
Because language involves the active categorization of sounds and words into
higher-level units, children make some mistakes in interpreting what words mean
and how to use them. In particular, they often make overextensions of concepts,
which means they use a given word in a broader context than appropriate. A child
might at first call all adult men “daddy” or all animals “doggie.”
Children also use contextual information, particularly the cues that parents
provide, to help them learn language. Infants are frequently more attuned to the
tone of voice of the person speaking than to the content of the words themselves
and are aware of the target of speech. Werker, Pegg, and McLeod [5] found that infants listened longer
to a woman who was speaking to a baby than to a woman who was speaking to
another adult. Children learn that people are usually referring to things that
they are looking at when they are speaking [6] and that the speaker’s emotional expressions are
related to the content of their speech. Children also use their knowledge of
syntax to help them figure out what words mean. If a child hears an adult point
to a strange object and say, “This is a dirb,” they will infer that a dirb is a thing, but if they hear them say, “This is one
of those dirb things,” they will infer that dirb refers
to the color or other characteristic of the object. And if they hear the word
“dirbing,” they will infer that dirbing is something we
do. [7]
References
- Moon, C., Cooper, R. P., and Fifer, W. P.
(1993).
"Two-day-olds prefer their native language." Infant Behavior and Development. Volume 16. Number 4. 495–500 Pages.
- Saffran, J. R., Aslin, R. N., and Newport, E. L.
(2004).
Statistical Learning by 8-Month-Old Infants. Psychology Press. New York.
- Mandel, D. R., Jusczyk, P. W., and Pisoni,
D. B.
(1995).
"Infants’ recognition of the sound patterns of their own names."
Psychological Science. Volume 6. Number 5. 314–317 Pages.
- Dobrich, W., and Scarborough, H. S.
(1992).
"Phonological characteristics of words young children try to
say." Journal of Child Language. Volume 19. Number 3. 597–616 Pages.
- Werker, J. F., Pegg, J. E., and McLeod, P. J.
(1994).
"A cross-language investigation of infant preference for infant-directed
communication." Infant Behavior and Development. Volume 17. Number 3. 323–333 Pages.
- Baldwin, D. A.
(1993).
"Early referential understanding: Infants’ ability to recognize
referential acts for what they are." Developmental Psychology. Volume 29. Number 5. 832–843 Pages.
- Waxman, S. R.
(1990).
"Linguistic biases and the establishment of conceptual hierarchies:
Evidence from preschool children." Cognitive Development. Volume 5. Number 2. 123–150 Pages.
Psychological theories of language learning differ in terms of the importance
they place on nature versus nurture. Yet it is clear that both matter. Children
are not born knowing language; they learn to speak by hearing what happens
around them. On the other hand, human brains, unlike those of any other animal,
are prewired in a way that leads them, almost effortlessly, to learn
language.
Perhaps the most straightforward explanation of language development is that it
occurs through principles of learning, including association, reinforcement,
and the observation of others. [1] There must be at
least some truth to the idea that language is learned, because children learn
the language that they hear spoken around them rather than some other language.
Also supporting this idea is the gradual improvement of language skills with
time. It seems that children modify their language through imitation,
reinforcement, and shaping, as would be predicted by learning theories.
But language cannot be entirely learned. For one, children learn words too fast for them to
be learned through reinforcement. Between the ages of 18 months and 5 years, children learn
up to 10 new words every day. [2] More important, language is more
generative than it is imitative. Generativity refers to the ability of speakers to compose sentences to represent new ideas they
have never before been exposed to. Language is not a predefined set of ideas and
sentences that we choose when we need them, but rather a system of rules and procedures
that allows us to create an infinite number of statements, thoughts, and ideas, including
those that have never previously occurred. When a child says that she “swimmed” in the
pool, for instance, she is showing generativity. An adult speaker of English would not say
“swimmed,” yet the word is easily generated from the normal system of producing
language.
Other evidence that refutes the idea that all language is learned through experience comes
from the observation that children may learn languages better than they ever hear them.
Deaf children whose parents do not speak American Sign Language very well nevertheless can
learn it perfectly on their own and may even make up their own language if they need
to. [3] A group of deaf children in a school
in Nicaragua, whose teachers could not sign, invented a way to communicate through made-up
signs and through signs different individuals had used to communicate with their own
families. [4] Within a few years, this
made-up signing system became increasingly rule governed and consistent. The development of
this new Nicaraguan Sign Language has continued and changed as new generations of students
have come to the school and started using the language. Although the original system was
not a real language, linguists now find that the signing system invented by these children
has all the typical features and complexity of a real language.
In the middle of the 20th century, American linguist Noam Chomsky explained how some
aspects of language could be innate. Prior to this time, people tended to believe that
children learn language soley by imitating the adults around them. Chomsky agreed that
individual words must be learned by experience, but he argued that genes could code into
the brain categories and organization that form the basis of grammatical structure. We come
into the world ready to distinguish different grammatical classes, like nouns and verbs and
adjectives, and sensitive to the order in which words are spoken. Then, using this innate
sensitivity, we quickly learn from listening to our parents about how to organize our own
language [5] [6] For instance, if we grow up hearing Spanish, we
learn that adjectives come after nouns (el gato amarillo, where gato means “cat” and amarillo is “yellow”),
but if we grow up hearing English, we learn that adjectives come first (“the yellow cat”).
Chomsky termed this innate sensitivity that allows infants and young children to organize
the abstract categories of language the language acquisition device
(LAD).
According to Chomsky’s approach, each of the many languages spoken around the
world (there are between 6,000 and 8,000) is an individual example of the same
underlying set of procedures that are hardwired into human brains. Each
language, while unique, is just a set of variations on a small set of possible
rule systems that the brain permits language to use. Chomsky’s account proposes
that children are born with a knowledge of general rules of grammar (including
phoneme, morpheme, and syntactical rules) that determine how sentences are
constructed.
Although there is general agreement among psychologists that babies are genetically
programmed to learn language, there is still debate about Chomsky’s idea that a universal
grammar can account for all language learning. Evans and Levinson [7]
surveyed the world’s languages and found that none of the presumed underlying features of
the language acquisition device were entirely universal. In their search they found
languages that did not have noun or verb phrases, that did not have tenses (e.g., past,
present, future), and some that did not have nouns or verbs at all, even though a basic
assumption of a universal grammar is that all languages should share these features. Other
psychologists believe that early experience can fully explain language acquisition, and
Chomsky’s language acquisition device is unnecessary. Nevertheless, Chomsky’s work clearly
laid out the many problems that had to be solved in order to adequately explain how
children acquire language and why languages have the structures that they do.
learn by doing
The two theories of language acquisition discussed in the text map to the nature
versus nurture distinction. Proponents of the nurture view, such as learning
theorists, maintain that language is, for the most part, acquired through principles
of learning. Supporters of the nature view, such as Noam Chomsky, believe that the
general foundation for grammatical parts of language is innate, though many important
aspects of language are learned. For each of the following statements, select either
Skinner’s learning theory or Chomsky’s LAD theory (LAD: language acquisition
device).
did I get this
Let’s ensure that you can identify the two theories of language acquisition discussed
in the text: Skinner’s learning theory and Chomsky’s LAD theory. For each statement,
select whether it is true or false.
References
- Skinner, B. F.
(1965).
Science and Human Behavior. Free Press. New York.
- Anglin, J. M.
(1993).
"Vocabulary development: A morphological analysis." Monographs of
the Society for Research in Child Development. Volume 58. Number 10.
v–165 Pages.
- Goldin-Meadow, S., and Mylander, C.
(1998).
"Spontaneous sign systems created by deaf children in two cultures." Nature. Volume 391. Number 6664. 279–281 Pages.
- Senghas, R. J., Senghas, A., and Pyers, J. E.
(2005).
Biology and Knowledge Revisited: From Neurogenesis to Psychogenesis.
Chapter The emergence of Nicaraguan Sign Language: Questions of
development, acquisition, and evolution. Lawrence Erlbaum Associates.
Mahwah, NJ. 287–306 Pages. S. T. Parker, J. Langer, and C. Milbrath
(Eds.).
- Chomsky, N.
(1965).
Aspects of the Theory of Syntax. MIT Press. Cambridge, MA.
- Chomsky, N.
(1972).
Language and Mind. Harcourt, Brace, Jovanovich. New York. Edition Extended.
- Evans, N., and Levinson, S. C.
(2009).
"The myth of language universals: Language diversity and its
importance for cognitive science." Behavioral and Brain Sciences. Volume
32. Number 66564. 429–448 Pages.
Although it is less common in the United States than in other countries, bilingualism (the ability to speak two languages) is becoming increasingly
frequent in the modern world. Nearly one-half of the world’s population, including 18% of
U.S. citizens, grows up bilingual.
In recent years, many U.S. states have passed laws outlawing bilingual education in
schools. These laws are in part based on the idea that students will have a stronger
identity with the school, the culture, and the government if they speak only English and in
part based on the idea that speaking two languages may interfere with cognitive
development.
Some early psychological research showed that, when compared with monolingual
children, bilingual children performed more slowly when processing language,
and their verbal scores were lower. But these tests were frequently given in
English, even when this was not the child’s first language, and the children
tested were often of lower socioeconomic status than the monolingual
children. [1]
More current research controlled for these factors and found that although bilingual
children may in some cases learn language somewhat more slowly than do monolingual
children [2] , bilingual and monolingual children do
not significantly differ in the final depth of language learning, nor do they generally
confuse the two languages. [3] In fact,
participants who speak two languages have been found to have better cognitive functioning,
cognitive flexibility, and analytic skills in comparison to
monolinguals. [4] Thus, rather than slowing language
development, learning a second language seems to increase cognitive abilities.
did I get this
Does bilingualism cause mental confusion? Is being bilingual a cognitive
advantage? People have debated these questions for a long time, but the
answers aren’t simple. For this exercise, please read a brief article that discusses the work of some of the
leading researchers in bilingualism. Then answer a few questions based on
your reading.
References
- Andrews, I.
(1982).
"Bilinguals out of focus: A critical discussion." International
Review of Applied Linguistics in Language Teaching. Volume 20. Number 4.
297–305 Pages.
- Oller, D. K., and Pearson, B. Z.
(2002).
Language and Literacy in Bilingual Children.
Chapter Assessing the effects of bilingualism: A background.
Multilingual Matters. Tonawanda, NY. 3–21 Pages. D. K. Oller and R. E.
Eilers (Eds.).
- Nicoladis, E., and Genesee, F.
(1997).
"Language development in preschool bilingual children." Journal of
Speech-Language Pathology and Audiology. Volume 21. Number 4. 258–270
Pages.
- Bialystok, E.
(2009).
"Bilingualism: The good, the bad, and the indifferent."
Bilingualism: Language and Cognition. Volume 12. Number 1. 3–11 Pages.
Nonhuman animals have a wide variety of systems of communication. Some species communicate
using scents; others use visual displays, such as baring the teeth, puffing up the fur, or
flapping the wings; and still others use vocal sounds. Male songbirds, such as canaries and
finches, sing songs to attract mates and to protect territory, and chimpanzees use a
combination of facial expressions, sounds, and actions, such as slapping the ground, to
convey aggression. [1] Honeybees use a “waggle dance” to direct
other bees to the location of food sources. [2] The language of
vervet monkeys is relatively advanced in the sense that they use specific sounds to
communicate specific meanings. Vervets make different calls to signify that they have seen
either a leopard, a snake, or a hawk. [3]
As mentioned earlier, despite the variety and sophistication of animal communication
systems, none comes close to human language in its ability to express a variety of ideas
and subtle differences in meaning. For years, scientists have wondered if it is the
communication systems that are limited or if other animals are simply unable to acquire a
system as advanced as human language. Quite a few efforts have been made to learn more by
attempting to teach human language to other animals, especially to chimpanzees and their
cousins, bonobos.
Despite their wide abilities to communicate, efforts to teach animals to use language have
had only limited success. One of the early efforts was made by Catherine and Keith Hayes,
who raised a chimpanzee named Viki in their home along with their own children. But Viki
learned little and could never speak. [4] Researchers speculated that Viki’s difficulties
might have been in part because the she could not create the words in her vocal cords, and
so subsequent attempts were made to teach primates to speak using sign language or using
boards on which they can point to symbols.
Allen and Beatrix Gardner worked for many years to teach a chimpanzee named Washoe to sign
using ASL. Washoe, who lived to be 42 years old, could label up to 250 different objects
and make simple requests and comments, such as “please tickle” and “me sorry.” [5] Washoe’s adopted daughter Loulis, who
was never exposed to human signers, learned more than 70 signs simply by watching her
mother sign.
The most proficient nonhuman language speaker is Kanzi, a bonobo who lives at the Language
Learning Center at Georgia State University. [6] As you can see in the following video
clip, Kanzi has a propensity for language that is in many ways similar to humans’. He
learned faster when he was younger than when he got older, he learns by observation, and he
can use symbols to comment on social interactions rather than simply for food treats. Kanzi
can also create elementary syntax and understand relatively complex commands. Kanzi can
make tools and can even play Pac-Man.
And yet even Kanzi does not have a true language in the same way that humans do. Human
babies learn words faster and faster as they get older, but Kanzi does not. Each new word
he learns is almost as difficult as the one before. Kanzi usually requires many trials to
learn a new sign, whereas human babies can speak words after only one exposure. Kanzi’s
language is focused primarily on food and pleasure and only rarely on social relationships.
Although he can combine words, he generates few new phrases and cannot master syntactic
rules beyond the level of about a 2-year-old human
child. [7]
learn by doing
Watch the video about Kanzi, then answer the questions.
In sum, although many animals communicate, none of them have a true language. With some
exceptions, the information that can be communicated in nonhuman species is limited
primarily to displays of liking or disliking and related to basic motivations of aggression
and mating. Humans also use this more primitive type of communication, in the form of
nonverbal behaviors such as eye contact, touch, hand signs, and interpersonal distance, to
communicate their like or dislike for others, but they (unlike animals) supplant this more
primitive communication with language. Although other animal brains share similarities to
ours, only the human brain is complex enough to create language. What is perhaps most
remarkable is that although language never appears in nonhumans, language is universal in
humans. All humans, unless they have a profound brain abnormality or are completely
isolated from other humans, learn language.
References
- de Waal, F.
(1989).
Peacemaking among Primates. Harvard University Press. Cambridge, MA.
- Von Frisch, K.
(1956).
Bees: Their Vision, Chemical Senses, and Language. Cornell University Press. Ithaca, NY.
- Seyfarth, R. M., and Cheney, D. L.
(1997).
"Behavioral mechanisms underlying vocal communication in nonhuman
primates." Animal Learning and Behavior. Volume 25. Number 3. 249–267
Pages.
- Hayes, K. J., and Hayes, C.
(1952).
"Imitation in a home-raised chimpanzee." Journal of Comparative and
Physiological Psychology. Volume 45. Number 5. 450–459 Pages.
- Fouts, R.
(1997).
Next of Kin: What Chimpanzees Have Taught Me about Who We Are. William Morrow. New York.
- Savage-Rumbaugh, S., and Lewin, R.
(1994).
Kanzi: The Ape at the Brink of the Human Mind. Wiley. Hoboken, NJ.
- Greenfield, P. M., and Savage-Rumbaugh, E. S.
(1991).
Biological and Behavioral Determinants of Language Development.
Chapter Imitation, grammatical development, and the invention of
protogrammar by an ape. Lawrence Erlbaum. Hillsdale, NJ. 235–258 Pages.
N. A. Krasnegor, D. M. Rumbaugh, R. L. Schiefelbusch, and M.
Studdert-Kennedy (Eds.).
Psychologists have long debated how to best conceptualize and measure
intelligence. These questions include how many types of intelligence there are,
the role of nature versus nurture in intelligence, how intelligence is
represented in the brain, and the meaning of group differences in
intelligence.
Psychologists have studied human intelligence since the 1880s. As you will
read, there are several theories of intelligence and a variety of tests to
measure intelligence. In fact, some define intelligence as whatever an
intelligence test measures. And most intelligence tests measure how much
knowledge one has, or in other words, “school smarts”. Today, most
psychologists define intelligence as a mental ability consisting of the ability
to learn from experience, solve problems, and use knowledge to adapt to new
situations.
In the early 1900s, the French psychologist Alfred Binet (1857–1914) and his colleague
Henri Simon (1872–1961) began working in Paris to develop a measure that would
differentiate students who were expected to be better learners from students who were
expected to be slower learners. The goal was to help teachers better educate these two
groups of students. Binet and Simon developed what most psychologists today regard as the
first intelligence test, which consisted of a wide variety of questions that included the
ability to name objects, define words, draw pictures, complete sentences, compare items,
and construct sentences.
Binet and Simon believed that the questions they asked their students, even
though they were on the surface dissimilar, all assessed the basic abilities to
understand, reason, and make judgments. And it turned out that the correlations
among these different types of measures were in fact all positive; students who
got one item correct were more likely to also get other items correct, even
though the questions themselves were very different.
On the basis of these results, the psychologist Charles Spearman (1863–1945)
hypothesized that there must be a single underlying
construct that all of these items measure. He called the construct that the
different abilities and skills measured on intelligence tests have in common
the general intelligence factor (g). Virtually all psychologists now believe
that there is a generalized intelligence factor, g, that relates to abstract
thinking and that includes the abilities to acquire knowledge, to reason
abstractly, to adapt to novel situations, and to benefit from instruction and
experience. People with higher general intelligence learn faster.
learn by doing
Generalized intelligence factor, referred to as g,
is assessed by having a person complete a variety of tasks. Some of the
tasks that psychologists will have the person do are intended to measure
key skill sets often needed to be successful in traditional school
settings. They include the following:
- verbal comprehension: measures a person’s ability to recognize and
use vocabulary, concepts, words
- abstract reasoning: the process of perceiving issues and reaching
conclusions through the use of symbols or generalizations rather than
concrete factual information
- perceptual speed: how fast one sees similarities/differences between
objects and/or symbols
- information: the level of knowledge that a
person has about commonly known facts
Using what you have learned about g, determine what
skill is being assessed in each of the following tasks.
Soon after Binet and Simon introduced their test, the American psychologist
Lewis Terman (1877–1956) developed an American version of Binet’s test
that became known as the Stanford-Binet Intelligence Test. The Stanford-Binet
is a measure of general intelligence made up of a wide
variety of tasks including vocabulary, memory for pictures, naming of familiar
objects, repeating sentences, and following commands.
Although there is general agreement among psychologists that g exists, there is
also evidence for specific intelligence (s), a measure of specific skills in
narrow domains. One empirical result in support of the idea of s comes from
intelligence tests themselves. Although the different types of questions do
correlate with each other, some items correlate more highly with each other
than do other items; they form clusters or clumps of intelligences.
One distinction is between fluid intelligence, which refers to the capacity to learn new
ways of solving problems and performing activities, and crystallized intelligence, which
refers to the accumulated knowledge of the world we have acquired throughout our lives.
These intelligences must be different because crystallized
intelligence increases with age—older adults are as good as or better than young
people in solving crossword puzzles—whereas fluid intelligence tends
to decrease with
age.
Other researchers have proposed even more types of intelligences. L. L. Thurstone [1] proposed that there were seven clusters of
primary mental abilities: word fluency, verbal comprehension, spatial ability, perceptual
speed, numerical ability, inductive reasoning, and memory. But even these dimensions tend
to be at least somewhat correlated, showing again the importance of g.
References
- Thurstone, L. L.
(1938).
Primary Mental Abilities. University of Chicago Press. Chicago. Psychometric Monographs, No. 1.
The goal of most intelligence tests is to measure g, the general
intelligence factor. Good intelligence tests are reliable, meaning that they are
consistent over time, and also demonstrate construct validity, meaning that they actually
measure intelligence rather than something else. Because intelligence
is such an important individual difference dimension, psychologists have invested
substantial effort in creating and improving measures of intelligence, and these tests are
now the most accurate of all psychological tests. In fact, the ability to accurately assess
intelligence is one of the most important contributions of psychology to everyday public
life.
Intelligence changes with age. A 3-year-old who could accurately multiply 183 by 39 would
certainly be intelligent, but a 25-year-old who could not do so might be seen as
unintelligent. Thus, understanding intelligence requires that we know the norms or
standards in a given population of people at a given age. The standardization of a test
involves giving it to a large number of people at different ages and computing the average
score on the test at each age level.
It is important that intelligence tests be standardized periodically to determine that the
average scores on the test at each age level remain the same; in other words, that the
median score of 100 remains the same for each age level on the test over time. James Flynn,
a New Zealand researcher, discovered that the mean IQ score of 100 between the years 1918
and 1995 had actually risen by about 25 points. [1] This is called
the Flynn effect, referring to the observation that scores on intelligence tests worldwide
have increased substantially over the past decades. Although the increase varies somewhat
from country to country, the average increase is about 3 IQ points every 10 years. It is
uncertain what causes this increase in intelligence on IQ tests. But some of the
explanations for the Flynn effect include better nutrition, increased
access to information, and more familiarity with multiple-choice tests. Whether people are
actually getting smarter is debatable.
learn by doing
Each year from 1945 through 1985, all children in the fifth grade in the United
States were given the California Scholastic Achievement Test, which was developed in
1944 and had not undergone any revisions or standardization. Later, a New Zealand
researcher analyzed the patterns of these scores. Study the three line graphs on the
chart below and complete the following questions.
Once the standardization has been accomplished, we have a picture of
the average abilities of people at different ages and can calculate a person’s mental age,
which is the age at which a person is performing intellectually. If we compare the mental
age of a person to the person’s chronological age, the result is the intelligence quotient
(IQ), a measure of intelligence that is adjusted for age. A simple way to calculate IQ is
by using the following formula:
IQ = mental age ÷ chronological age × 100
A 10-year-old child who does as well as the average 10-year-old child has an IQ of 100 (10
÷ 10 × 100), whereas an 8-year-old child who does as well as the average 10-year-old child
would have an IQ of 125 (10 ÷ 8 × 100). Most modern intelligence tests are based on the
relative position of a person’s score among people of the same age, rather than on the
basis of this formula, but the idea of an intelligence “ratio” or “quotient” provides a
good description of the score’s meaning.
learn by doing
Using the intelligence quotient formula, compute the required information for each of
the persons described in the below scenarios.
A number of scales are based on the IQ. The Wechsler Adult lntelligence Scale (WAIS) is the
most widely used intelligence test for adults. The current version of the WAIS, called the
WAIS-IV, was standardized on 2,200 people ranging from 16 to 90 years of age. It consists
of 15 different tasks, each designed to assess intelligence, including working memory,
arithmetic ability, spatial ability, and general knowledge about the world (see the figure
below). The WAIS-IV yields scores on four domains: verbal,
perceptual, working memory, and processing speed. The reliability of
the test is high (more than 0.95), meaning that when a person is assessed at different
times on the test, the person will score approximately the same every time with more than a
95% accuracy rate.
The WAIS-IV also shows substantial validity; it is correlated highly
with other IQ tests such as the Stanford-Binet, as well as with
criteria of academic and life success, including college grades, measures of work
performance, and occupational level. It also shows significant correlations with measures
of everyday functioning among the mentally retarded.
The Wechsler scale has also been adapted for preschool children in the form of the Wechsler Primary and Preschool Scale of Intelligence (WPPSI-III) and
for older children and adolescents in the form of the Wechsler
Intelligence Scale for Children (WISC-IV).
learn by doing
Let's now look at the concepts of reliability and validity. These are concepts that
are easily confused with one another and, in fact, they are related. A valid test
must be reliable, but the fact that a test is reliable does not mean it is valid. So
what is the difference?
Validity refers to the degree to which a
test or other measure of some psychological construct actually measures that
construct. A valid measure of your self-confidence is a questionnaire or
other measure that accurately indicates or predicts your true level of
self-confidence. There are a couple of things to notice about this definition.
First, it says “the degree to which…”—that means that validity is not an all-or-none
idea. Some tests are more valid than other tests. You will seldom see a test in
general use that is absolutely invalid, because such a test will be noticed and
discarded by people who want to study the construct being measured (e.g.,
self-confidence).
Second, validity is a very difficult characteristic to prove, particularly when you
are trying to measure something as complex as self-esteem or level of depression. For
this reason, any test in widespread use in psychology has many studies that attempt
to determine how valid it is in measuring what it is trying to measure and
enumerating its limitations.
Reliability refers to the degree to which a
test keeps producing the same or similar results over repeated testing. In
other words, reliability is another term for consistency.
There are a couple of things to notice here, as well.
First, reliability, like validity, is not all-or-none. Some tests are more reliable
than other tests.
Second, reliability is easier to establish than validity, because we can easily
conduct research that allows us to see if a test gives the same answer on repeated
testing.
A nice metaphor for thinking about validity and reliability comes from target
shooting. Imagine that you go to a target range and shoot at a target for a bull’s
eye. Here is what you hope you will see when you are done:

But let’s imagine that the target below is the one you produce:

What’s wrong? The hits are all clustered together, so you are very consistent. The
trouble is that you are missing the place you are aiming for.
For your review, here are four drawings of targets that illustrate the various levels
of validity and reliability.

Now let’s apply the concepts of validity and reliability to a psychological test
designed to measure self-confidence. A person’s true
self-confidence is the “center of the target.” The self-confidence test requires
people to answer five questions, such as the ones below. The person reads each
statement and then rates himself or herself on a scale of 1 to 5, with 1 representing
strong disagreement with the statement and 5 representing strong agreement with the
statement.
This is not a real self-confidence test but just an example. As you can see, the test
will result in a minimum score of 5 and a maximum score of 25. A person’s score can
then be compared to his or her actual or true self-confidence
level to determine how closely the test predicts the respondent’s actual
self-confidence. The closer the result is to the true self-confidence level, the
higher the validity.
To help you with this activity, each person’s true level of
self-confidence is provided in the chart below in the column labeled TRUTH.
Obviously, in real life, we don’t associate a person’s actual self-confidence level
with a score—that’s why we are using this self-questionnaire.
Imagine that you gave the self-confidence test to 10 people, and then you retested
them a week later. The chart below lists each person’s test scores for Week 1 and
Week 2. The two scores are compared to determine whether they are consistent with
each other. The more consistent the test scores, the higher the test
reliability.
Now you want to determine the validity and reliability of the self-confidence
test.
Here is another example with different scores for each person for weeks 1 and 2:
Following is another example that presents more difficulty in determining the level
of validity and reliability. Let’s see if you can get this one correct.
References
- Flynn, J. R.
(1999).
"Searching for justice: The discovery of IQ gains over time." American Psychologist. Volume 54. Number 1. 5–20 Pages.
Depending on the design, intelligence tests measure achievement (what one has
already learned) and aptitude (an ability to learn). Most licensed
psychologists, who want to determine one’s mental abilities with regard to any
mental disorders, will assess an individuals IQ that measures both achievement and aptitude. A
psychologist will use tests such as the Standford Binet or one of the Wechsler
scales.
More familiar intelligence tests are aptitude tests that
are designed to measure one’s ability to do well in college or in postgraduate
training. Most U.S. colleges and universities require students to take an
aptitude test such as the Scholastic Assessment Test (SAT) or the American
College Test (ACT), and postgraduate schools require the Graduate Record
Examination (GRE), Medical College Admissions Test (MCAT), or the Law School
Admission Test (LSAT). These tests are useful as one criteria for selecting
students because they predict academic success in the programs that they are
designed for, particularly in the first year of the program. These aptitude
tests also measure, in part, intelligence. Frey and Detterman [1]
found that the SAT correlated highly (between about r = .7 and r = .8) with
standard measures of intelligence, particularly on the WAIS.
Aptitude tests are also used by industrial and organizational (I/O)
psychologists in the process of personnel selection. Personnel selection is the
use of structured tests to select people who are likely to perform well at
given jobs. To develop a personnel selection test,
industrial and organizational (I/O) psychologists begin by conducting a job
analysis in which they determine what knowledge, skills, abilities, and
personal characteristics (KSAPs) are required for a given job. This is normally
accomplished by surveying and/or interviewing current workers and their
supervisors. Based on the results of the job analysis, I/O psychologists choose
selection methods that are most likely to be predictive of job performance.
Measures include tests of cognitive and physical ability and job knowledge
tests, as well as measures of intelligence and personality.
learn by doing
For students of psychology, it is important to know about some of the famous
researchers and psychologists who made valuable contributions to the field of
intelligence.
References
- Frey, M. C., and Detterman, D. K.
(2004).
"Scholastic assessment or g? The relationship between the
scholastic assessment test and general cognitive ability." Psychological
Science. Volume 15. Number 6. 373–378 Pages.
Before discussing different views of intelligence and controversies related to interpreting
intelligence, let’s look at the typical results that researchers get when they measure
intelligence using the Wechsler Adult Intelligence Scale (WAIS), which you studied in the previous module.
The WAIS was most recently updated in 2008. A sample of 2,200 adults varying in age (16 to
90 years old), sex, race, ethnicity, and other factors was tested. Although the test has
many questions, the scores are standardized so that the average performance is scored as
100. People who did better than average have scores above 100, and people who did worse
than average have scores below 100.
When we list all the scores of people taking tests like the WAIS, including other
intelligence tests as well as tests of aptitudes and various skills and traits, those
scores frequently fall into a pattern called the normal distribution,
or the bell curve. It looks like this:
Although this section is a little technical, understanding normal distribution is useful
for interpreting results not only of psychological studies but also of studies in many
other fields. We focus on an IQ test—the WAIS—but what you will learn can be applied any
time you see a bell curve.
In the following activities, you will learn the results of the study
when the IQ scores from the 2,200 adults were analyzed.
learn by doing
The recent study tested 2,200 people, but for our purposes, let’s reduce the number
to 16 people, and later we will discuss the results for all 2,200 people. Imagine
that the 16 people pictured below participated in the IQ study. Each photo is labeled
with the individual's IQ score.
Let’s see what happens when we organize them according to their IQ scores. Your task
is to drag each person to an appropriate box below. You have only 16 people, so a lot
of the boxes will be empty.
Start with the people with average IQ. Drag the pictures of the people with exactly
average IQ (remember, average = 100 in IQ scores) into the purple boxes, starting
with the bottom box.
Notice what happens as you get further to the right. What you see here with our
little sample of 16 people is very much like what would happen if you had all 2,200
scores.
Now let’s eliminate the empty boxes.
What we have here is called a frequency distribution. It shows
how frequently each score (in this case, each IQ score) appears in our group. Let’s
see if you can read it accurately.
The group of people, or distribution, below looks like a triangle.
However, if all 2,200 people and all the possible IQ scores were represented, the
shape would look like this:
The black line that goes above and around our 16 people has a distinctive shape,
which gives the graph its name: bell curve.
It is also called the normal distribution. It shows how many people have each score
on the IQ scale or the scale for any other test or measure (e.g., height, weight,
achievement test score, and many others).
Let’s look at the bell curve without our little people inside.
Now imagine 2,200 people squeezed beneath our bell curve. Notice that the numbers are
now gone from the Y axis on the left, so you can only talk in terms of more or fewer
people with any particular score.
When working with the bell curve, researchers often want to identify locations or regions.
For instance, they might want to talk about the top 10% of IQ scores or the middle 50%. To
do this, they break the curve into units, and for IQ those units are 15 points wide. This
15-point step is called a standard deviation.
For example, here is our bell curve, but notice that we have colored in a region that goes
from the mean (IQ = 100) to 15 points above the mean (100 + 15 = 115). Because this segment
covers exactly 15 points, it is one standard deviation wide.
To keep track of these units, we start counting from the mean (100) and count the standard
deviation steps from the mean in each direction. Here is another picture of the bell curve
with the standard deviation steps marked above the IQ scores.
And here is the area from the mean (100) to one standard deviation, or 15 points below the
mean (100 − 15 = 85).
As you can see, the further you get away from the mean, the smaller the area under the
curve in the 15-point units.
Here is the area between one and two standard deviations below the mean.
And now we go between two and three standard deviations below the mean.
We can keep going, but now you see there aren’t many people left as we get to the area
between three and four standard deviations below the mean.
Let’s look more closely at this. Here is the bell curve with the region covering the first
standard deviation above the mean colored in blue. Notice the numbers above this region. It
shows that this is 34% of the total area under the curve (just a little more than one-third
of the total). To put that in perspective, the number below it shows how many people out of
that original group of 2,200 used to standardize the IQ test are in this area: 748 out of
2,200.
If we go the same distance on the other side of the mean, we now show two colored regions:
one above the mean (100 to 115) and one below the mean (100 down to 85).
Just above each segment, you can see the percentage of the area under the curve and the
number of people in that unit. On top, in red, you can see the sum of these colored-in
areas. This figure says that 748 people out of 2,200 had IQ scores between 100 and 115 and
another 748 had IQ scores between 100 and 85, so a total of 1,496 had IQ scores between 85
and 115. That is just a little more than two-thirds of the total set of 2,200. Of course,
we’re not really interested in those 2,200 people. They simply represent the larger
population of adults.
did I get this
Here is a figure you can manipulate. Simply click on any of the areas under the
curve, and it will change colors (blue above the mean and green below the mean). The
area under the curve and the number of people in the sample of 2,200, as well as the
totals for all the colored areas, will be shown.
In the previous section, we explored the normal distribution in relation to the IQ scores
of samples of particular people. However, IQ scores in the general population are also
normally distributed. The figure below displays the distribution of IQ scores in the
general population.
One end of the distribution of intelligence scores is defined by people with very low IQ.
Mental retardation is a generalized disorder ascribed to people who have an IQ below 70,
who have experienced deficits since childhood, and who have trouble with basic life skills,
such as self-care and communicating with
others. [1] About 1% of the U.S. population, most
of them males, fulfill the criteria for mental retardation, but some children who are
diagnosed as mentally retarded lose the classification as they get older and better learn
to function in society. A particular vulnerability of people with low IQ is that they may
be taken advantage of by others, and this is an important aspect of the definition of
mental retardation. [2] Mental retardation
is divided into four categories: mild, moderate, severe, and profound. Severe and profound
mental retardation is usually caused by genetic mutations or accidents during birth,
whereas mild forms have both genetic and environmental influences.
One cause of mental retardation is Down syndrome, a chromosomal disorder
leading to mental retardation caused by the presence of all or part of an extra
21st chromosome. The incidence of Down syndrome is estimated at 1 per 800 to
1,000 births, although its prevalence rises sharply in those born to older
mothers. People with Down syndrome typically exhibit a distinctive pattern of
physical features, including a flat nose, upwardly slanted eyes, a protruding
tongue, and a short neck.
Societal attitudes toward individuals with mental retardation have changed over the past
decades. We no longer use terms such as “moron,” “idiot,” or “imbecile” to describe these
people, although these were the official psychological terms used to describe degrees of
retardation in the past. Laws such as the Americans with Disabilities Act (ADA) have made
it illegal to discriminate on the basis of mental and physical disability, and there has
been a trend to bring the mentally retarded out of institutions and into our workplaces and
schools. In 2002 the U.S. Supreme Court ruled that the execution of people with mental
retardation is “cruel and unusual punishment,” thereby ending this
practice. [3]
Extremely High Intelligence
Having an extremely high IQ is clearly less of a problem than having an extremely low
IQ, but there may also be challenges to being particularly smart. It is often assumed
that schoolchildren who are labeled as “gifted” may have adjustment problems that
make it more difficult for them to create social relationships. To study gifted
children, Lewis Terman and his colleagues [4]
selected about 1,500 high school students who
scored in the top 1% on the Stanford-Binet and similar IQ tests (i.e., who had IQs of
about 135 or higher) and tracked them for more than seven decades (the children
became known as the “Termites” and are still being studied today). This study found,
first, that these students were not unhealthy or poorly adjusted but rather were
above average in physical health and were taller and heavier than individuals in the
general population. The students also had above average social relationships—for
instance, they were less likely to divorce than the average
person. [5]
Terman’s study also found that many of these students went on to achieve high levels
of education and entered prestigious professions, including medicine, law, and
science. Of the sample, 7% earned doctoral degrees, 4% earned medical degrees, and 6%
earned law degrees. These numbers are all considerably higher than what would have
been expected from a more general population. Another study of young adolescents who
had even higher IQs found that these students ended up attending graduate school at a
rate more than 50 times higher than that in the general
population. [6]
As you might expect based on our discussion of intelligence, kids who are gifted have
higher scores on general intelligence (g). But there are also different types of
giftedness. Some children are particularly good at math or science, some at
automobile repair or carpentry, some at music or art, some at sports or leadership,
and so on. There is a lively debate among scholars about whether it is appropriate or
beneficial to label some children as gifted and talented in school and to provide
them with accelerated special classes and other programs that are not available to
everyone. Although doing so may help the gifted kids, [7]
it also may isolate them
from their peers and make such provisions unavailable to those who are not classified
as gifted.
did I get this
Here is a figure you can manipulate. Simply click on any of the areas under the
curve, and it will change colors (blue above the mean and green below the mean). The
area under the curve and the number of people in the sample of 2,200, as well as the
totals for all the colored areas, will be shown.
References
- Switzky, H. N., and Greenspan, S.
(2006).
What Is Mental Retardation? Ideas for an Evolving Disability in the 21st Century. American Association on Mental Retardation. Washington, DC.
- Greenspan, S., Loughlin, G., and Black, R. S.
(2001).
International Review of Research in Mental Retardation, Vol. 24.
Chapter Credulity and gullibility in people with developmental
disorders: A framework for future research. Academic Press. San Diego.
101–135 Pages. L. M. Glidden (Ed.).
-
(2002).
Atkins v. Virginia, 536 U.S. 304.
- Terman, L. M., and Oden, M. H.
(1959).
Genetic Studies of Genius: The Gifted Group at Mid-Life, Vol. 5. Stanford University Press. Stanford, CA.
- Seagoe, M. V.
(1975).
Terman and the Gidted. William Kaufmann. Los Altos, CA.
- Lubinski, D., and Benbow, C. P.
(2006).
"Study of mathematically precocious youth after 35 years:
Uncovering antecedents for the development of math-science expertise."
Perspectives on Psychological Science. Volume 1. Number 4. 316–345
Pages.
- Colangelo, N., and Assouline, S.
(2009).
The Routledge International Companion to Gifted Education.
Chapter Credulity and gullibility in people with developmental
disorders: A framework for future research. Routledge. New York. 194–202
Pages. T. Balchin, B. Hymer, and D. J. Matthews (Eds.).
One advocate of the idea of multiple intelligences is the psychologist Robert
Sternberg. Sternberg has proposed a triarchic (three-part)
theory of intelligence that proposes that people may display more or
less analytical intelligence, creative intelligence, and practical
intelligence. Sternberg [1] [2] argued that traditional
intelligence tests assess analytical intelligence, the ability to answer
problems with a single right answer, but that they do not well assess
creativity (the ability to adapt to new situations and create new ideas) or
practicality (e.g., the ability to write good memos or to effectively delegate
responsibility).
As Sternberg proposed, research has found that creativity is not highly correlated with
analytical intelligence, [3] and exceptionally
creative scientists, artists, mathematicians, and engineers do not score higher on
intelligence than do their less creative peers. [4]
Furthermore, the brain areas associated with convergent thinking, thinking that is directed toward finding the correct answer to a given
problem, are different from those associated with divergent
thinking, the ability to generate many different ideas for or
solutions to a single
problem. [5] On the other
hand, being creative often takes some of the basic abilities measured by g, including the
abilities to learn from experience, to remember information, and to think
abstractly. [6]
Studies of creative people suggest at least five components that are likely to
be important for creativity:
-
Expertise: Creative people have carefully studied and know a lot about the topic they
are working in. Creativity comes with a lot of hard
work. [7] [8]
-
Imaginative thinking: Creative people often view a problem in a visual way,
allowing them to see it from a new and different point of view.
-
Risk taking: Creative people are willing to take on new but potentially
risky approaches.
-
Intrinsic interest: Creative people tend to work on projects because they love doing
them, not because they are paid for them. In fact, research has found that people who
are paid to be creative are often less creative than those who are not
paid. [9]
-
Working in a creative environment: Creativity is in part a social
phenomenon. Simonton [10] found that the most creative people
were supported, aided, and challenged by other people working on similar
projects.
The last aspect of the triarchic model, practical intelligence,
refers primarily to intelligence that cannot be gained from books or
formal learning. Practical intelligence represents a type of “street smarts,” or
common sense, that is learned from life experiences. Although a number of tests have been
devised to measure practical
intelligence, [11] [12]
research has not found much evidence that practical intelligence is distinct from g or that
it is predictive of success at any particular tasks. [13]
Practical intelligence may include, at least in part, certain abilities that help people
perform well at specific jobs, and these abilities may not always be highly correlated with
general intelligence. [11] On the
other hand, these abilities or skills are very specific to particular occupations and do
not seem to represent the broader idea of intelligence.
Another champion of the idea of multiple intelligences is the psychologist Howard
Gardner. [14] [15] Gardner argued that it would be evolutionarily
functional for different people to have different talents and skills and proposed that
there are eight intelligences that can be differentiated from each other (shown in the
table below). Gardner noted that some evidence for multiple intelligences comes from the
abilities of autistic savants, people who score low on intelligence tests overall but who
nevertheless may have exceptional skills in a given domain, such as math, music, art, or in
being able to recite statistics in a given
sport. [16]
| Howard Gardner’s Eight Specific Intelligences |
|---|
| From Flat World Knowledge, Introduction to Psychology, v1.0, CC-BY-NC-SA. |
| Intelligence |
Description |
| Linguistic |
The ability to speak and write well |
| Logico-mathematical |
The ability to use logic and mathematical skills to solve problems |
| Spatial |
The ability to think and reason about objects in three dimensions |
| Musical |
The ability to perform and enjoy music |
| Kinesthetic (body) |
The ability to move the body in sports, dance, or other physical
activities |
| Interpersonal |
The ability to understand and interact effectively with others |
| Intrapersonal |
The ability to have insight into the self |
| Naturalistic |
The ability to recognize, identify, and understand animals, plants, and
other living things |
|
The idea of multiple intelligences has been influential in the field of education, and
teachers have used these ideas to try to teach differently to different students. For
instance, to teach math problems to students who have particularly good kinesthetic
intelligence, a teacher might encourage the students to move their bodies or hands
according to the numbers. On the other hand, some have argued that these “intelligences”
sometimes seem more like “abilities” or “talents” rather than real intelligence. And there
is no clear conclusion about how many intelligences there are. Are sense of humor, artistic
skills, dramatic skills, and so forth also separate intelligences? Furthermore, and again
demonstrating the underlying power of a single intelligence, the many different
intelligences are in fact correlated and thus represent, in part,
g. [17]
Psychology in Everyday Life: Emotional Intelligence
Although most psychologists have considered intelligence a cognitive ability, people also
use their emotions to help them solve problems and relate effectively to others. Emotional
intelligence is the ability to accurately identify, assess, and understand emotions, as
well as to effectively control one’s own
emotions. [18] [19]
The idea of emotional intelligence is seen in Howard Gardner’s interpersonal intelligence
(the capacity to understand the emotions, intentions, motivations, and desires of other
people) and intrapersonal intelligence (the capacity to understand oneself, including one’s
emotions). Public interest in and research on emotional intellgence became widely prevalent
following the publication of Daniel Goleman’s best-selling book, Emotional Intelligence: Why It Can Matter More Than
IQ. [20]
Mayer and Salovey [19] developed a four-branch model of emotional
intelligence that describes four fundamental capacities or skills. More specifically, this
model defines emotional intelligence as the ability to
- accurately perceive emotions in oneself and others (e.g., in the face or voice of
others);
- use emotions to facilitate thinking (i.e., to prioritize thinking or to allow
creativity to emerge);
- understand emotional meanings (i.e., understanding that specific emotions
convey their own pattern of possible messages and actions associated with
those messages); and
- manage emotions (i.e., regulate and manage one’s own and others’ emotions to promote
one’s own and others’ goals).
There are a variety of measures of emotional
intelligence. [21] [22]
One popular measure, the Mayer-Salovey-Caruso Emotional Intelligence
Test, includes items about the ability to understand,
experience, and manage emotions, such as these:
One problem with emotional intelligence tests is that they often do not show a great deal
of reliability or construct validity. [23]
Although it has been found that people with higher emotional intelligence are also
healthier, [24] findings are mixed about
whether emotional intelligence predicts life success—for instance, job
performance. [25] Furthermore, other researchers
have questioned the construct validity of the measures, arguing that emotional intelligence
really measures knowledge about what emotions are, not necessarily how to use those
emotions, [26] and that emotional intelligence is actually a
personality trait, a part of g, or a skill that can be applied in some specific work
situations—for instance, academic and work situations. [27]
Although measures of the ability to understand, experience, and manage emotions may not
predict effective behaviors, another important aspect of emotional intelligence—emotion
regulation—does. Emotion regulation is the ability
to control and productively use one’s emotions. Research has found that people who
are better able to override their impulses to seek immediate gratification and who are less
impulsive also have higher cognitive and social intelligence. They have better SAT scores,
are rated by their friends as more socially adept, and cope with frustration and stress
better than those with less skill at emotion
regulation. [28] [29] [30]
Because emotional intelligence seems so important, many school systems have designed
programs to teach it to their students. However, the effectiveness of these programs has
not been rigorously tested, and we do not yet know whether emotional intelligence can be
taught or if learning it would improve the quality of people’s
lives. [31]
learn by doing
The Mayer-Salovey-Caruso Emotional Intelligence Test includes questions about various
abilities: identifying emotions, facilitating thinking, understanding emotions, and
managing emotions.
Indicate which of the four branches of emotional intelligence is being assessed for
each of the following items. That is, is the question assessing the ability to (1)
identify emotions, (2) facilitate thinking, (3) understand emotions, or (4) manage
emotions?
References
- Sternberg, R. J.
(1985).
Beyond IQ: A Triarchic Theory of Human Intelligence. Cambridge University Press. New York.
- Sternberg, R. J.
(2003).
"Our research program validating the triarchic theory of successful
intelligence: Reply to Gottfredson." Intelligence. Volume 31. Number 4.
399–413 Pages.
- Furnham, A., and Bachtiar, V.
(2008).
"Personality and intelligence as predictors of creativity."
Personality and Individual Differences. Volume 45. Number 7. 613–617
Pages.
- Simonton, D. K.
(2000).
"Creativity: Cognitive, personal, developmental, and social
aspect." American Psychologist. Volume 55. Number 1. 151–158 Pages.
- Tarasova, I. V., Volf, N. V., and
Razoumnikova, O. M.
(2010).
"Parameters of cortical interactions in subjects with high and low
levels of verbal creativity." Human Physiology. Volume 36. Number 1.
80–85 Pages.
- Bink, M. L., and Marsh, R. L.
(2000).
"Cognitive regularities in creative activity." Review of General Psychology. Volume 4. Number 1. 59–78 Pages.
- Ericsson, K.
(1998).
"The scientific study of expert levels of performance: General
implications for optimal learning and creativity." High Ability Studies.
Volume 9. Number 1. 75–100 Pages.
- Weisberg, R.
(2006).
Creativity: Understanding Innovation in Problem Solving Science Invention and the Arts. Wiley. Hoboken, NJ.
- Hennessey, B. A., and Amabile, T. M.
(2010).
"Creativity." Annual Review of Psychology. Volume 61. Number 1. 569–598 Pages.
- Simonton, D. K.
(1992).
"The social context of career success and course for 2,026
scientists and inventors." Personality and Social Psychology Bulletin.
Volume 18. Number 4. 452–463 Pages.
- Sternberg, R. J., Wagner, R. K., and Okagaki, L.
(1993).
Mechanisms of Everyday Cognition. Chapter
Practical intelligence: The nature and role of tacit knowledge in work
and at school. Erlbaum. Hillsdale, NJ. 205–227 Pages. J. M. Puckett and
H. W. Reese (Eds.).
- Wagner, R., and Sternberg, R.
(1985).
"Practical intelligence in real-world pursuits: The role of tacit
knowledge." Journal of Personality and Social Psychology. Volume 49.
Number 2. 436–458 Pages.
- Gottfredson, L. S.
(2003).
"Dissecting practical intelligence theory: Its claims and evidence." Intelligence. Volume 31. Number 4. 343–397 Pages.
- Gardner, H.
(1983).
Frames of Mind: The Theory of Multiple Intelligences. Basic Books. New York.
- Gardner, H.
(1999).
Intelligence Reframed: Multiple Intelligences for the 21st Century. Basic Books. New York.
- Treffert, D. A., and Wallace, G. L.
(2004).
"Islands of genius." Scientific American. Volume 286. Number 6. 14–23 Pages.
- Brody, N.
(2003).
"Construct validation of the Sternberg triarchic abilities test:
Comment and reanalysis." Intelligence. Volume 31. Number 4. 319–329
Pages.
- Feldman-Barrett, L., and Salovey, P. (Eds.)
(2002).
The Wisdom in Feeling: Psychological Processes in Emotional Intelligence. Guilford Press. New York.
- Mayer, J. D., Salovey, P., and Caruso, D.
(2000).
Handbook of Intelligence. Chapter Models of emotional intelligence. Cambridge University Press. New York. 396–420 Pages. R. J. Sternberg (Ed.).
- Goleman, D.
(1998).
Working with in Emotional Intelligence. Bantam Books. New York.
- Mayer, J. D., Salovey, P., and Caruso, D. R.
(2008).
"Emotional intelligence: New ability or eclectic traits." American Psychologist. Volume 63. Number 6. 503–517 Pages.
- Petrides, K. V., and Furnham, A.
(2000).
"On the dimensional structure of emotional intelligence."
Personality and Individual Differences. Volume 29. Number 2. 313–320
Pages.
- Føllesdal, H., and Hagtvet, K. A.
(2009).
"Emotional intelligence: The MSCEIT from the perspective of
generalizability theory." Intelligence. Volume 37. Number 1. 94–105
Pages.
- Martins, A., Ramalho, N., and Morin, E.
(2010).
"A comprehensive meta-analysis of the relationship between
emotional intelligence and health." Personality and Individual
Differences. Volume 49. Number 6. 554–564 Pages.
- Harms, P. D., and Credé, M.
(2010).
"Emotional intelligence and transformational and transactional
leadership: A meta-analysis." Journal of Leadership and Organizational
Studies. Volume 17. Number 1. 5–17 Pages.
- Brody, N.
(2004).
"What cognitive intelligence is and what emotional intelligence is
not." Psychological Inquiry. Volume 15. Number 3. 234–238 Pages.
- Landy, F. J.
(2005).
"Some historical and scientific issues related to research on
emotional intelligence." Journal of Organizational Behavior. Volume 26.
Number 4. 411–424 Pages.
- Ayduk, O., Mendoza-Denton, R., Mischel, W.,
Downey, G., Peake, P. K., and Rodriguez, M.
(2000).
"Regulating the interpersonal self: Strategic self-regulation for
coping with rejection sensitivity." Journal of Personality and Social
Psychology. Volume 79. Number 5. 776–792 Pages.
- Eigsti, I.-M., Zayas, V., Mischel, W., Shoda,
Y., Ayduk, O., Dadlani, M. B., et al.
(2006).
"Predicting cognitive control from preschool to late adolescence
and young adulthood." Psychological Science. Volume 17. Number 6.
478–484 Pages.
- Mischel, W., and Ayduk, O. (Eds.)
(2004).
Willpower in a Cognitive-Affective Processing System: The Dynamics of Delay of Gratification. Guilford Press. New York.
- Mayer, J. D., and Cobb, C. D.
(2000).
"Educational policy on emotional intelligence: Does it make
sense?." Educational Psychology Review. Volume 12. Number 2. 163–183
Pages.
What do you think intelligence is? Is it something that you are born with,
largely inherited from your parents, leaving you with little room for
improvement? Or is it something that can be changed through hard work and by
taking advantage of opportunities to grow intellectually?
Your personal answer to this question turns out to be surprisingly important. It may even
affect your intelligence! Stanford University psychologist Carol Dweck has spent her career
studying how people’s beliefs about their own abilities—particularly mental abilities like
intelligence—influence the kinds of challenges they give themselves. In much of her
research, she has studied students, from their early prekindergarten days through
college.
Dweck identified two broad “theories of intelligence” that people—from young children to
mature adults—hold. Some people have an “entity” theory of intelligence. They believe that
their intelligence is determined by factors present at birth, particularly related to their
genetic inheritance. According to this theory, intelligence is a relatively unchangeable
fact about who you are and about your potential to excel. You may work hard, but
intelligence will always act as a limit for some people and as a supercharged fuel for
others. Other people hold an “incremental” theory of intelligence. They believe that
intelligence can be changed, particularly through efforts to learn and to excel. They
believe that genetic factors are only a starting point, and people’s future competencies
are not determined by their initial strengths and weaknesses.
These two theories of intelligence would only be vaguely interesting if they didn’t
influence people’s behavior. But they do. It turns out that students who hold the entity
theory of intelligence tend to avoid academic challenges. When given the opportunity to
work on a really challenging task—with opportunity for success but also a real possibility
of failure—they are less likely to take the opportunity than are their classmates who hold
an incremental theory of intelligence. The students who believe that intelligence is
unchangeable—the entity theory holders—are more likely to choose a task that they already
know will lead to success.
Attitudes toward failure can also be predicted by knowing which theory a
student has about intelligence. Students who have an entity theory of
intelligence tend to interpret failure—in academics and in other aspects of
life—as a message about their own inherent limitations, so failure or even the
anticipation of failure reduces their motivation to work on something. For
them, the way to protect their self-esteem is to avoid failure. For the
students who have an incremental theory of intelligence, failure is more often
seen as a challenge that can actually increase motivation. These students are
more likely than their entity theorist classmates to see failure as an
opportunity to discover and test their potential, thus inspiring them to try to
see what they can do.
Everything you have already read in this unit should have made it clear to you that
intelligence is a difficult quality to define and measure. Nevertheless, we do know that
IQ—the standard measure of intelligence—can change. For example, children who are unable to
attend school for a long periods due to war or extended illness show IQ levels 2 standard
deviations (30 IQ points) below their peers who are attending
school. [1] On the positive side, research has shown that
children, particularly children from low socioeconomic groups, can improve in IQ if they
are placed in an enriched prekindergarten program and then in an elementary school of
sufficient quality to maintain these gains. [2] Sadly, if children are
only placed in enriched preschools, but later attend academically poor elementary schools,
their IQ gains diminish or even disappear.
The Flynn Effect
Perhaps the most convincing discovery for understanding whether
intelligence can change or not comes from the work of James Flynn, who
analyzed IQ data from 14 nations spanning a period from the beginning of
the 20th century to the late 1980s. Later studies by Flynn and others
have added another 16 countries to the list, and these more recent
results are consistent with the initial findings. Flynn used
cross-sectional testing, meaning that different people were tested at
each point in time, rather than longitudinal testing, where the same
people would have been tracked across the time period of the study.
What Flynn found was that countries that were fully modern, with a thriving middle
class, effective school systems, and good employment opportunities, showed gains in
IQ that averaged about 3 points per decade. This may seem like a small amount, but
changes of this magnitude are actually astounding. Across a 50-year period, the
average IQ of people in these countries increased by approximately 15 IQ points,
which is a full standard deviation (see the Bell Curve module if you have forgotten
what a standard deviation is). These changes were not due to modifications of the
test; it reflects improvements in performance on IQ tests controlling for any changes
to the test itself. Further confirmation of this progressive improvement in IQ—a
change now called “the Flynn effect”—comes from data from countries that modernized
in the mid-20th century (e.g., Kenya and some Caribbean nations). The people in these
countries did not show substantial changes prior to modernization, but after people’s
socioeconomic status changed, the same IQ gains that characterized the countries that
modernized earlier—about 3 IQ points per decade—were recorded.
The reasons for these general changes in IQ are not completely
understood. It is likely that improvements to nutrition are important,
along with better schooling, more stimulating jobs, and even changes in
childbearing practices. For example, with fewer children per family, a
phenomenon common in more economically developed countries, parents can
devote more time to each child, leading to more opportunities for the
child to learn effectively from adults.
These changes may not go on forever. Some countries that were already
modernized in the late 19th century (e.g., Scandinavian countries) were
great examples of the Flynn effect when Flynn initially reported his
discovery in the 1980s, but have stopped showing IQ improvements in
recent years. Other countries, including the United States and Great
Britain, continue to show the 3 IQ points per decade improvement, but
there is no guarantee that this change will be sustained in future
decades. Nevertheless, the Flynn effect along with the effects of
enriched pre-kindergarten programs mentioned earlier clearly show that
intelligence—at least as measured by IQ tests—is something that can be
improved, both at the level of individuals and at the level of an entire
nation.
References
- Neisser, U., Boodoo, G., Bouchard, T. J., Jr., Boykin, A. W., Brody, N., Ceci, S. J., et al.
(1996).
"Intelligence: Knowns and unknowns." American Psychologist. Volume 51. Number 2. 77–101 Pages.
- Garber, H. L.
(1988).
The Milwaukee Project: Preventing Mental Retardation in Children at Risk. American Association on Mental Retardation. Washington, DC.
From the earliest days of IQ testing, people have wondered about group
differences in intelligence. You will probably not be surprised to learn that
studies of differences between groups in intelligence can easily feed
stereotypes and prejudices, and raise questions about testing biases and even
the integrity of the researchers.
You might think that the question of differences between men and women could
easily be resolved by analyzing IQ tests for thousands of people and simply
reporting the results. But it turns out that this won’t work. The most commonly
used IQ test, the WAIS, is regularly adjusted to eliminate questions that
produce differences between men and women. Consequently, the fact that there
are no gender differences on the WAIS is not interesting; the test is designed
to eliminate the possibility of differences. The goal of this adjustment is to
avoid including biased questions, but it means that we need to look elsewhere
to answer the question of IQ differences between men and women.
Using advanced statistical techniques, researchers have been able to extract the necessary
information from tests not specifically designed to measure IQ. For instance, Arthur
Jensen, whose view we will discuss further in the section on race and intelligence, studied
results from tests that are strongly related to IQ tests (“loaded heavily on g”) but have
not been adjusted to eliminate gender differences. Jensen [1] found minor
differences between men and women on tests of specific abilities, but he found no overall
differences between men and women in average intelligence. Using a different strategy,
James Flynn [2] looked at results from the Raven’s
Progressive Matrices test, a well-regarded nonverbal measure of intelligence, and found
that males and females were not different either in the childhood samples or adult samples.
The generally accepted view today is that the average IQs for men and women are the
same.
learn by doing
Note: For the following activities, the red
distributions correspond to females and the blue distributions correspond
to males.
This is not the end of questions about sex differences in intelligence,
however. In 2006, Lawrence Summers, president of Harvard University, was
discussing reasons that far more men than women go into advanced positions in
science and engineering. Citing published research, Summers suggested that
there may not be a difference between the average intelligence for men and
women, but men may be more variable in their intelligence.
Prof. Summers’ claim is not without some foundation. Mental retardation (i.e., IQ below 70)
is about 3.6 times more common for males than females. [3]
Note that the diagnosis of mental retardation is based on more than scores on a standard IQ
test, but this fact is consistent with the low end of the blue curve in the figure—more
males than females appear to occupy that lower region. Summers’ statement about the high
end of the distributions is based primarily on data showing more males than females among
the highest scorers on tests of mathematics and quantitative reasoning. For instance, in
the 1980s, twelve times more boys than girls scored above 700 (out of a possible 800) on
the SAT test. [4] These results are consistent with the
high extreme depicted in the figure: the blue curve for males is higher (more individuals)
on the right than the red curve for females.
learn by doing
Note: For this activity, the red
distributions correspond to females and the blue distributions correspond
to males.
Now we get to the controversial part of the IQ debate for gender. Professor Summers
of Harvard University suggested that women’s intelligence—particularly as related to
mathematical thinking—might be less likely to extend to the genius level than men’s
intelligence.
Why are there these differences between the spread of scores for males and for females in
intelligence-related measures? Most researchers think that the male and female
distributions would be about the same on the lower end of the distributions if males were
not more vulnerable to genetic and prenatal factors that can hurt development of brain
structures related to thinking. Some X-chromosome regions have been linked to mental
retardation, and only males have a Y chromosome. Furthermore, prenatal steroidal hormones
influence brain structures related to intelligence, and males fetuses are exposed to
massively higher levels of these steroids than are female fetuses. Estrogen, an important
female hormone, may be a protective factor for girls and women, reducing the impact of
biological factors that can influence intellectual functioning.
On the high extreme, genetic and other biological factors favoring males have
not been found. Instead, experience appears to be the critical factor. For
instance, differences between men and women on mathematics and other
quantitative skills are rapidly diminishing as girls and women take more
mathematics-related courses in school and are encouraged to excel in these
areas. The 12:1 ratio of males over females on the quantitative SAT scores
comes from data in the mid-20th century. Sex differences have dramatically
declined since that time. More recent studies show about a 3:1 ratio (3 times
more boys than girls) at the highest levels of SAT scores. It is impossible to
know if these trends will continue or not, but such a dramatic change in a few
decades strongly supports the hypothesis that most or all of the differences
between men and women at the high extreme of IQ-related tests can be explained
by educational and motivational differences between genders, and these
differences are quickly disappearing.
learn by doing
Note: For this activity, the red
distributions correspond to females and the blue distributions correspond
to males.
In the text, you learned that most psychologists (as well as scholars in other
fields) disagreed with Dr. Summers’s suggestion that there may be a genetic reason
for higher male performance on the highest extreme of quantitative measures related
to IQ. See the text to learn some of the reasons for rejecting the genetic
hypothesis. The idea that there may be differences between men and women on the lower
extreme of the IQ distribution is less controversial.
References
- Jensen, A. R.
(1998).
The g Factor: The Science of Mental Ability. Praeger. Westport, CT.
- Flynn, J. R., and Rossi-Casé, L.
(2011).
"Modern women match men on Raven’s Progressive Matrices."
Personality and Individual Differences. Volume 50. Number 6. 799–803
Pages.
- Flynn, J. R., and Rossi-Casé, L.
(1993).
"Sex differences in pervasive developmental disorders." Journal of
Autism and Developmental Disorders. Volume 23. Number 4. 579–591 Pages.
- Benbow, C. P., and Stanley, J. C.
(1983).
"Sex differences in mathematical reasoning ability: More facts." Science. Volume 222. Number 4627. 1029–1031 Pages.
Intelligence tests are adjusted to eliminate gender differences, but racial and ethnic
differences have been more resistant to test changes. Prior to the civil rights era of the
1960s, little attention was paid to choices of content and wording that might bias the
tests in favor of one racial or ethnic group over another. During the 1960s and 1970s, the
validity and fairness of IQ tests and other achievement and aptitude tests was hotly
debated. Among the positive results of that discussion was the development of now-standard
procedures for detecting and eliminating some types of unfair items and the increased
sensitivity of testers to potential biases in the content and scoring of tests.
Nevertheless, differences in culture and experience are so complex that no procedures or
statistical tests can successfully detect items or procedures that are unfair to some
individuals or groups. [1]
In the early 20th century, it was not unusual to attribute differences in average IQ scores
among various racial and ethnic groups to biological causes, an interpretation sometimes
called the hereditarian theory of
IQ. [2] The belief was that some groups had evolved
further than others, leading these so-called superior groups to function better
intellectually than others. For instance, at the beginning of the 20th century, immigrants
from Italy to America had a median tested IQ of 87, which is nearly a standard deviation
(15 points) below the average of 100. One the most respected figures in intelligence
testing at the time, Henry Goddard, concluded that approximately 80% of Italian immigrants
were “feeble-minded,” and he made similar claims about immigrants from Russia and the
Austro-Hungarian empire. Goddard and many others attributed this supposed intellectual
deficiency to hereditary factors. He recommended that all immigrants to the U.S. be tested
for intelligence, and those with low scores should be barred from entry. What we now know
is that the intelligence tests were given in English, not the immigrants’ native language
and furthermore, contained phrases that were culturally-specific. For example, in America,
you may often hear the phrase “to kill two birds with one stone.” You will likely
understand this to mean that you will be able to get two jobs done with one action.
However, for someone not accustomed to this phrase, it will mean very little. Today,
Italian Americans as a group score slightly above 100 on the average, and other immigrant
groups that, like those of Italian descent, have been able to integrate with the dominant
white culture show similar gains, supporting the well-known fact that early intelligence
tests had extreme cultural bias and consequently, the results were widely misconstrued.
The hereditarian theory has not completely disappeared. Most notably, in 1994, a book
called The Bell Curve by two well-known social scientists, Richard
Herrnstein and Charles Murray, forcefully argued that some IQ differences between races are
genetic and unlikely to disappear regardless of social and educational opportunities. [3] Not
surprisingly, the book immediately led to intense and often acrimonious debate. In response
to the debate, the American Psychological Association (APA) asked a group of highly
regarded scientists, headed by respected psychologist Ulric Neisser of Emory University, to
review the scientific literature that related to IQ differences among racial and ethnic
groups, as well as sex differences.
The APA Task Force [4] started by noting that “intelligence” is a
very complex quality and even experts disagree about its definition. Furthermore, all IQ
tests assess only a limited number and range of abilities, inevitably leaving many other
aspects of intelligence untested.
The APA Task Force report summarized racial and ethnic group average IQ scores from the
mid-1990s. Both Asian Americans and Caucasian Americans had averages around 100, the
standardized average for IQ scores. African Americans averaged around 90, having reduced
the 15 points (average IQ = 85) found in earlier decades by 5 points. Hispanic Americans
were found to score in the mid-90s on average.
After reviewing evidence related to IQ, the APA Task Force concluded that there
is no credible evidence for a genetic explanation for racial and ethnic
differences in IQ. This does not mean that our genes have no influence on IQ;
that link has been firmly established. However, this simply means that our
parents’ IQ is somewhat correlated with our own IQ, but this reasoning cannot
be extended to group differences. To understand how genetic factors can
influence the relationship between the IQ of parents and their children while
not explaining differences between racial groups, work through the following
activity.
learn by doing
People often confuse causes of individual differences (e.g., why you are
a better athlete than your best friend) with group differences (e.g., why
people from Africa currently dominate distance running). The mistake is
to believe that the cause of some difference at the individual level must
follow the same rules as the cause of a difference at the group level.
But let’s see if this is necessarily true.
Imagine that you have two varieties of a plant. The orange variety has
developed under excellent lighting conditions. Notice that some of them
are tall, some are medium sized, and some are short. This is just normal
variability that we find with almost any characteristic of a living thing
that you measure. A second variety of the plant, with blue flowers, can
be seen on the right. As with the orange variety, some are relatively
tall, some are relatively medium in height, and some are relatively
short.
Now we are going to see what happens when each of these plants has
offspring. What do the plants that grew from each of these look like.
Let’s also imagine that this strong relationship between relative heights
of parents and offspring is heavily influenced by genes. So the reason that tall plants have tall offspring is
because that tall parents pass on genes that maximize growth and the reason that short parents have short offspring is
because the short parents have genes that minimize growth.
Now it is time to do some transplanting. Imagine that you wonder if the
blue plants are getting enough sunlight. You plant some of the blue
variety in the same sunny conditions that the orange variety already
enjoys. Let’s see what happens.
How could this happen? Even though genes determine relative height (in
our cartoon flowers anyway), the genes don’t determine the absolute
height. Better or worse growing conditions can determine just how tall
the plant can possibly grow, but, within any given set of conditions,
genes will determine which are the tall, medium, and short plants.
This idea is not at all unrealistic. At the end of World War II, people
from the United States were the tallest people in the world. This did not
mean that everyone from the United States was
taller than everyone from any other country. There
were still tall, medium, and short U.S. citizens and tall, medium, and
short citizens of other countries, and tall parents still tended to have
tall children, short parents tended to have short children, and so on. At
that time, because the United States was such a dominant center for
agriculture, average nutrition in the United States was superior to
average nutrition in most other places, even though there were then, as
now, people going hungry even in the United States. Since that time,
nutrition has improved in many other countries and now citizens of the
U.S. are not, on average, among the top 10 in terms of height. The
tallest people in the world today are from the Netherlands. People from
the U.S. have not shrunk. People from these other countries have gotten
taller.
To make the point even more strongly, imagine that you planted both the
orange and blue varieties in some different soil and this is what
happened:
Notice that the orange plants are unaffected by the new soil, so they are the same as
before. But the blue variety loves the new soil and thrives
in it. Now the variety that used to be shorter on average—the blue variety—is taller
on average. But there is still the same genetic link: Tall plants have tall
offspring, medium plants have medium offspring, and short plants have short
offspring.
Now let’s apply this same idea to intelligence.
Imagine that there are two groups of people, represented by the orange
and blue borders below. The orange group lives in an intellectually
stimulating environment, while the blue group lives in a less varied and
intellectually challenging environment. This graphic represents the IQ
levels of members of the two groups.
 Photos used in this activity courtesy of Franklin
Park Library and umjanedoan
(CC-BY-2.0).
Photos used in this activity courtesy of Franklin
Park Library and umjanedoan
(CC-BY-2.0).
Now imagine that the blue group experiences an improvement of
circumstances, moving to a more stimulating and intellectually
challenging environment. Here is what happens:
Under intellectually enriched conditions, the blue group has now improved
its average IQ. But there is still a direct relationship between parent
and offspring IQ. It is possible for genes to determine the relationship
between parent and offspring IQ even if environmental factors determine
the average level of each group’s IQ. Of course, in the real world,
unlike our cartoon world, both genes and environmental factors influence
IQ, so the relationship between parent and offspring IQ is not so easily
predicted as it is in our cartoons.
Although the hereditarian hypothesis is a logically possible explanation of
differences between racial and ethnic groups, research doesn’t support it.
There is not empirical support for the idea that racial or ethnic groups differ
genetically in ways that relate to intelligence. The APA Task Force also
reviewed the research on biased tests and biased testing procedures and found
that these factors cannot explain the size of the group differences. Similarly,
they rejected differences in socioeconomic status as an adequate explanation.
In fact, although they unequivocally rejected the hereditarian explanation,
they concluded that “at this point, no one knows what causes this
differential,” where the “differential” is the group difference in IQ.
Even if we cannot clearly identify the reasons for racial and ethnic differences in IQ, we
do know that these differences can change, just as we suggested in the Learn by Doing
exercise. For example, Dickens and Flynn [5] looked at IQ scores from 1972 to
2002 and found a reduction in the difference between blacks and whites during this period
of more than 5 IQ points, one-third of the difference between the groups.
An adoption study by Moore [6] looked at black children adopted into black and
white families, where the children adopted by the white families could expect to receive
the benefits of greater affluence and the social and cultural support of the dominant
group. On later testing, children adopted into white families had IQs that were 13 points
higher than the children adopted into black families. This is almost the entire 15 point
difference reported between the two races at that time. These results and others suggest
that racial differences in IQ are largely or completely the result of differences in
experience. It is particularly interesting that black children measured at age 4 are only
about 5 IQ points below white children of the same age, while the group differences are
about 17 points by age 24, a finding that strongly suggests that the life experiences of
black and white children may produce these diverging outcomes.
There are many ways that experience can influence intelligence. Socioeconomic status (i.e.,
income and social opportunities) can affect the type of neighborhood a person can afford to
live in, the quality of schooling and likelihood of preschool educational opportunities,
and likelihood of taking advantage of educational activities (e.g., visiting museums and
historical sites). Differences in parental education levels can have a huge impact. For
instance, Hart and Risley [7] studied interactions between adults and children in
families differing in socioeconomic status and education. This was not a race difference
study. They found that children of professional-level parents heard three times as many
words and far more complex and unusual words than did children of unemployed parents, and
children of working-class parents heard twice as many words as the children of unemployed
parents. Although a word count like this may seem unimportant, exposure to language is very
important for development of communication skills and categories of knowledge.
It is impossible to know for certain at this point in time why racial groups
differ in measured IQ. However, it is clear that many social and environmental
factors can influence intellectual development and racial groups differ
substantially in typical social experiences. Furthermore, as genetics has
matured as a science, the old distinction between nature and nurture has been
lost. We now understand that environmental factors influence genetic expression
from the moment of conception to the end of life, so differences between groups
that differ in typical experiences are to be expected. Research is slowly
unraveling those influences.
References
- Cole, N. S., and Zieky, M. J.
(2001).
"The new faces of fairness." Journal of Educational Measurement. Volume 38. Number 4. 369–382 Pages.
- Gould, S. J.
(2008).
The Mismeasure of Man. W.W. Norton. New York.
- Herrnstein, R. J., and Murray, C. A. S.
(2010).
The Bell Curve: Intellingence and Class Structure in American Life. Free Press. New York.
- Neisser, U., Boodoo, G., Bouchard, T. J., Jr., Boykin, A. W., Brody, N., Ceci, S. J., et al.
(1996).
"Intelligence: Knowns and unknowns." American Psychologist. Volume 51. Number 2. 77–101 Pages.
- Dickens, W. T., and Flynn, J. R.
(2006).
"Black Americans reduce the racial IQ gap: Evidence from
standardization samples." Psychological Science. Volume 17. Number 10.
913–920 Pages.
- Moore, E. G. J.
(1986).
"Family socialization and the IQ test performance of traditionally
and transracially adopted black children." Developmental Psychology.
Volume 22. Number 3. 317–326 Pages.
- Hart, B., and Risley, R. T.
(1995).
Meaningful Differences in the Everyday Experience of Young American Children. Paul H. Brookes. Baltimore.
Although intelligence tests may not be culturally biased, the situation in
which one takes a test may be. One environmental factor that may affect how
individuals perform and achieve is their expectations about their ability at a
task. In some cases these beliefs may be positive, and they have the effect of
making us feel more confident and thus better able to perform tasks. For
instance, research has found that because Asian students are aware of the
cultural stereotype that “Asians are good at math,” reminding them of this fact
before they take a difficult math test can improve their performance on the
test. [1] On the other hand, sometimes these
beliefs are negative, and they create negative self-fulfilling prophecies such
that we perform more poorly just because of our knowledge about the
stereotypes.
In 1995 Claude Steele and Joshua Aronson tested the hypothesis that the
differences in performance on IQ tests between Blacks and Whites might be due
to the activation of negative
stereotypes. [2] Because Black students
are aware of the stereotype that Blacks are intellectually inferior to Whites,
this stereotype might create a negative expectation, which might interfere with
their performance on intellectual tests through fear of confirming that
stereotype.
In support of this hypothesis, the experiments revealed that Black college
students performed worse (in comparison to their prior test scores) on
standardized test questions when this task was described to them as being
diagnostic of their verbal ability (and thus when the stereotype was relevant),
but that their performance was not influenced when the same questions were
described as an exercise in problem solving. And in another study, the
researchers found that when Black students were asked to indicate their race
before they took a math test (again activating the stereotype), they performed
more poorly than they had on prior exams, whereas White students were not
affected by first indicating their race.
Steele and Aronson argued that thinking about negative stereotypes that are
relevant to a task that one is performing creates stereotype
threat—performance decrements that are caused by the
knowledge of cultural stereotypes. That is, they argued that the
negative impact of race on standardized tests may be caused, at least in part,
by the performance situation itself. Because the threat is “in the air,” Black
students may be negatively influenced by it.
Research has found that stereotype threat effects can help explain a wide
variety of performance decrements among those who are targeted by negative
stereotypes. For instance, when a math task is described as diagnostic of
intelligence, Latinos and Latinas perform more poorly than do
Whites. [3]
Similarly, when stereotypes are activated, children with low socioeconomic
status perform more poorly in math than do those with high socioeconomic
status, and psychology students perform more poorly than do natural science
students. [4] [5]
Even groups who typically enjoy advantaged social status can be made to
experience stereotype threat. White men perform more poorly on a math test when
they are told that their performance will be compared with that of Asian
men, [6]
and Whites perform more poorly than Blacks on a sport-related task when it is
described to them as measuring their natural athletic
ability. [7] [8]
Research has found that stereotype threat is caused by both cognitive and
emotional factors. [9] On the
cognitive side, individuals who are experiencing stereotype threat show an
increased vigilance toward the environment as well as increased attempts to
suppress stereotypic thoughts. Engaging in these behaviors takes cognitive
capacity away from the task. On the affective side, stereotype threat occurs
when there is a discrepancy between our positive concept of our own skills and
abilities and the negative stereotypes that suggest poor performance. These
discrepancies create stress and anxiety, and these emotions make it harder to
perform well on the task.
Stereotype threat is not, however, absolute; we can get past it if we try. What
is important is to reduce the self doubts that are activated when we consider
the negative stereotypes. Manipulations that affirm positive characteristics
about the self or one’s social group are successful at reducing stereotype
threat. [10] [11]
In fact, just knowing that stereotype threat exists and may influence our
performance can help alleviate its negative
impact. [12]
learn by doing
The following video clip discusses stereotype threat. Watch the video and
complete the table below.
The video described a study by Jeff Stone that measured the effects of
stereotype threat on Black and White athletes’ performance on a test of
athletic aptitude. The study consisted of two conditions. In one
condition, participants were told that the test measured natural athletic
ability, and in the other condition participants were told that the test
measured ability to think strategically.
References
- Walton, G. M., and Cohen, G. L.
(2003).
"Stereotype lift." Journal of Experimental Social Psychology. Volume 39. Number 5. 456–467 Pages.
- Steele, C. M., and Aronson, J.
(1995).
"Stereotype threat and the intellectual performance of African
Americans." Journal of Personality and Social Psychology. Volume 69.
Number 5. 797–811 Pages.
- Gonzales, P. M., Blanton, H., and Williams,
K. J.
(2002).
"The effects of stereotype threat and double-minority status on the
test performance of Latino women." Personality and Social Psychology
Bulletin. Volume 28. Number 5. 659–670 Pages.
- Brown, R., Croizet, J.-C., Bohner, G.,
Fournet, M., and Payne, A.
(2003).
"Automatic category activation and social behaviour: The moderating
role of prejudiced beliefs." Social Cognition. Volume 21. Number 3.
167–193 Pages.
- Croizet, J.-C., and Claire, T.
(1998).
"Extending the concept of stereotype and threat to social class:
The intellectual underperformance of students from low socioeconomic
backgrounds." Personality and Social Psychology Bulletin. Volume 24.
Number 6. 588–594 Pages.
- Aronson, J., Lustina, M. J., Good, C.,
Keough, K., and Steele, C. M.
(1999).
"When white men can’t do math: Necessary and sufficient factors in
stereotype threat." Journal of Experimental Social Psychology. Volume
35. Number 1. 29–46 Pages.
- Stone, J.
(2002).
"Battling doubt by avoiding practice: The effects of stereotype
threat on self-handicapping in white athletes." Personality and Social
Psychology Bulletin. Volume 28. Number 12. 1667–1678 Pages.
- Stone, J., Lynch, C. I., Sjomeling, M., and
Darley, J. M.
(1999).
"Stereotype threat effects on black and white athletic
performance." Journal of Personality and Social Psychology. Volume 77.
Number 6. 1213–1227 Pages.
- Schmader, T., Johns, M., and Forbes, C.
(2008).
"An integrated process model of stereotype threat effects on
performance." Psychological Review. Volume 115. Number 2. 336–356 Pages.
- Marx, D. M., and Roman, J. S.
(2002).
"Female role models: Protecting women’s math test performance."
Personality and Social Psychology Bulletin. Volume 28. Number 9.
1183–1193 Pages.
- McIntyre, R. B., Paulson, R. M., and Lord,
C. G.
(2003).
"Alleviating women’s mathematics stereotype threat through salience
of group achievements." Journal of Experimental Social Psychology.
Volume 39. Number 1. 83–90 Pages.
- Johns, M., Schmader, T., and Martens, A.
(2005).
"Knowing is half the battle: Teaching stereotype threat as a means
of improving women’s math performance." Psychological Science. Volume
16. Number 3. 175–179 Pages.
The Repository for Germinal Choice
During the 1970s, American millionaire Robert Klark Graham began one of the most
controversial and unique sperm banks in the world. He called it the Repository
for Germinal Choice. The sperm bank was part of a project that attempted to
combat the “genetic decay” Graham saw all around him. He believed human
reproduction was experiencing a genetic decline, making for a population of
“retrograde humans,” and he was convinced that the way to save the human race
was to breed the best genes of his generation. [1]
Graham began his project by collecting sperm samples from the most intelligent
and highly achieving people he could find, including scientists, entrepreneurs,
athletes, and even Nobel Prize winners. Then he advertised for potential
mothers, who were required to be married to infertile men, educated, and
financially well-off. Graham mailed out catalogs to the potential mothers,
describing the donors using code names such as “Mr. Grey-White,” who was
“ruggedly handsome, outgoing, and positive, a university professor, expert
marksman who enjoys the classics,” and “Mr. Fuchsia,” who was an “Olympic gold
medalist, tall, dark, handsome, bright, a successful businessman and
author.” [1] When the mother had made her choice, the sperm
sample was delivered by courier and insemination was carried out at home. Before
it closed following Graham’s death in 1999, the repository claimed
responsibility for the birth of 228 children.
But did Graham’s project actually create superintelligent babies? Although it is
difficult to be sure, because very few interviews with the offspring have been
permitted, at least some of the repository’s progeny are indeed smart. A reporter
for Slate magazine, David Plotz, [1] spoke to
nine families who benefited from the repository, and they proudly touted their
children’s achievements. He found that most of the offspring in the families
interviewed seem to resemble their genetic fathers. Three from donor Mr. Fuchsia,
the Olympic gold medalist, are reportedly gifted athletes. Several who excel in math
and science were fathered by professors of math and science.
And the offspring, by and large, seem to be doing well, often attending excellent
schools and maintaining very high grade-point averages. One of the offspring, now 26
years old, is particularly intelligent. In infancy, he could mark the beat of
classical music with his hands. In kindergarten, he could read Hamlet and was learning algebra, and at age 6, his IQ was already 180. But
he refused to apply to prestigious universities, such as Harvard or Yale, opting
instead to study at a smaller progressive college and to major in comparative
religion with the aim of becoming an elementary school teacher. He is now an author
of children’s books.
Although it is difficult to know for sure, it appears that at least some of the
children of the repository are indeed outstanding. But can the talents,
characteristics, and skills of this small repository sample be attributed to
genetics alone? After all, consider the parents of these children: Plotz
reported that the parents, particularly the mothers, were highly involved in
their children’s development and took their parental roles very seriously. Most
of the parents studied child care manuals, coached their children’s sports
teams, practiced reading with their kids, and either home-schooled them or sent
them to the best schools in their areas. And the families were financially
well-off. Furthermore, the mothers approached the repository at a relatively
older child-bearing age, when all other options were exhausted. These children
were desperately wanted and very well loved. It is undeniable that, in addition
to their genetic backgrounds, all this excellent nurturing played a significant
role in the development of the repository children.
Although the existence of the repository provides interesting insight into the
potential importance of genetics on child development, the results of Graham’s
experiment are inconclusive. The offspring interviewed are definitely smart and
talented, but only one of them was considered a true genius and child prodigy.
And nurture may have played as much a role as nature in their
outcomes. [2] [1]
Introduction
The goal of this unit is to investigate the fundamental, complex, and essential
process of human development. Developmental psychology
concerns the physiological, behavioral, cognitive, and social
changes that occur throughout human life, which are guided by both genetic
predispositions (nature) and environmental influences (nurture).
Developmental psychologists explore three questions throughout their careers:
- Does our development occur gradually over time or in strict stages?
- Do our childhood experiences have a stronger impact than later experiences
in life?
- What roles do genetics and the environment play in our development?
We begin our study of development at the moment of conception, when the father’s
sperm unites with the mother’s egg, and then consider prenatal development in
the womb. Next we focus on infancy, the developmental stage that begins at birth
and continues to one year of age, and childhood, the period between infancy and
the onset of puberty. We then consider the developmental changes that occur
during adolescence—the years between the onset of puberty and the beginning of
adulthood; the stages of adulthood itself, including emerging, early, middle,
and older adulthood; and finally, the preparations for and eventual facing of
death.
Each stage of development has its unique physical, cognitive, and emotional
changes that define the stage and distinguish it from the others. Many
developmental theorists discuss the changes that we, as humans, undergo
throughout our lifetime. One such theorist, Erik
Erikson [3] , proposed a model of lifespan development that
provides a useful guideline for thinking about the changes we experience. As you
can see in the following table, Erikson believed each life stage has a unique
challenge that the person who reaches it must face. How the person resolves the
challenge has an impact on his or her overall development. So, for example, the
young infant begins his life in the first stage, the trust versus mistrust
stage. During that time, the infant is dependent on others to meet his basic
needs, which includes feeding him; clothing him; hugging him when he is afraid,
excited, or simply needs to be reassured; and allowing him to interact with his
environment in a safe and healthy manner. If the infant receives what he needs,
he will leave this stage with feelings of trust for his caregivers. However, if
the infant is mistreated, neglected, or not given what he needs during this
stage, he may resolve this stage with feelings of distrust for the people who
were supposed to care for him.
| Erik Erikson’s Framework for Development |
|---|
| From Flat World Knowledge, Introduction to Psychology, v1.0. Adapted from Erikson, E. H. (1963). Childhood and Society. New York: Norton (p. 202). |
| Stage/Age Range |
Main Challenge |
Positive Resolution of the Challenge |
| Birth to 18 months |
Trust versus mistrust |
The child develops a feeling of trust in his or her caregivers. |
| 18 months to 3 years |
Autonomy versus shame/doubt |
The child learns what he or she can and cannot control and develops a
sense of free will. |
| 3 to 6 years |
Initiative versus guilt |
The child learns to be independent by exploring, manipulating, and
taking action. |
| 6 to 12 years |
Industry versus inferiority |
The child learns to do things well or correctly according to standards
set by others, particularly in school. |
| 12 to 18 years |
Identity versus role confusion |
The adolescent develops a well-defined and positive sense of self in
relationship to others. |
| 19 to 40 years |
Intimacy versus isolation |
The person develops the ability to give and receive love and to make
long-term commitments. |
| 40 to 65 years |
Generativity versus stagnation |
The person develops an interest in guiding the development of the next
generation, often by becoming a parent. |
| 65 to death |
Ego integrity versus despair |
The person develops acceptance of his or her life as it was lived. |
|
As we progress through this module, we will see that Robert Klark Graham was in
part right—nature does play a substantial role in development (it has been
found, for instance, that identical twins, who share all of their genetic code,
usually begin sitting up and walking on the exact same days). But nurture is
also important—we begin to be influenced by our environments even while still in
the womb, and these influences remain with us throughout our development.
Furthermore, we will see that we play an active role in shaping our own lives.
Our own behavior influences how and what we learn, how people respond to us, and
how we develop as individuals. As you read the unit, you will no doubt get a
broader view of how we each pass through our own lives. You will see how we
learn and adapt to life’s changes, and this new knowledge may help you better
understand and better guide your own personal life journey. By the end of this
unit, you will see that human development is a lifelong process; we evolve and
change as we age, mature, and experience our lives.
References
- Plotz, D.
(2001).
The “genius babies,” and how they grew. Slate. Retrieved from http://www.slate.com/id/100331.
- Olding, P.
(2006).
The genius sperm bank. BBC News. Retrieved from http://www.slate.com/id/100331.
- Erikson, E. H.
(1963).
Childhood and Society. Norton. New York.
Conception
occurs when an egg from the mother is fertilized by a sperm from the
father. In humans, the conception process begins with ovulation, when an ovum, or egg (the largest cell in the human body), which has
been stored in one of the mother’s two ovaries, matures and is released into the
fallopian tube. Ovulation occurs about halfway through the woman’s menstrual
cycle and is aided by the release of a complex combination of hormones. In addition to
helping the egg mature, the hormones also cause the lining of the uterus to grow thicker
and more suitable for implantation of a fertilized egg.
If the woman has had sexual intercourse within 1 or 2 days of the egg’s maturation, one of the
up to 500 million sperm deposited by the man’s ejaculation, which are traveling up the
fallopian tube, may fertilize the egg. Although few of the sperm can make the long
journey, some of the strongest swimmers succeed in meeting the egg. As the sperm reach
the egg in the fallopian tube, they release enzymes that attack the outer jelly-like
protective coating of the egg, each trying to be the first to enter. When one of the
millions of sperm enters the egg’s coating, the egg immediately responds by blocking out
all other challengers and at the same time pulling in the single successful sperm.
The Zygote
Most cells in your body have 23 pairs of chromosomes, for a total of 46. The egg and sperm
are different. Each egg and each sperm has only one set of 23 chromosomes, not a
pair. When fertilization occurs, the 23 chromosomes from the egg fuse with the
23 from the sperm to create a zygote, which starts as a fertilized egg, or ovum, with the full complement of
23 pairs of chromosomes. The zygote continues to travel down the fallopian tube
to the uterus. Although the uterus is only about 4 inches away in the woman’s
body, the journey is nevertheless a substantial one for a microscopic organism.
Consequently, fewer than half of zygotes survive beyond this earliest stage of
life. If the zygote is still viable when it completes the journey, it attaches
itself to the wall of the uterus, but if it is not, it is flushed out in the
woman’s menstrual flow. During this time, the cells in the zygote continue to
divide: The original two cells become four, those four become eight, and so on,
until there are thousands (and eventually trillions) of cells. Soon the cells
begin to differentiate, each taking on a separate
function. The earliest differentiation is between the cells on the inside of the
zygote, which begin to form the developing human being, and the cells on the
outside, which form the protective environment that provides support for the new
life throughout the pregnancy.
The Embryo
Once the zygote attaches to the wall of the uterus, it is known as
the embryo. During the embryonic phase, which lasts for
the next 6 weeks, the major internal and external organs are formed, each
beginning at the microscopic level, with only a few cells. The changes in the
embryo’s appearance continue rapidly from this point until birth.
While the inner layer of embryonic cells is busy forming the embryo, the outer layer is
forming the surrounding protective environment that helps the embryo survive the
pregnancy. This environment consists of three major structures: The amniotic sac is the fluid-filled
reservoir in which the embryo (soon to be known as a fetus) lives until
birth. The amniotic sac also acts as a cushion against outside pressure and
as a temperature regulator. The placenta is an organ that allows the exchange of nutrients between the
embryo and the mother, while at the same time filtering out harmful
material. The filtering occurs through a thin membrane that separates
the mother’s blood from the blood of the fetus, allowing them to share only the
material that can pass through the filter. Finally, the umbilical cord
links the embryo directly to the placenta and transfers all
material to the fetus. Together, the placenta and the umbilical cord
protect the fetus from many foreign agents in the mother’s system that might
otherwise pose a threat.
The Fetus
Beginning in the 9th week after conception, the embryo becomes a
fetus. The defining characteristic of the fetal stage is
growth. All the major aspects of the growing organism were formed in the
embryonic phase, and now the fetus has approximately six months to go from
weighing less than an ounce to weighing an average of 6 to 8 pounds. That’s
quite a growth spurt.
The fetus begins to take on many of the characteristics of a human being, including moving
(by the third month, the fetus can curl and open its fingers, form fists, and
wiggle its toes), sleeping, as well as early forms of swallowing and breathing.
The fetus begins to develop its senses, becoming able to distinguish tastes and
respond to sounds. Research has found that the fetus even develops some initial
preferences. A newborn prefers the mother’s voice to that of a stranger, the
languages heard in the womb over other
languages, [1] [2]
and even the kinds of foods that the mother ate during the
pregnancy. [3] By the end of
the third month of pregnancy, the sexual organs are visible.
References
- DeCasper, A. J., and Fifer, W. P.
(1980).
"Of human bonding: Newborns prefer their mothers’ voices." Science. Volume 208. Number 4448. 1174–1176 Pages.
- Moon, C., Cooper, R. P., and Fifer, W. P.
(1993).
"Two-day-olds prefer their native language." Infant Behavior and Development. Volume 16. Number 4. 495–500 Pages.
- Mennella, J. A., Jagnow, C. P., and Beauchamp, G. K.
(2001).
"Prenatal and postnatal flavor learning by human infants." Pediatrics. Volume 107. Number 6. E88 Pages.
Prenatal development is a complicated process and may not always go as planned. About 45% of
pregnancies result in a miscarriage, often without the mother ever being aware it has
occurred. [1] Although the amniotic sac and the
placenta are designed to protect the embryo, substances that can harm
the fetus, known as teratogens, may nevertheless cause
problems. Teratogens include general environmental factors, such as air pollution and
radiation, as well as cigarettes, alcohol, and drugs that the mother may use. Teratogens
do not always harm the fetus, but they are more likely to do so when they occur in
larger amounts, for long time periods, and during the more sensitive phases of fetal
development, such as when the fetus is growing most rapidly. The most vulnerable period
for many of the fetal organs is very early in the pregnancy—before the mother even knows
she is pregnant.
Harmful substances that the mother ingests may harm the child. Cigarette smoking, for example,
reduces the blood oxygen for both the mother and child and can cause a fetus to be born
severely underweight. Another serious threat is fetal alcohol syndrome
(FAS), a condition caused by maternal alcohol drinking that
can lead to numerous detrimental developmental effects, including limb and facial
abnormalities, genital anomalies, and mental retardation. One in about every
500 babies in the United States is born with fetal alcohol syndrome, and it is
considered one of the leading causes of retardation in the world
today. [2] Because there is no known safe level of alcohol
consumption for a pregnant woman, the U.S. Centers for Disease Control and Prevention
recommends that “a pregnant woman should not drink
alcohol.” [3] Therefore, the
best approach for expectant mothers is to avoid alcohol completely. Maternal drug abuse
is also of major concern and is considered one of the greatest risk factors facing
unborn children.
The environment in which the mother lives also has a major impact on infant
development. [4] [5]
Children born into homelessness or poverty are more likely to have mothers who are
malnourished; who suffer from domestic violence, stress, and other psychological
problems; and who smoke or abuse drugs. Children born into poverty are also more likely
to be exposed to teratogens. Poverty’s impact may also amplify other issues, creating
substantial problems for healthy child
development. [6] [7] Mothers
normally receive genetic and blood tests during the first months of pregnancy to
determine the health of the embryo or fetus. They may undergo sonogram, ultrasound,
amniocentesis, or other testing. The screenings detect potential birth defects,
including neural tube defects, chromosomal abnormalities (such as Down syndrome),
genetic diseases, and other potentially dangerous conditions. Early diagnosis of
prenatal problems can allow medical treatment to improve the health of the fetus.
References
- Moore, K., and Persaud, T.
(1993).
The Developing Human: Clinically Oriented Embryology. Saunders. Philadelphia. Edition 5.
- Niccols, G. A.
(1994).
"Fetal alcohol syndrome: Implications for psychologists." Clinical Psychology Review. Volume 14. Number 2. 91–111 Pages.
- Centers for Disease Control and Prevention
(2005).
Alcohol use and pregnancy. Retrieved from http://www.cdc.gov/ncbddd/factsheets/FAS_alcoholuse.pdf.
- Duncan, G., and Brooks-Gunn, J.
(2000).
"Family poverty, welfare reform, and child development." Child Development. Volume 71. Number 1. 188–196 Pages.
- Haber, M., and Toro, P.
(2004).
"Homelessness among families, children, and adolescents: An
ecological–developmental perspective." Clinical Child and Family
Psychology Review. Volume 7. Number 3. 123–164 Pages.
- Evans, G. W., and English, K.
(2002).
"The environment of poverty: Multiple stressor exposure,
psychophysiological stress, and socio-emotional adjustment." Child
Development. Volume 73. Number 4. 1238–1248 Pages.
- Gunnar, M., and Quevedo, K.
(2007).
"The neurobiology of stress and development." Annual Review of Psychology. Volume 58. Number 1. 145–173 Pages.
If all has gone well, a baby is born sometime around the 38th week of pregnancy.
The fetus is responsible, at least in part, for its own birth because chemicals
released by the developing fetal brain trigger the muscles in the mother’s
uterus to start the rhythmic contractions of childbirth. The contractions are
initially spaced at about 15-minute intervals but come more rapidly with time.
When the contractions reach an interval of 2 to 3 minutes, the mother is
requested to assist in the labor and help push the baby out.
The Newborn Arrives with Many Behaviors Intact
Newborns are relatively helpless, and they will need the protective and nurturing attention
of adults for many years. However, the newborn does have a variety of responses
to environmental stimuli that appear from the first day of life, and some start
to appear before birth. These responses are called the survival reflexes. Some, like the grasp reflex, whereby the baby holds
hard to an object that has brushed the palm of her hand, may have some real
survival value. Others, like the stepping reflex, are probably not useful
immediately, but they reflect a muscle control system that already has
behavioral patterns that will later mature when the infant is ready to use those
muscles.
Doctors test for these reflexes to determine if the nervous system is developing correctly in
the newborn and young child. The failure of a reflex to appear as a
well-organized response can be a warning sign of trouble, and the failure of a
reflex to disappear at the appropriate time can also indicate a problem.
In addition to reflexes, newborns have preferences—they like sweet-tasting foods at first,
becoming more open to salty items by 4 months of
age. [1] [2]
Newborns also prefer the smell of their mothers. An infant only 6 days old is
significantly more likely to turn toward its own mother’s breast pad than to the
breast pad of another baby’s mother, [3] and a newborn also
shows a preference for the face of its own
mother. [4]
Although infants are born ready to engage in some activities, they also contribute to their
own development through their behaviors. The child’s knowledge and abilities
increase as it babbles, talks, crawls, tastes, grasps, plays, and interacts with
the objects in the environment. [5] [6] [7] Parents
may help in this process by providing a variety of activities and experiences
for the child. Research has found that animals raised in environments with more
novel objects and that engage in a variety of stimulating activities have more
brain synapses and larger cerebral cortexes, and they perform better on a
variety of learning tasks compared with animals raised in more impoverished
environments. [8] Similar
effects likely occur in children who have opportunities to play, explore, and
interact with their
environments. [9]
learn by doing
Identify and Distinguish Basic Survival Reflexes
This exercise shows videos of seven basic infant reflexes. Infants have many more reflexes,
but these seven nicely illustrate the diversity of reflexes. Also read
the brief explanation accompanying each reflex. After you explore the
seven reflexes, you are asked to recall them and answer questions about
them. Fortunately, except for a couple of the reflexes, the names are
very informative about the behavior that the infant shows.
The Rooting Reflex
Observe: When the newborn’s cheek is lightly touched, the head
turns in the direction of the touch. This reflex aids
breastfeeding, because it allows the infant to orient its head
in the direction of the mother’s breast. The rooting reflex is
present at birth. Over the next few months, the infant gains
more and more voluntary control of these head movements, and the
reflex disappears.
The Sucking Reflex
Observe: When the infant’s lips are lightly touched,
sucking behavior occurs. It is easy to see that sucking behavior
is vital for the infant to be able to feed from the mother’s
breast, something that must be possible immediately after birth.
The sucking reflex disappears as the infant increasingly gains
voluntary control over feeding behaviors as she gains
experience.
The Blink Reflex
Observe: When the infant is touched by a light tap on
top of the head, she blinks immediately. Additional blinks
following the initial reaction to the tap on the head indicate
that the infant is “sensitized to” stimuli around the head. This
reflex is present from birth and persists throughout our lives
in some form. The blink reflex is a protective response of the
eyelids to potentially damaging objects around the eyes.
The Withdrawal Reflex
Observe: If you poke an infant (softly) on the bottom of the foot
with a sharp object, the infant will pull both legs into a
crouching position, moving them away from the source of
irritation. This reflex is present from birth, and it disappears
as a simple reflex as the response becomes more complex with
increased motor control.
The Grasp Reflex
Observe: This reflex is sometimes called the palmar reflex. When
the palm of the infant’s hand is touched or brushed, the hand
closes in a grip. The infant’s grip can be very strong. In fact,
many infants can support their own weight for a short period of
time. Stroking the back of the hand produces a release of the
grip. This reflex is present at birth and disappears as a reflex
at around 5 or 6 months of age. The grasp reflex can permit the
infant to hold an object, but it may have originated as a way
for the infant to cling to the mother as she traveled or
searched for food.
The Moro Reflex
Observe: The Moro reflex is also called the startle reflex. It is a
reaction to a startling noise or to a loss of support that feels
like falling. The head and legs extend, and the arms move up and
out. Then the arms come together across the body with the fists
clenched. The Moro reflex is present at birth, and it disappears
by 3 or 4 months of age. This reflex may be the foundation of a
body response to falling or losing hold of the mother.
The Stepping Reflex
Observe: When an infant is supported in a standing
position on a flat surface, he will move his legs in a walking
movement when his feet touch the ground. The walking reflex is
present at birth, then disappears at about 6 weeks of age. It
probably reflects an innate muscular basis for the walking
movement that will be developed later.
The Babinsky Reflex
Observe: If you stroke the bottom of the infant’s foot from heel to
toe, he spreads his toes out except for the big toe, which moves
upward, and he turns the foot inward. This reflex shows a
complex, innate muscular reaction to the kinds of stimuli we
feel when walking. It is present at birth and generally
disappears by the end of the first year as the infant gains more
motor control.
References
- Beauchamp, D. K., Cowart, B. J., Menellia, J.
A., and Marsh, R. R.
(1994).
"Infant salt taste: Developmental, methodological, and contextual
factors." Developmental Psychology. Volume 27. Number 6. 353–365 Pages.
- Blass, E. M., and Smith, B. A.
(1992).
"Differential effects of sucrose, fructose, glucose, and lactose on
crying in 1- to 3-day-old human infants: Qualitative and quantitative
considerations." Developmental Psychology. Volume 28. Number 5. 804–810
Pages.
- Porter, R. H., Makin, J. W., Davis, L. B., and
Christensen, K. M.
(1992).
"Breast-fed infants respond to olfactory cues from their own mother
and unfamiliar lactating females." Infant Behavior and Development.
Volume 15. Number 1. 85–93 Pages.
- Bushnell, I. W. R., Sai, F., and Mullin, J. T.
(1989).
"Neonatal recognition of the mother’s face." British Journal of
Developmental Psychology. Volume 7. Number 1. 3–15 Pages.
- Gibson, E. J., Rosenzweig, M. R., and Porter, L. W.
(1988).
Annual Review of Psychology, Vol. 39.
Chapter Exploratory behavior in the development of perceiving, acting,
and the acquiring of knowledge. Annual Reviews. Palo Alto, CA. 1–41
Pages.
- Gibson, E. J., and Pick, A. D.
(2000).
An Ecological Approach to Perceptual Learning and Development. Oxford University Press. New York.
- Smith, L. B., and Thelen, E.
(2003).
"Development as a dynamic system." Trends in Cognitive Sciences. Volume 7. Number 8. 343–348 Pages.
- Juraska, J. M., Henderson, C., and Müller, J.
(1984).
"Differential rearing experience, gender, and radial maze
performance." Developmental Psychobiology. Volume 17. Number 3. 209–215
Pages.
- Soska, K. C, Adolph, K. E., and Johnson, S. P.
(2010).
"Systems in development: Motor skill acquisition facilitates
three-dimensional object completion." Developmental Psychobiology.
Volume 46. Number 1. 129–138 Pages.
Childhood is a time when changes occur quickly. The child is growing physically, and
cognitive abilities are also developing. During this time the child learns to
actively manipulate and control the environment and is first exposed to the
requirements of society, particularly the need to control the bladder and
bowels. According to Erik Erikson, the challenges the child must confront in
childhood relate to the development of initiative, competence, and independence.
Children need to learn to explore the world, to become self-reliant, and to make
their own way in the environment.
These skills do not come overnight. Neurological changes during childhood provide children
the ability to do some things at certain ages and yet make it impossible for
them to do other things. This fact was made apparent through the groundbreaking
work of the Swiss psychologist Jean Piaget. During the 1920s, Piaget was
administering intelligence tests to children in an attempt to determine the
kinds of logical thinking children are capable of. In the process of testing the
children, Piaget became intrigued not so much by the answers the children got
right but more by the answers they got wrong. Piaget believed that the incorrect
answers the children gave were not mere shots in the dark but rather represented
specific ways of thinking unique to the children’s developmental stage. Just as
almost all babies learn to roll over before they learn to sit up by themselves,
and learn to crawl before they learn to walk, Piaget believed that children gain
their cognitive ability in a developmental order. These insights—that children
at different ages think in fundamentally different ways—led to Piaget’s stage model of cognitive development.
Piaget argued that children do not just passively learn but also actively try to make sense
of their worlds. He argued that as they learn and mature, children develop schemas—patterns of knowledge in
long-term memory—that help them remember, organize, and respond to
information. Furthermore, Piaget thought that when children experience
new things, they attempt to reconcile the new knowledge with existing schemas.
Piaget believed that children use two distinct methods in doing so, methods he
called assimilation and accommodation.
When children employ assimilation, they use already developed schemas to understand new information. If
children have learned a schema for horses, then they may call the striped animal
they see at the zoo a horse rather than a zebra. In this case, children fit the
existing schema to the new information and label the new information with the
existing knowledge. Accommodation, on the other hand,
involves learning new information, and thus changing the
schema. When a mother says, “No, honey, that’s a zebra, not a horse,”
the child may adapt the schema to fit the new stimulus, learning that there are
different types of four-legged animals, only one of which is a horse.
learn by doing
A schema is an organized set of related
information in long-term memory. A concept (e.g., furniture or
things that can be used as a hammer) is an example of a schema.
Behaviors, such as movements needed to ride a bicycle, can also be
schemas.
According to Piaget, we develop and use schemas throughout our lives.
However, at different times in our lives, different schemas are likely
to be particularly important.
Piaget’s most important contribution to understanding cognitive development, and the
fundamental aspect of his theory, was the idea that development occurs in unique and
distinct stages, with each stage occurring at a specific time, in a sequential manner,
and in a way that allows the child to think about the world using new capacities.
Piaget’s stages of cognitive development are summarized in the following table.
| Piaget's Stages of Cognitive Development |
|---|
| From Flat World Knowledge, Introduction to Psychology, v1.0, CC-BY-NC-SA. |
| Stage |
Approximate Age Range |
Characteristics |
Stage Attainments |
| Sensorimotor |
Birth to about 2 years |
The child experiences the world through the fundamental senses of seeing,
hearing, touching, and tasting. |
Object permanence |
| Preoperational |
2 to 7 years |
Children acquire the ability to internally represent the world through language
and mental imagery. They also start to see the world from other people's
perspectives. |
Theory of mind; rapid increase in language ability |
| Concrete operational |
7 to 11 years |
Children become able to think logically. They can increasingly perform
operations on objects that are only imagined. |
Conservation |
| Formal operational |
11 years to adulthood |
Adolescents can think systematically, can reason about abstract concepts, and
can understand ethics and scientific reasoning. |
Abstract logic |
|
Sensorimotor Stage
The first developmental stage for Piaget was the sensorimotor stage,
the cognitive stage that begins at birth and lasts until
around the age of 2. It is defined by the direct physical interactions that
babies have with the objects around them. During this stage, babies
form their first schemas by using their primary senses—they stare at, listen to,
reach for, hold, shake, and taste the things in their environments. During the
sensorimotor stage, babies’ use of their senses to perceive the world is so
central to their understanding that whenever babies do not directly perceive
objects, as far as they are concerned, the objects do not exist. Piaget found,
for instance, that if he first interested babies in a toy and then covered the
toy with a blanket, children who were younger than 6 months of age would act as
if the toy had disappeared completely—they never tried to find it under the
blanket but would nevertheless smile and reach for it when the blanket was
removed. Piaget found that it was not until about 8 months that the children
realized the object was merely covered and not gone. Piaget used the term object permanence to refer to the
child’s ability to know that an object exists even when the object cannot be
perceived.
Children younger than about 8 months of age do not understand object
permanence.
Preoperational Stage
At about 2 years of age, and until about 7 years of age, children move into the preoperational stage. During this stage, children begin to use language and to think more abstractly
about objects, but their understanding is more intuitive and without much
ability to deduce or reason. The thinking is preoperational, meaning
that the child lacks the ability to operate on or transform objects mentally. In
one study that showed the extent of this inability, Judy
DeLoache [1] showed children a room within a small dollhouse.
Inside the room, a small toy was visible behind a small couch. The researchers
took the children to another lab room, which was an exact replica of the
dollhouse room, but full sized. When children who were 2.5 years old were asked
to find the toy, they did not know where to look—they were simply unable to make
the transition across the changes in room size. Three-year-old children, on the
other hand, immediately looked for the toy behind the couch, demonstrating that
they were improving their operational skills.
The inability of young children to view transitions also leads them to be egocentric—unable to readily see and understand other people’s
viewpoints. Developmental psychologists define the theory of
mind as the ability to take another person’s
viewpoint, and the ability to do so increases rapidly during the
preoperational stage. In one demonstration of the development of theory of mind,
a researcher shows a child a video of another child (let’s call her Anna)
putting a ball in a red box. Then Anna leaves the room, and the video shows that
while she is gone, a researcher moves the ball from the red box into a blue box.
As the video continues, Anna comes back into the room. The child is then asked
to point to the box where Anna will probably look to find her ball. Children who
are younger than 4 years of age typically are unable to understand that Anna
does not know the ball has been moved, and they predict that she will look for
it in the blue box. After 4 years of age, however, children have developed a
theory of mind—they realize that different people can have different viewpoints,
and that (although she will be wrong) Anna will nevertheless think the ball is
still in the red box.
References
- DeLoache, J. S.
(1987).
"Rapid change in the symbolic functioning of very young children." Science. Volume 238. Number 4833. 1556–138 Pages.
Concrete Operational Stage
After about 7 years of age, the child moves into the concrete operational
stage, which is marked by more frequent and more
accurate use of transitions, operations, and abstract concepts, including
those of time, space, and numbers. An important milestone during the
concrete operational stage is the development of conservation—the understanding that changes in the
form of an object do not necessarily mean changes in the quantity of the
object. Children younger than 7 years generally think that a tall glass
holds more milk than a shorter, wider glass, and they continue to believe so
even when they see the same milk poured back and forth between the glasses. It
appears that these children focus only on one dimension (in this case, the
height of the glass) and ignore the other dimension (width). However, when
children reach the concrete operational stage, their abilities to understand
such transformations make them aware that, although the milk looks different in
the different glasses, the amount must be the same.
learn by doing
Associate each of the following situations with a phenomenon or
"attainment."
You have two identical glasses with exactly the same amount of water in each. You pour the
water from one of the tall, thin glasses into a low, wide bowl. Veronica
is watching as you do this. You then ask her, "Which one holds more,
this one (the tall, thin glass) or this one (the low, wide bowl)?"
She responds that the tall, thin glass has more.
You are playing with a very young infant, dangling a doll in front of her as
she grabs it or tries to grab it when you move it. Both of you are having fun.
Then you wiggle the doll in front of her and, as she watches intently, you put
it under a blanket. She briefly looks around and then seems to lose interest in
the doll.
A child watches as you tell the following story using dolls: "Becky walks into
her bedroom carrying her favorite book. She puts the book in the top drawer of
her dresser, closes the drawer, and leaves the room. A few minutes later, her
brother Zack comes into the room, takes the book from the drawer, and puts it in
the toy box. Then Zack leaves the room. Then Becky comes back to the room to get
her book." You ask the child to tell you where Becky will look first. The child
says, "In the toy box!" without hesitation.
Formal Operational Stage
At about 11 years of age, children enter the formal operational stage,
which is marked by the ability to think in abstract terms and
to use scientific and philosophical lines of thought. Children in the
formal operational stage are better able to systematically test alternative
ideas to determine their influences on outcomes. For instance, rather than
haphazardly changing different aspects of a situation that allows no clear
conclusions to be drawn, they systematically make changes in one thing at a time
and observe what difference that particular change makes. They learn to use
deductive reasoning, such as “if this, then that,” and they become capable of
imagining situations that “might be” rather than just those that actually
exist.
Piaget’s theories have made a substantial and lasting contribution to developmental psychology.
His contributions include the idea that children are not merely passive receptacles of
information but actively engage in acquiring new knowledge and making sense of the world
around them. This general idea has generated many other theories of cognitive
development, each designed to help us better understand the development of the child’s
information-processing
skills. [1] [2]
Furthermore, the extensive research that Piaget’s theory has stimulated has generally
supported his beliefs about the order in which cognition develops. Piaget’s work has
also been applied in many domains—for instance, many teachers use Piaget’s stages to
develop educational approaches aimed at the level children are developmentally prepared
for. [3] [4]
Over the years, Piagetian ideas have been refined. For instance, it is now believed that object
permanence develops gradually, rather than immediately, as a true stage model would
predict, and that it can sometimes develop much earlier than Piaget expected. Renée
Baillargeon and her colleagues [5] [6] placed babies
in a habituation setup, having them watch as an object was placed behind a screen,
entirely hidden from view. The researchers then arranged for the object to reappear from
behind another screen in a different place. Babies who saw this pattern of events looked
longer at the display than did babies who witnessed the same object physically being
moved between the screens. These data suggest the babies were aware that the object
still existed even though it was hidden behind the screen and thus that they were
displaying object permanence as early as 3 months of age rather than the 8 months that
Piaget predicted.
Another factor that might have surprised Piaget is the extent to which a child’s social
surroundings influence learning. In some cases, children progress to new ways of
thinking and retreat to old ones depending on the type of task they are performing, the
circumstances they find themselves in, and the nature of the language used to instruct
them. [7] And children in different cultures show
somewhat different patterns of cognitive development. Dasen [8] found that
children in non-Western cultures moved to the next developmental stage about a year
later than did children from Western cultures and that level of schooling also
influenced cognitive development. In short, Piaget’s theory probably understated the
contribution of environmental factors to social development.
References
- Klahr, D., and McWhinney, B.
(1998).
Handbook of Child Psychology: Cognition, Perception, and Language, Vol. 2. Chapter Information processing. Wiley. New York. Edition 5. 631–678 Pages. D. Kuhn and R. S. Siegler (Eds.).
- Shrager, J., and Siegler, R. S.
(1998).
"SCADS: A model of children’s strategy choices and strategy
discoveries." Psyhological Science. Volume 9. Number 5. 405–422 Pages.
- Driscoll, M. P.
(1994).
Psychology of Learning for Instruction. Allyn and Bacon. Boston.
- Levin, I., Siegler, S. R., and Druyan, S.
(1990).
"Misconceptions on motion: Development and training effects." Child Development. Volume 61. Number 5. 1544–1556 Pages.
- Levin, I., Siegler, S. R., and Druyan, S.
(2004).
"Infants’ physical world." Current Directions in Psychological Science. Volume 13. Number 3. 89–94 Pages.
- Wang, S. H., Baillargeon, R., and Brueckner, L.
(2004).
"Young infants’ reasoning about hidden objects: Evidence from
violation-of-expectation tasks with test trials only." Cognition. Volume
93. Number 3. 167–198 Pages.
- Courage, M. L., and Howe, M. L.
(2002).
"From infant to child: The dynamics of cognitive change in the
second year of life." Psychological Bulletin. Volume 128. Number 2.
250–276 Pages.
- Dasen, P. R.
(1972).
"Cross-cultural Piagetian research: A summary." Journal of Cross-Cultural Psychology. Volume 3. Number 1. 23–39 Pages.
Piaget’s background was in biology, and he viewed the cognitive development
process as something like physical maturation in which changes occur inevitably
as the individual gets older. Piaget has been criticized for not giving
sufficient credit to the impact of experience on the growth of the child’s
skills and knowledge. Here we discuss the ideas of another important figure in
early developmental psychology, Lev Vygotsky.
Lev Vygotsky (1896–1934) was a Russian (Soviet) psychologist whose emphasis on
the interaction of the parent (or other caregivers) and child has had a profound
influence on many developmental psychologists. According to Vygotsky, learning
starts with doing something—interacting with the world. For instance, an infant
tries to communicate with an adult to get some juice, and that process of
interacting with the adult—whether successful or not—is a learning experience
that is a little step in cognitive development.
In Vygotsky’s theory, our mental processes are actions that are internalized, which means they take place
symbolically in our minds. For example, the child’s early speech has
the purpose of communicating needs and desires to others, particularly to the
child’s caregivers. As the child uses speech regularly to interact with adults
and other children, he or she develops a parallel system of silent inner speech,
which is the foundation of reasoning and problem solving. In Vygotsky’s view,
this inner speech is not simply the act of talking to
oneself. It is more abstract and condensed than language spoken aloud, and it
would be unrecognizable if we did somehow broadcast it so we could hear it.
Inner speech is used to explore ideas and regulate and understand our own
behaviors. One type of evidence Vygotsky uses for this theory of internalization
of speech is the fact that children of 3 and 4 years of age often talk aloud
when they are solving a problem or regulating their own behavior, even when they
are alone. By the time they are 5 or 6, the amount of self-talk diminishes
dramatically.
This period when the child talks aloud to himself or herself is considered a
transitional phase between the early stage, when the child can speak but lacks
internalized thought processes and the later stage when the child has abilities
like those of the adult to reason and analyze ideas without making a sound. An
important difference between this view and Piaget’s is that thinking does not
just naturally appear and mature over time. Rather, it is the consequence of a
great deal of practice that includes constant spoken interactions with other
people, particularly parents or other caregivers.
Vygotsky saw the role of parents and other caregivers as essential to normal
cognitive development. Parents model behaviors by doing things while the child
watches, and they are constantly around as the child explores objects, witnesses
events, and communicates with others. Vygotsky’s particular contribution to
understanding how adults help children learn is the concept of scaffolding. A scaffold is a support structure used by construction
workers to reach higher places on a building than they could by merely standing
on the ground. Using this idea as an analogy, Vygotsky suggested that caregivers can support the child to achieve higher cognitive
levels by providing support and guidance. They do this by helping the
child to do things for herself rather than by doing things for the child. For
instance, a parent can help a child learn the meaning of a new word by pointing
at the object it labels or by holding the object so that the child can see it
and explore it. Using a different example, a parent can provide scaffolding for
a child who is trying to open a box by orienting the box at a convenient angle
and assuring that the lid is a type that can be opened by the child.
Vygotsky suggested that the child is most likely to learn and mature cognitively
if the adult is sensitive to the child’s abilities and limitations. Ideally, the
adult understands what kinds of tasks and activities will challenge the child
without being so difficult that they lead to complete failure. Vygotsky used the
daunting phrase zone of proximal development to describe
abilities that a child is just starting to be able to
use. A task that is too difficult is beyond the zone of proximal
development, and a task that is too easy is not a challenge for the child, so it
will not lead to cognitive growth. Putting this idea together with scaffolding,
Vygotsky suggested that the effective caregiver knows what tasks and activities
the child is just starting to be able to handle (the zone of proximal
development) and, by providing just enough assistance (scaffolding) that the
child can avoid frustration yet can explore and succeed, the parent helps the
child develop new abilities and greater understanding than would be possible
without help.
It is through the remarkable increases in cognitive ability that children learn to
interact with and understand their environments. But these cognitive skills are only
part of the changes that occur during childhood. Equally crucial is the development of
the child’s social skills—the ability to understand, predict, and create bonds with the
other people in their environments.
One of the important milestones in a child’s social development is learning about his or
her self-existence. Self-awareness is an important part of
consciousness; as the infant’s cognitive skills develop, so does the awareness of others
and self. Self-awareness is the realization that he or she is a distinct individual,
whose body, mind and actions are separate from those of other people. At about age 5
months, infants begin to realize that they exist separately from their caregivers.
Self-awareness continues with the emergence of the self-concept. The self-concept is a knowledge representation or schema that
contains knowledge about ourselves, including our beliefs about our personality
traits, physical characteristics, abilities, values, goals, and roles, as well as
the knowledge that we exist as individuals. [1]
Some animals, including chimpanzees, orangutans, and perhaps dolphins, have at least a
primitive sense of self. [2] In one study, [3]
researchers painted a red dot on the foreheads of
anesthetized chimpanzees and then placed each animal in a cage with a mirror. When the
chimps woke up and looked in the mirror, they touched the dot on their faces, not the
dot on the faces in the mirror. These actions suggest that the chimps understood they
were looking at themselves and not at other animals, and thus we can assume they are
able to realize that they exist as individuals. On the other hand, most other animals,
including, for instance dogs, cats, and monkeys, never behave as if they realize they
are seeing themselves in the mirror.
Infants who have a similar red dot painted on their foreheads recognize themselves in a
mirror in the same way that the chimps do, and they do this by about 18 months of
age. [4] Other examples of
self-awareness are their ability to use language that refers to "I, me, mine, and my",
particularly when referring to their possessions such as toys. By age 2, children begin
to show emotions such as pride, shame and embarrassment.
Children's knowledge about the self continues to develop as
cognitive and language skills
increase due to brain maturity and learning from their
sociocultural surroundings about
sex and gender differences. By age 2, children are aware of
their biological sex, which
is their physical body parts associated with being a boy or a
girl. As children grow
older, they develop a gender identity which is the
psychological and sociocultural
characteristics of maleness or femaleness that are
associated with one’s physical sex. Children express their gender
identity by insisting on
playing with toys that they associate with their gender such
as dolls for girls and
trucks or cars for boys. Their awareness of the gender
differences in clothing,
playmates, and future careers provide further evidence of
the young child’s sense of
gender identity.
By age 4, self-descriptions are likely to be based on physical features,
such as hair color and possessions, and by about age 6, children can understand their basic
emotions and the basic concepts of their personality traits, demonstrated by statements such as, “I am a nice
person.” [5]
Soon after children enter grade school (at about age 6 or 7), they
begin to evaluate themselves against their observations of other children, a
process known as social comparison. For example, a child might
describe himself as being faster than one boy but slower than another. [6] According to
Erikson, the important component of this process is the development of competence and
autonomy—the recognition of one’s own abilities relative to other children. And children
increasingly show awareness of social situations—they understand that other people are
looking at and judging them the same way they are looking at and judging others. [7]
References
- Kagan, J.
(1991).
"The theoretical utility of constructs of self." Developmental Review. Volume 11. Number 3. 244–250 Pages.
- Boysen, S. T., and Himes, G. T.
(1999).
"Current issues and emerging theories in animal cognition." Annual
Review of Psychology. Volume 50. Number 1. 683–705 Pages.
- Gallup, G. G., Jr.
(1970).
"Chimpanzees: Self-recognition." Science. Volume 167. Number 3914. 86–887 Pages.
- Povinelli, D. J., Landau, K. R., and Perilloux, H. K.
(1996).
"Self-recognition in young children using delayed versus live feedback:
Evidence of a developmental asynchrony." Child Development. Volume 67. Number 4. 1540–1554 Pages.
- Harter, S.
(1998).
Handbook of Child Psychology: Social, Emotional, and Personality
Development, Vol. 3. Chapter The development of self-representations. Wiley. New York. Edition 5. 553–618 Pages. W. Damon and N. Eisenberg (Eds.).
- Moretti, M. M., and Higgins, E. T.
(1990).
Competence Considered. Chapter The
development of self-esteem vulnerabilities: Social and cognitive
factors in developmental psychopathology. Yale
University Press. New Haven, CT. 286–314 Pages. R. J. Sternberg and J.
Kolligian, Jr. (Eds.).
- Doherty, M. J.
(2009).
Theory of Mind: How Children Understand Others’ Thoughts and
Feelings. Psychology Press. New York.
One of the most important behaviors a child must learn is how to be accepted by
others—the development of close and meaningful social relationships. The emotional bonds we develop with those with whom we feel closest, and
particularly the bonds an infant develops with the mother or primary caregiver,
are called attachment. [1]
As late as the 1930s, psychologists believed that children who were raised in
institutions such as orphanages, and who received good physical care and proper
nourishment, would develop normally, even if they had little interaction with their
caretakers. But studies by the developmental psychologist John Bowlby [2]
and others showed that these children did not develop normally—they
were usually sickly, emotionally slow, and generally unmotivated. These observations
helped make it clear that normal infant development requires successful attachment with
a caretaker.
In one classic study showing the importance of attachment, Wisconsin University
psychologists Harry and Margaret Harlow investigated the responses of young monkeys,
separated from their biological mothers, to two surrogate mothers introduced to their
cages. One—the wire mother—consisted of a wooden head, a mesh of cold metal wires, and a
bottle of milk from which the baby monkey could drink. The second mother was a
foam-rubber form wrapped in a heated terry-cloth blanket. The Harlows found that
although the infant monkeys went to the wire mother for food, they overwhelmingly
preferred and spent significantly more time with the warm terry-cloth mother that
provided no food but did provide comfort. [3]
The studies by the Harlows showed that young monkeys preferred the warm mother that
provided a secure base to the cold mother that provided food.
The Harlows’ studies confirmed that babies have social as well as physical needs. Both
monkeys and human babies need a secure base that allows them to feel safe. From this
base, they can gain the confidence they need to venture out and explore their worlds.
Erikson agreed with the importance of a secure base, arguing that the most important
goal of infancy was the development of a basic sense of trust in one’s caregivers.
Review this first stage in the table "Erik Erikson's Framework for Development."
Developmental psychologist Mary Ainsworth, a student of John Bowlby, was interested in
studying the development of attachment in infants. Ainsworth created a laboratory test
that measured an infant’s attachment to his or her parent. The test is called the
Strange Situation Classification because it is conducted in a context that is unfamiliar
to the child and therefore likely to heighten the child’s need for his or her
parent. [4] During the procedure, which
lasts about 20 minutes, the parent and the infant are first left alone while the infant
explores the room full of toys. Then a strange adult enters the room and talks for a
minute to the parent, after which the parent leaves the room. The stranger stays with
the infant for a few minutes, and then the parent reenters and the stranger leaves the
room. During the entire session, a video camera records the child’s behaviors, which are
later coded by trained coders.
In the Strange Situation, children are observed responding to the comings and goings of
parents and unfamiliar adults in their environments.
On the basis of their behaviors, the children are categorized into one of four groups,
where each group reflects a different kind of attachment relationship with the
caregiver. A child with a secure attachment style
usually explores freely while the mother is present and engages with
the stranger. The child may be upset when the mother departs but is also happy
to see the mother return. A child with an ambivalent (sometimes called
insecure-resistant) attachment style
is wary about the situation in general, particularly the stranger,
and stays close or even clings to the mother rather than exploring the toys.
When the mother leaves, the child is extremely distressed and is ambivalent when she
returns. The child may rush to the mother but then fail to cling to her when she picks
up the child. A child with an avoidant (sometimes called
insecure-avoidant) attachment style
will avoid or ignore the mother, showing little emotion when the
mother departs or returns. The child may run away from the mother when she
approaches. The child will not explore very much, regardless of who is there, and the
stranger will not be treated much differently from the mother.
Finally, a child with a disorganized attachment style
seems to have no consistent way of coping with the stress of the
strange situation—the child may cry during the separation but avoid the mother when
she returns, or the child may approach the mother but then freeze or fall to the
floor. Although some cultural differences in attachment styles have been
found, [5] research has also
found that the proportion of children who fall into each of the attachment categories is
relatively constant across cultures.
You might wonder whether differences in attachment style are determined more by the child
(nature) or by the parents (nurture). Most developmental psychologists believe that
socialization is primary, arguing that a child becomes securely attached when the mother
is available and able to meet the needs of the child in a responsive and appropriate
manner and that the insecure styles occur when the mother is insensitive and responds
inconsistently to the child’s needs. In a direct test of this idea, Dutch researcher
Dymphna van den Boom [6] randomly assigned
some babies’ mothers to a training session in which they learned to better respond to
their children’s needs. The research found that these mothers’ babies were more likely
to show a secure attachment style than were babies of mothers in a control group that
did not receive training.
References
- Cassidy, J. E., and Shaver, P. R. E.
(1999).
Handbook of Attachment: Theory, Research, and Clinical
Applications. Guilford Press. New York.
- Bowlby, J.
(1953).
"Some pathological processes set in train by early mother-child
separation." Journal of Mental Science. Volume 99. Number 415. 265–272 Pages.
- Harlow, H.
(1958).
"The nature of love." American Psychologist. Volume 13. Number 12. 573–685 Pages.
- Ainsworth, M. S., Blehar, M. C., Waters, E., and Wall, S.
(1978).
Patterns of Attachment: A Psychological Study of the Strange
Situation. Lawrence Erlbaum Associates. Hillsdale, NJ.
- Rothbaum, F., Weisz, J., Pott, M., Miyake, K., and Morelli,
G.
(2000).
"Attachment and culture: Security in the United States and
Japan." American Psychologist. Volume 55. Number 10. 1093–1104 Pages.
- Van den Boom, D. C.
(1994).
"The influence of temperament and mothering on attachment and exploration:
An experimental manipulation of sensitive responsiveness among lower-class
mothers with irritable infants." Child Development. Volume 65. Number 5. 1457–1476 Pages.
The attachment behavior of the child is also likely influenced, at least in part, by temperament, the innate personality
characteristics of the infant. Specifically, temperament is the infant’s distinctive
pattern of attention, arousal, and reactivity to new or novel situations.
Temperament is displayed by some children being warm, friendly, and responsive, whereas
others display a more irritable, less manageable, and difficult-to-console behavior. A
specific temperament pattern appears early, is relatively stable and long-lasting from
early infancy and appears to become the basis for one’s personality that is displayed
throughout adulthood. Researchers [1]
studied differences in infants’ temperaments by
interviewing mothers with 2- to 3-month-old infants and then observing these same
infants repeatedly over the next 7 years. The researchers then rated each infant on nine
components of temperament, including activity level, attention span, fussiness, and
mood. On the basis of these ratings, they divided infants into four categories.
-
Easy babies, who made up 40% of the sample, were happy and
cheerful, had regular sleeping and eating habits, and adapted quickly to new
situations.
-
Slow-to-warm-up babies, who made up 15% of the sample, were
more withdrawn, were moody, and tended to take longer to adapt to new
situations.
-
Difficult babies, who made up 10% of the sample, were fussy,
fearful of new situations, and more intense in their reactions. During the course of
the 7-year study, difficult babies developed more serious emotional problems than
did the easy or slow-to-warm-up babies.
-
No-single-category babies, who made up 35% of the sample, had
a variety of traits and could not be classified into one of the other three
categories.
These differences may also play a role in attachment. [2] [3]
Taken together, it seems safe to say that attachment, like most other developmental
processes, is affected by an interplay of genetic and socialization influences.
References
- Thomas, A., and Chess, S.
(1977).
Temperament and Development. Brunner/Mazel. New York.
- Gillath, O., Shaver, P. R., Baek, J.-M.,
and Chun, D. S.
(2008).
"Genetic correlates of adult attachment style." Personality and
Social Psychology Bulletin. Volume 34. Number 10. 1396–1405 Pages.
- Seifer, R., Schiller, M., Sameroff, A. J., Resnick, S., and Riordan,
K.
(1996).
"Attachment, maternal sensitivity, and infant temperament during the first
year of life." Developmental Psychology. Volume 32. Number 1. 12–25 Pages.
One thing you may have wondered about as you grew up, and which you may start to think
about again if you decide to have children yourself, concerns the skills involved in
parenting. Some parents are strict, others are lax; some parents spend a lot of time
with their kids, trying to resolve their problems and helping to keep them out of
dangerous situations, whereas others leave their children with nannies or in day care.
Some parents hug and kiss their kids and tell them they love them over and over every
day, whereas others never do. Do these behaviors matter? And what makes a “good
parent”?
We have already considered two answers to this question in the form of what all children
require: (1) babies need a conscientious mother who does not smoke, drink, or use drugs
during her pregnancy, and (2) infants need caretakers who are consistently available,
loving, and supportive to help them form a secure base. One case in which these basic
goals are less likely to be met is when the mother is an adolescent. Adolescent mothers
are more likely to use drugs and alcohol during their pregnancies, to have poor
parenting skills in general, and to provide insufficient support for the
child. [1] As a result, the babies of
adolescent mothers have higher rates of academic failure, delinquency, and incarceration
than do children of older mothers. [2]
Normally, it is the mother who provides early attachment, but fathers are not irrelevant.
Studies have found that children whose fathers are more involved with childrearing tend
to be more cognitively and socially competent, more empathic, and psychologically better
adjusted than children whose fathers are less
involved. [3] In fact, Amato [4]
found that, in some cases, the role of the father can be as important
as or even more important than that of the mother in the child’s overall psychological
health and well-being. Amato concluded, “Regardless of the quality of the mother–child
relationship, the closer adult offspring were to their fathers, the happier, more
satisfied, and less distressed they reported being” (p. 1039).
As the child grows, parents take on one of four types of parenting
styles—parental behaviors that determine the nature of
parent–child interactions and that guide their interaction with the child.
These styles depend on whether the parent is more or less demanding and more or less
responsive to the child. Authoritarian parents are demanding but not responsive. They impose rules and expect
obedience, tending to give orders (“Eat your food!”) and enforcing their commands with
rewards and punishment, without providing any explanation of where the rules came from
except “Because I said so!” Permissive parents, on the other hand,
tend to make few demands and give little punishment, but they are
responsive in the sense that they generally allow their children to make their own
rules. Authoritative parents are demanding (“You must be home by curfew”), but they are also responsive to the needs
and opinions of the child (“Let’s discuss what an appropriate curfew might
be”). They set rules and enforce them, but they also explain and discuss the reasons
behind the rules. Finally, rejecting-neglecting parents are undemanding and unresponsive overall.
Parenting style is based on the combination of demandingness and responsiveness. The
authoritative style, characterized by both responsiveness and demandingness, is the most
effective.
Many studies of children and their parents, using different methods, measures, and
samples, have reached the same conclusion: that authoritative parenting, compared to the
other three styles, is associated with a wide range of psychological and social
advantages for children. Children whose parents use the authoritative style (demanding
but responsive) demonstrate better psychological adjustment, school performance, and
psychosocial maturity than do children whose parents use the other styles. These
children tend to be more independent, socially adept, and
self-confident. [5] [6] Although there
are some cultural differences in parenting styles among racial and ethnic groups,
cross-cultural research indicates that authoritative parenting leads to the most
positive outcomes across all groups.
Despite that different parenting styles are differentially effective overall, every child
is different and parents must be adaptable. Some children have particularly difficult
temperaments, and these children require more parenting. Because these difficult
children demand more parenting, the behaviors of the parents matter more for the
children’s development than they do for other, less demanding children who require less
parenting overall. [7] These findings remind us how
the behavior of the child can influence the behavior of the people in his or her
environment.
Although childrearing demands a focus on the child, the parents must never forget about
each other. Parenting is time consuming and emotionally taxing, and the parents must
work together to create a relationship in which both mother and father contribute to the
household tasks and support each other. It is also important for the parents to invest
time in their own intimacy, as happy parents are more likely to stay together, and
divorce has a profoundly negative impact on children, particularly during and
immediately after the
divorce. [8] [9]
References
- Ekéus, C., Christensson, K., and Hjern, A.
(2004).
"Unintentional and violent injuries among pre-school children of
teenage mothers in Sweden: A national cohort study." Journal of
Epidemiology and Community Health. Volume 58. Number 8. 680–685 Pages.
- Moore, M. R., and Brooks-Gunn, J.
(1990).
Handbook of Parenting: Being and Becoming a Parent, Vol. 3. Chapter Adolescent parenthood. Lawrence Erlbaum Associates. Mahwah, NJ. Edition 2. 173–214 Pages. M. H. Bornstein (Ed.).
- Rohner, R. P., and Veneziano, R. A.
(2001).
"The importance of father love: History and contemporary evidence."
Review of General Psychology. Volume 5. Number 4. 382–405 Pages.
- Amato, P. R.
(1994).
"Father-child relations, mother-child relations, and offspring
psychological well-being in adulthood." Journal of Marriage and the
Family. Volume 56. Number 4. 1031–1042 Pages.
- Baumrind, D.
(1996).
"The discipline controversy revisited." Family Relations. Volume 45. Number 4. 405–414 Pages.
- Grolnick, W. S., and Ryan, R. M.
(1989).
"Parent styles associated with children’s self-regulation and
competence in school." Journal of Educational Psychology. Volume 81.
Number 2. 143–154 Pages.
- Pluess, M., and Belsky, J.
(2010).
"Differential susceptibility to parenting and quality child care."
Developmental Psychology. Volume 46. Number 2. 379–390 Pages.
- Burt, S. A., Barnes, A. R., McGue, M., and
Iacono, W. G.
(2008).
"Parental divorce and adolescent delinquency: Ruling out the impact
of common genes." Developmental Psychology. Volume 44. Number 6.
1668–1677 Pages.
- Ge, X., Natsuaki, M. N., and Conger, R. D.
(2006).
"Trajectories of depressive symptoms and stressful life events
among male and female adolescents in divorced and nondivorced families."
Development and Psychopathology. Volume 18. Number 1. 253–273 Pages.
Adolescence is defined as the years between the onset of puberty and the beginning of
adulthood. In the past, when people were likely to marry in their early 20s or
younger, this period might have lasted only 10 years or less—starting roughly between
ages 12 and 13 and ending by age 20, at which time the child got a job or went to work
on the family farm, married, and started his or her own family. Today, children mature
more slowly, move away from home at later ages, and maintain ties with their parents
longer. For instance, children may go away to college but still receive financial
support from parents, and they may come home on weekends or even to live for extended
time periods. Thus the period between puberty and adulthood may well last into the late
20s, merging into adulthood itself. In fact, it is appropriate now to consider the
period of adolescence and that of emerging adulthood (the ages between 18 and the middle
or late 20s) together.
During adolescence, the child continues to grow physically, cognitively, and emotionally,
changing from a child into an adult. The body grows rapidly in size and the sexual and
reproductive organs become fully functional. At the same time, as adolescents develop
more advanced patterns of reasoning and a stronger sense of self, they seek to forge
their own identities, developing important attachments with people other than their
parents. Particularly in Western societies, where the need to forge a new independence
is critical, [1] [2] this period can be
stressful for many children, as it involves new emotions, the need to develop new social
relationships, and an increasing sense of responsibility and independence.
Although adolescence can be a time of stress for many teenagers, most of them weather the
trials and tribulations successfully. For example, the majority of adolescents
experiment with alcohol sometime before high school graduation. Although many will have
been drunk at least once, relatively few teenagers will develop long-lasting drinking
problems or permit alcohol to adversely affect their school or personal relationships.
Similarly, a great many teenagers break the law during adolescence, but very few young
people develop criminal careers. [3] These facts do not,
however, mean that using drugs or alcohol is a good idea. The use of recreational drugs
can have substantial negative consequences, and the likelihood of these problems
(including dependence, addiction, and even brain damage) is significantly greater for
young adults who begin using drugs at an early age.
References
- Baumeister, R. F., and Tice, D. M.
(1986).
Psychological Perspectives on the Self, Vol. 3.
Chapter How adolescence became the struggle for self: A historical
transformation of psychological development. Lawrence Erlbaum
Associates. Hillsdale, NJ. 183–201 Pages. J. Suls and A. G. Greenwald
(Eds.).
- Twenge, J. M.
(2006).
Generation Me: Why Today’s Young Americans Are More Confident, Assertive, Entitled—And More Miserable Than Ever Before. Free Press. New York.
- Farrington, D. P.
(1995).
Psychosocial Disturbances in Young People: Challenges for Prevention.
Chapter The challenge of teenage antisocial behavior. Cambridge
University Press. New York. 83–130 Pages. M. Rutter and M. E. Rutter
(Eds.).
Adolescence begins with the onset of puberty, a
developmental period in which hormonal changes cause rapid physical alterations in
the body, culminating in sexual maturity. Although the timing varies to some
degree across cultures, the average age range for reaching puberty is between 9 and 14
years for girls and between 10 and 17 years for boys. [1]
Puberty begins when the pituitary gland begins to stimulate production of the male sex
hormone testosterone in boys and the female sex hormones estrogen and progesterone in
girls. The release of these sex hormones triggers the development of the primary sex characteristics, the sex organs
concerned with reproduction. These changes include enlargement of the testicles
and penis in boys and development of the ovaries, uterus, and vagina in girls. Secondary sex characteristics (features that
distinguish the two sexes from each other but are not involved in
reproduction), such as an enlarged Adam’s apple, a deeper voice, and pubic and
underarm hair in boys and growing breasts, widening hips, and pubic and underarm hair in
girls, as shown in the figure below. The enlargement of breasts is usually the first
sign of puberty in girls and, on average, occurs between ages 10 and 12. [1]
Boys typically begin to grow facial hair
between ages 14 and 16, and both boys and girls experience a rapid growth spurt during
this stage. The growth spurt usually occurs earlier for girls than for boys, and some
boys continue to grow into their 20s.
A major milestone of puberty for girls is menarche, the first menstrual period, typically experienced at around 12
or 13 years of age. [2]
The age of menarche varies substantially
and is determined by genetics, as well as by diet and lifestyle, since a certain amount
of body fat is needed to attain menarche. Girls who are very slim, who engage in
strenuous athletic activities, or who are malnourished may experience delayed menarche.
Even after menstruation begins, girls whose level of body fat drops below the critical
level may stop having their periods. A less obvious but equally important reproductive
milestone for boys is spermarche, which is the
beginning of sperm development in boys' testicles. The sequence of events for
puberty is more predictable than the age at which they occur. Some girls may begin to
grow pubic hair at age 10 but not attain menarche until age 15. In boys, facial hair may
not appear until 10 years after the initial onset of puberty.
The timing of puberty in both boys and girls can have significant psychological
consequences. Boys who mature early attain some social advantages because they are
taller and stronger and, therefore, often more popular. [3]
At the same time,
however, early-maturing boys are at greater risk for delinquency and are more likely
than their peers to engage in antisocial behaviors, including drug and alcohol use,
truancy, and precocious sexual activity. Girls who mature early may find their maturity
stressful, particularly if they experience teasing or sexual harassment. [4] [5]
Early-maturing girls are also more likely than their peers to have emotional problems, a
lower self-image, and higher rates of depression, anxiety, and disordered eating than their peers. [6]
References
- Marshall, W. A., and Tanner, J. M.
(1986).
Human Growth: A Comprehensive Treatise. Chapter Puberty. Plenum Press. New York. Edition 2. 171–209 Pages. F. Falkner and J. M. Tanner (Eds.).
- Anderson, S. E., Dannal, G. E., and Must,
A.
(2003).
"Relative weight and race influence average age at menarche:
Results from two nationally representative surveys of U.S. girls studied
25 years apart." Pediatrics. Volume 111. Number 4. 844–850 Pages.
- Lynne, S. D., Graber, J. A., Nichols, T. R.,
Brooks-Gunn, J., and Botvin, G. J.
(2007).
"Links between pubertal timing, peer influences, and externalizing
behaviors among urban students followed through middle school." Journal
of Adolescent Health. Volume 40. Number 2. 181.e7–181.e13 Pages.
- Mendle, J., Turkheimer, E., and Emery, R.
E.
(2007).
"Detrimental psychological outcomes associated with early pubertal
timing in adolescent girls." Developmental Review. Volume 27. Number 2.
151–171 Pages.
- Pescovitz, O. H., and Walvoord, E. C.
(2007).
When Puberty Is Precocious: Scientific and Clinical Aspects. Humana Press. Totowa, NJ.
- Ge, X., Conger, R. D., and Elder, G. H., Jr.
(1996).
"Coming of age too early: Pubertal influences on girls’
vulnerability to psychological distress." Child Development. Volume 67.
Number 6. 3386–3400 Pages.
Although the most rapid cognitive changes occur during childhood, the brain continues to
develop throughout adolescence and even into the 20s. [1]
During adolescence, the brain
continues to form new neural connections but also casts off unused neurons and
connections. [2]
As teenagers mature, the prefrontal
cortex, the area of the brain responsible for reasoning,
planning, and problem solving, also continues to develop. [3]
Myelin, the fatty
tissue that forms around axons and neurons and helps speed transmissions between
different regions of the brain, also continues to grow. [4]
Adolescents often seem to act impulsively rather than thoughtfully, perhaps in part
because the development of the prefrontal cortex is generally slower than the
development of the emotional parts of the brain, including the limbic system. [2] Furthermore, the hormonal
surge associated with puberty, which primarily influences emotional responses, may
create strong emotions and lead to impulsive behavior. It is hypothesized that
adolescents may engage in risky behavior, such as smoking, drug use, dangerous driving,
and unprotected sex, in part because they have not yet fully acquired the mental ability
to curb impulsive behavior or to make entirely rational judgments. [5]
On the positive side, adolescents are gaining new cognitive abilities that differentiate
them from children. Recall Piaget’s cognitive development stages. During puberty,
adolescents begin to develop formal operational thinking—the ability to think systematically and use scientific
reasoning. They also gain the ability to think and reason about abstract concepts—something they were
unable to do as children.
The new cognitive abilities attained during adolescence may also give rise to new
feelings of egocentrism, in which adolescents
believe that they can do anything and that they know better than anyone else,
including their parents. [6]
Teenagers are likely to be highly self-conscious,
often creating an imaginary audience in which they feel that everyone is constantly watching them. [7]
Because teens think so much
about themselves, they mistakenly believe that others must be thinking about them,
too. [8] It is no wonder that
everything a teen’s parents do suddenly feels embarrassing to them when they are in
public.
References
- Weinberger, D. R., Elvevåg, B., and Giedd, J. N.
(2005).
The adolescent brain: A work in progress. National Campaign to Prevent Teen Pregnancy. Retrieved from
http://www.thenationalcampaign.org/resources/pdf/BRAIN.pdf.
- Blakemore, S. J.
(2008).
"Development of the social brain during adolescence." Quarterly
Journal of Experimental Psychology. Volume 61. Number 1. 40–49 Pages.
- Goldberg, E.
(2001).
The Executive Brain: Frontal Lobes and the Civilized Mind. Oxford University Press. New York.
- Rapoport, J. L., Giedd, J. N.,
Blumenthal, J., Hamburger, S., Jeffries,
N., Fernandez, T., et al.
(1999).
"Progressive cortical change during adolescence in childhood-onset
schizophrenia: A longitudinal magnetic resonance
imaging study." Archives of General Psychiatry. Volume 56. Number 7.
649–654 Pages.
- Steinberg, L.
(2007).
"Risk taking in adolescence: New perspectives from brain and behavioral
science." Current Directions in Psychological Science. Volume 16. Number 2. 55–59 Pages.
- Goldberg, E.
(1978).
The Child’s Reality: Three Developmental Themes. Lawrence Erlbaum Associates. Hillsdale, NJ.
- Goossens, L., Beyers, W., Emmen, M., and
van Aken, M.
(2002).
"The imaginary audience and personal fable: Factor analyses and
concurrent
validity of the “new look” measures." Journal of
Research on Adolescence. Volume 12. Number 2. 193–215 Pages.
- Rycek, R. F., Stuhr, S. L., Mcdermott, J., Benker, J., and Swartz, M.
D.
(1998).
"Adolescent egocentrism and cognitive functioning during late
adolescence." Adolescence. Volume 33. Number 132. 746–750 Pages.
Some of the most important changes that occur during adolescence involve the further
development of self-concept and the development of new attachments. Whereas young
children are most strongly attached to their parents, the important attachments of
adolescents move increasingly away from parents and toward
peers. [1] As a result, parents’ influence diminishes at this
stage.
According to Erikson (refer to the table "Erikson’s Framework for Development"), the main social task of the adolescent is the search for a unique
identity—the ability to answer the question, Who am I? In the search for identity, the
adolescent may experience role confusion in which he or she is balancing or choosing
among identities, taking on negative or undesirable identities, or temporarily giving up
looking for an identity altogether if things are not going well. Erikson [2]
believed that it was normative for adolescents to “try
on” different roles to determine what their identity would become. He termed
this search for identity role experimentation.
One approach to assessing identity development was proposed by James
Marcia. [3] In his approach, adolescents are asked
questions regarding their exploration of and commitment to issues related to occupation,
politics, religion, and sexual behavior. Their responses enable researchers to classify
the adolescents into one of four identity categories shown in the following table.
| James Marcia’s Stages of Identity Development |
|---|
| From Flat World Knowledge, Introduction to Psychology, v1.0; adapted from Marcia, J. E. (1980). Identity in adolescence. In J. Adelson (Ed.), Handbook of Adolescent Psychology, Vol. 5, pp. 145–160, New York: Wiley. |
| Status |
Description |
| Identity-diffusion status |
The individual does not have firm commitments regarding the issues in question
and is not making progress toward them. |
| Foreclosure status |
The individual has not engaged in any identity experimentation and has
established an identity based on the choices or values of others. |
| Moratorium status |
The individual is exploring various choices but has not yet made a clear
commitment to any of them. |
| Identity-achievement status |
The individual has attained a coherent and committed identity based on personal
decisions. |
|
Studies assessing how teens pass through Marcia’s stages show that although most teens
eventually succeed in developing a stable identity, the path to it is not always easy
and many routes can be taken. Some teens may simply adopt the beliefs
of their parents or the first role that is offered to them, perhaps at the expense
of searching for other, more promising possibilities (foreclosure status). Other teens may spend years trying on
different possible identities (moratorium status) before finally choosing one.
To help them work through the process of developing an identity, teenagers may try out
different identities in different social situations. They may maintain one identity at
home and a different persona when they are with their peers. Eventually, most teenagers integrate the different possibilities into a single
self-concept and a comfortable sense of identity (identity-achievement status).
For teenagers, the peer group provides valuable information about self-concept. For
instance, in response to the question What were you like as a
teenager? (e.g., cool, nerdy, awkward?), posed on the website Answerbag, one
teenager replied in this way:
I’m still a teenager now, but from 8th–9th grade I didn’t really know
what I wanted at all. I was smart, so I hung out with the nerdy kids. I still do; my
friends mean the world to me. But in the middle of 8th I started hanging out with whom
you may call the 'cool' kids...and I also hung out with some stoners, just for variety.
I pierced various parts of my body and kept my grades up. Now, I’m just trying to find
who I am. I’m even doing my sophomore year in China so I can get a better view of what I
want. [4]
Responses like this one demonstrate the extent to which adolescents are developing their
self-concepts and self-identities and how they rely on peers to help them do that. This
is also an example of Erikson’s idea of role experimentation. The writer here is trying
out several (perhaps conflicting) identities, and the identities any teen experiments
with are defined by the group the person chooses to be a part of. The friendship groups
(cliques, crowds, or gangs) that are such an important part of the adolescent experience
allow young adults to try out different identities, and these groups provide a sense of
belonging and acceptance. [5] A big part of
what adolescents are learning is social identity, the part of their self-concept that is
derived from group memberships. Adolescents define their social identities according to
how they are similar to and how they differ from others, finding meaning in the sports,
religious, school, gender, and ethnic categories they belong to.
It’s important to remember that, unlike Piaget's and Erikson's, Marcia’s theory is not a
stage theory, so Marcia uses the term status to indicate which
of the four options characterizes someone. Adolescents don’t progress from one status to
another in a sequential manner. For example, not all adolescents explore different
identities, and some do not make a commitment to an identity. The way to determine the
status of an adolescent is to determine (a) whether he or she has explored meaningful
alternatives to an identity question, and (b) whether he or she has made a commitment to
an identity. Based on these questions, the following table shows which status best
describes an adolescent's current level of identity formation:
References
- Harris, J.
(1998).
The Nurture Assumption—Why Children Turn Out the Way They Do. Free Press. New York.
- Erikson, E. H.
(1956).
"The problem of ego identity." Journal of the American Psychoanalytic Association. Volume 4. Number 1. 56–121 Pages.
- Marcia, J. E.
(1980).
Handbook of Adolescent Psychology, Vol. 5. Chapter Identity in adolescence. Wiley. New York. 145–160 Pages. J. Adelson (Ed.).
- Answerbag
(2007, March 20).
What were you like as a teenager? (e.g., cool, nerdy, awkward?). Retrieved from http://www.answerbag.com/q_view/171753.
- Rubin, K. H., Bukowski, W. M., and Parker, J. G.
(2006).
Handbook of Child Psychology: Social, Emotional, and Personality Development, Vol. 3.
Chapter Peer interactions, relationships, and groups. Wiley. Hoboken,
NJ. Edition 6. 571–645 Pages. N. Eisenberg, W. Damon, and R. M. Lerner
(Eds.).
The independence that comes with adolescence requires independent thinking as well as the
development of morality—standards of behavior that are generally accepted within a
culture to be right or proper. Just as Piaget believed that children’s cognitive
development follows specific patterns, Lawrence Kohlberg [1] argued that
children learn their moral values through active thinking and reasoning and that the
development of moral reasoning progresses through a series of levels and stages and
continues to develop throughout an individual’s life. To develop his theory, Kohlberg
posed hypothetical moral dilemmas to children, adolescents, and adults and then matched
each person’s response to a specific level and stage of moral development. One of
Kohlberg’s classic hypothetical moral dilemmas is the following:
Heinz’s wife is dying of cancer, and only one drug can save her. The
only place to get the drug is at the store of a pharmacist who is known to
overcharge people for drugs. The man can only pay $1,000, but the pharmacist wants
$2,000 and refuses to sell it to him for less or to let him pay later. Desperate,
the man later breaks into the pharmacy and steals the medicine. Should he have done
that? Was it right or wrong? Why? (p.
200)
learn by doing
A moral dilemma is a mental conflict involving choice, wherein each potential
course of action breaches an individual's moral principles or cultural
standards. The Heinz dilemma described above presents several such conflicts for
the husband.
References
- Kohlberg, L.
(1984).
The Psychology of Moral Development: Essays on Moral Development, Vol. 2. Harper and Row. San Francisco.
As you can see in the following table, Kohlberg concluded, on the basis of their
responses to the moral questions, that as children develop intellectually, they pass
through three stages of moral thinking: the preconventional level,
the conventional level, and the postconventional
level.
| Lawrence Kohlberg’s Stages of Moral Reasoning |
|---|
| Age |
Moral Stage |
Description |
| Young children |
Preconventional morality |
Until about age 9, children focus on self-interest. At this stage, punishment is
avoided and rewards are sought. A person at this level will argue, “The man
shouldn’t steal the drug because he may get caught and go to jail.” |
| Older children, adolescents, most adults |
Conventional morality |
By early adolescence, the child begins to care about how situational outcomes
impact others and wants to please and be accepted. At this developmental phase,
people are able to value the good that can be derived from holding to social
norms in the form of laws or less formalized rules. For example, a person at
this level may say, “He should not steal the drug because everyone will see him
as a thief, and his wife, who needs the drug, wouldn’t want to be cured because
of thievery,” or “No matter what, he should obey the law because stealing is a
crime.” |
| Many adults |
Postconventional morality |
At this stage, individuals employ abstract reasoning to justify behaviors. Moral
behavior is based on self-chosen ethical principles that are generally
comprehensive and universal, such as justice, dignity, and equality. Someone
with self-chosen principles may say, “The man should steal the drug to cure his
wife and then tell the authorities that he has done so. He may have to pay a
penalty, but at least he has saved a human life.” |
|
learn by doing
Each of the following persons are presented the Heinz dilemma and asked if Heinz
should have stolen the drug for his wife and why. Read each person's response,
and then choose the answer that best reflects his or her level of moral
development.
Although research supports Kohlberg’s idea that moral reasoning changes from an
early emphasis on punishment and social rules and regulations to an emphasis on more
general ethical principles, as with Piaget’s approach, Kohlberg’s stage model is
probably too simple. For one, children may use higher levels of reasoning for some types
of problems but revert to lower levels when doing so is more consistent with their goals
or beliefs. [1] Second, it has been argued that the stage model is
particularly appropriate for Western, rather than non-Western, samples in which
allegiance to social norms (such as respect for authority) may be particularly
important. [2] And there is frequently little correlation between how
children score on the moral stages and how they behave in real life.
Perhaps the most important
critique of Kohlberg’s theory is that it may describe the moral development of
boys better than it describes that of girls. Carol Gilligan [3] has
argued that, because of differences in their socialization, males tend to value
principles of justice and rights, whereas females value caring for and helping
others. Although there is little evidence that boys and girls score differently
on Kohlberg’s stages of moral development. [4] it is true that
girls and women tend to focus more on issues of caring, helping, and connecting
with others than do boys and men. [5] If you don’t
believe this, ask yourself when you last got a thank-you note from a man.
References
- Rest, J.
(1979).
Development in Judging Moral Issues. University of Minnesota Press. Minneapolis.
- Haidt, J.
(2001).
"The emotional dog and its rational tail: A social intuitionist
approach to moral judgment." Psychological Review. Volume 108. Number 4.
814–834 Pages.
- Gilligan, C.
(1982).
In a Different Voice: Psychological Theory and Women’s Development. Harvard University Press. Cambridge, MA.
- Turiel, E.
(1998).
Handbook of Child Psychology: Socialization, Vol. 3. Chapter Peer interactions, relationships, and groups. Wiley. New York. Edition 5. 863–932 Pages. W. Damon (Ed.).
- Jaffee, S., and Hyde, J. S.
(2000).
"Gender differences in moral orientation: A meta-analysis." Psychological Bulletin. Volume 126. Number 5. 703–726 Pages.
Until the 1970s, psychologists tended to treat adulthood as a single developmental stage
with few or no distinctions made among the various periods we pass through between
adolescence and death. Present-day psychologists realize, however, that physical,
cognitive, and emotional responses continue to develop throughout life, with
corresponding changes in our social needs and desires. Each of the three stages of
adulthood—early, middle, and late—has its own physical, cognitive, and social
challenges.
In this section, we consider the development of our cognitive and physical aspects that
occur during early adulthood and middle adulthood—roughly the ages between 25 and 45 and
between 45 and 65 respectively. These stages represent a long period of time—longer, in
fact, than any of the other developmental stages—and the bulk of our lives is spent in
them. These are also the periods in which most of us make our most substantial
contributions to society, by meeting two of Erik Erikson’s life challenges: Intimacy
versus isolation is the conflict we face in learning to give and receive love in a
close, long-term relationship. Generativity versus stagnationis the conflict we face in
developing an interest in guiding the development of the next generation, often by
becoming parents.
Remember that the stage in Erikson’s framework that covers the period of adolescence is
identity versus role confusion. This period involves a psychological movement away from
the family as the center of one’s life and establishing one’s sense of self as well as
life goals and interests. Ideally, by the time a person moves into the adult years, he
or she has an increasingly stable identity and a new challenge, intimacy versus
isolation, turns the individual’s focus from the self to the social world. During this
period, young people become increasingly invested in intimate personal relationships and
more serious about developing personal and romantic relationships that will influence
the course of their adult lives. Marriage and starting a family may be put off or
rejected as life goals, but mature relationships lead to the experience of intimacy, or,
if such relationships fail to materialize, the person experiences isolation and the
doubts and difficulties that can be produced by an inadequate social base.
In later adulthood, which, in Erikson’s scheme, covers the period from the mid-20s to the
mid-60s—the majority of one’s life—people concern themselves with their life’s work.
This is the period described by the contrast of generativity versus stagnation.
Generativity or productivity is largely self-defined in terms of specific
accomplishments, but to be generative, an individual must have goals that are motivating
and must succeed in achieving some of those goals. The failure of generativity,
stagnation, can be due to a failure to define motivating goals or a failure to act
consistently in ways to achieve them.
learn by doing
Consider the following people and descriptions of where they are in their lives:
-
Joe has been stuck in a boring bureaucratic job
for the past decade, and he has lost confidence in his ability to
produce something really special with his life.
-
Jill has enjoyed casual friendships, but now she realizes
she wants a serious relationship and, hopefully in the not-too-distant
future, to start a family.
-
David doesn’t care much about school or any other
activities that seem to motivate other students at school. He has always
been good at video games, and the guys he hangs out with are also
gamers.
-
Jamal got an engineering degree in college, but during a
year working with Teach for America, he discovers that teaching math to high
school students makes him creative and excited about going to work.
-
Amanda started middle school feeling unhappy with
herself and her life, but she has discovered that she loves performing
in theater and musical events, and her friends are now the students who
are involved in these activities at school.
-
LaShana is envious of some of her friends who have
great boyfriends and fun lives. She starts avoiding them and spends
most of her time studying, hoping she will get into a good college far
away from all these boring people.
Compared with the other stages, the physical and cognitive changes that
occur in the stages of early and middle adulthood are less dramatic. As individuals pass
into their 30s and 40s, their recovery from muscular strain becomes more prolonged, and
their sensory abilities may become somewhat diminished, at least when compared with
their prime years, during the teens and early 20s. [1] Visual
acuity diminishes somewhat, and many people in their late 30s and early 40s begin to
notice that their eyes are changing and they need eyeglasses. Adults in their 30s and
40s may also begin to suffer some hearing loss because of damage to the hair cells (cilia) in the inner ear. [2]
And it is during middle adulthood that
many people first begin to suffer from ailments such as high cholesterol and high blood
pressure as well as low bone density. [3] Corresponding to
changes in our physical abilities, our cognitive and sensory abilities also seem to show
some, but not dramatic, decline during this stage.
Menopause
The stages of both early and middle adulthood bring about a gradual decline in
fertility, particularly for women. Eventually, women experience menopause, the cessation of the menstrual
cycle, which usually occurs at around age 50. Menopause occurs because
of the gradual decrease in the production of the female sex hormones estrogen
and progesterone, which slows the production and release of eggs into the
uterus. Women whose menstrual cycles have stopped for 12 consecutive months are
considered to have entered menopause. [4] A set of
symptoms (hot flashes, insomnia, mood swings) due to hormonal changes prior to
menopause are often referred to perimenopause.
Researchers have found that women’s responses to menopause are both social and
physical and that they vary substantially across both individuals and cultures.
Among individuals, some women may react more negatively than others to
menopause, worrying that they have lost their femininity and that their final
chance to bear children is over, whereas other women may regard menopause more
positively, focusing on the new freedom from menstrual discomfort and unwanted
pregnancy. In Western cultures such as in the United States, women are likely to
see menopause as a challenging and potentially negative event, whereas in India,
where older women enjoy more social privileges than do younger ones, menopause
is more positively regarded. [5]
Menopause may have evolutionary benefits. Infants have better chances of survival
when their mothers are younger and have more energy to care for them, and the
presence of older women who do not have children of their own to care for (but
who can help out with raising grandchildren) can be beneficial to the family
group. Also consistent with the idea of an evolutionary benefit of menopause is
that the decline in fertility occurs primarily for women, who do most of the
child care and who need the energy of youth to accomplish it. If older women
were able to have children, they might not be as able to effectively care for
them.
Most men never completely lose their fertility, but they do experience a gradual decrease in
testosterone levels, sperm count, and speed of erection and ejaculation.
Social Changes in Early and Middle Adulthood
Perhaps one of the major markers of adulthood is the ability to create an
effective and independent life. Whereas children and adolescents are generally
supported by parents, adults must make their own living and must start their own
families. Furthermore, the needs of adults are different from those of younger
persons.
Although the timing of the major life events that occur in early and middle adulthood
vary substantially across individuals, they nevertheless tend to follow a
general sequence, known as a social clock. The social
clock is the culturally preferred “right time” for
major life events, such as moving out of the childhood house, getting a
job, getting married, having children, and owning your own home. People who do
not appear to be following the norms of the social clock (e.g., young adults who
still live with their parents, individuals who never marry, and couples who
choose not to have children) may be seen as unusual or deviant, and they may be
stigmatized by
others. [6] [7]
Although, on average, they are doing it later than they did even 20 or 30 years ago,
most people do eventually marry. Marriage is beneficial to the partners in terms
of both mental health and physical health. People who are married report greater
life satisfaction than those who are not married and also suffer fewer health
problems. [8] [9]
Divorce is more common now than it was 50 years ago. In 2003, almost half of
marriages in the United States ended in divorce, [10]
although about three quarters of people
who divorce will remarry. Most divorces occur for couples in their 20s, because
younger people are frequently not mature enough to make good marriage choices or
to make marriages last. Marriages are more successful for older adults and for
those with more
education. [11]
Parenthood also involves a major and long-lasting commitment, one that can cause
substantial stress on the parents. The time and finances invested in children
create stress, which frequently results in decreased marital
satisfaction. [12] This decline is
especially true for women, who usually bear the larger part of the burden of
raising the children and taking care of the house, despite that they
increasingly also work and have careers.
Despite the challenges of early and middle adulthood, the majority of middle-aged
adults are not unhappy. These years are often very satisfying, as families have
been established, careers have been entered into, and some percentage of life
goals has been realized. [13]
References
- Panno, J.
(2004).
Aging: Theories and Potential Therapies. Facts on File Publishers. New York.
- Lacher-Fougëre, S., and Demany, L.
(2005).
"Consequences of cochlear damage for the detection of interaural
phase differences." Journal of the Acoustical Society of America. Volume
118. Number 4. 2519–2526 Pages.
- Shelton, H. M.
(2006).
High Blood Pressure. Kessinger Publishers. Whitefish, MT.
- Minkin, M. J., and Wright, C. V.
(2004).
A Woman’s Guide to Monepause and Perimenopause. Yale University Press. New Haven, CT.
- Avis, N. E., and Crawford, S.
(2008).
"Cultural differences in symptoms and attitudes toward menopause."
Menopause Management. Volume 17. Number 3. 8–13 Pages.
- DePaulo, B. M.
(2006).
Singled Out: How Singles Are Stereotyped, Stigmatized and Ignored, and Still Live Happily Ever After. St. Martin’s Press. New York.
- Rook, K. S., Catalano, R. C., and Dooley, D.
(1989).
"The timing of major life events: Effects of departing from the
social clock." American Journal of Community Psychology. Volume 17.
Number 2. 223–258 Pages.
- Gallagher, M., and Waite, L. J.
(2001).
The Case for Marriage: Why Married People Are Happier, Healthier, and Better Off Financially. Random House. New York.
- Liu, H., and Umberson, D.
(2008).
"The times they are a changin’: Marital status and health
differentials from 1972 to 2003." Journal of Health and Social Behavior.
Volume 49. Number 3. 239–253 Pages.
- Bureau of the Census
(2007).
Statistical Abstract of the United States 2006. U.S. Government Printing Office. Washington, DC.
- Goodwin, P. Y., Mosher, W. D., Chandra A.
(2010).
"Marriage and cohabitation in the United States: A statistical
portrait based on Cycle 6 (2002) of the National Survey of Family
Growth." Vital Health Statistics. Volume 23. Number 28. 1–45 Pages.
- Twenge, J., Campbell, W., and Foster, C.
(2003).
"Parenthood and marital satisfaction: A meta-analytic review."
Journal of Marriage and Family. Volume 65. Number 3. 574–583 Pages.
- Eid, M., and Larsen, R. J. (Eds.)
(2008).
The Science of Subjective Well-being. Guilford Press. New York.
We have seen that, over the course of their lives, most individuals are able to develop
secure attachments; reason cognitively, socially and morally; and create families and
find appropriate careers. Eventually, however, as people enter into their 60s and
beyond, the aging process leads to faster changes in our physical, cognitive, and social
capabilities and needs, and life begins to come to its natural conclusion, resulting in
the final life stage, beginning in the 60s, known as late adulthood.
Despite that the body and mind are slowing, most older adults nevertheless maintain an
active lifestyle, remain as happy as or are happier than when they were younger, and
increasingly value their social connections with family and friends. [1]
Kennedy, Mather, and Carstensen [2]
found that people’s memories of their lives became more positive with
age, and Myers and Diener [3] found that older adults tended to speak
more positively about events in their lives, particularly their relationships with
friends and family, than did younger adults.
Cognitive Changes during Aging
The changes associated with aging do not affect everyone in the same way, and
they do not necessarily interfere with a healthy life. Former Beatles drummer
Ringo Starr celebrated his 70th birthday in 2010 by playing at Radio City Music
Hall, and Rolling Stones singer Mick Jagger (who once supposedly said, “I’d
rather be dead than singing ‘Satisfaction’ at 45”) continues to perform as he
pushes 70. The golfer Tom Watson almost won the 2010 British Open golf
tournament at the age of 59, playing against competitors in their 20s and 30s.
And people such as the financier Warren Buffett, U.S. Senator Frank Lautenberg,
and actress Betty White, each in their 80s, all enjoy highly productive and
energetic lives.
Researchers are beginning to better understand the factors that allow some people
to age better than others. For one, research has found that the people who are
best able to adjust well to changing situations early in life are also able to
better adjust later in life. [4] [5]
Perceptions
also matter. People who believe that the elderly are sick, vulnerable, and
grumpy often act according to such beliefs, [6] and
Levy, Slade, Kunkel, and Kasl [7] found that the elderly who had
more positive perceptions about aging also lived longer.
In one important study concerning the role of expectations on memory, Becca Levy
and Ellen Langer [8] found that, although young American and
Chinese students performed equally well on cognitive tasks, older Americans
performed significantly more poorly on those tasks than did their Chinese
counterparts. Furthermore, this difference was explained by beliefs about
aging—in both cultures, the older adults who believed memory declines with age
also showed more actual memory decline than did the older adults who believed
memory does not decline with age. In addition, more older Americans than older
Chinese believed that memory declines with age, and as you can see in the
following figure, older Americans performed more poorly on the memory tasks.
Whereas it was once believed that almost all older adults suffered from a
generalized memory loss, research now indicates that healthy older adults
actually experience only some particular types of memory deficits, while other
types of memory remain relatively intact or may even improve with age. Older
adults do seem to process information more slowly—it may take them longer to
evaluate information and to understand language, and it takes them longer, on
average, than it does younger people, to recall a word they know, even though
they are perfectly able to recognize the word once they see
it. [9] Older adults also
have more difficulty inhibiting and controlling their
attention, [10] making
them, for example, more likely to talk about topics that are not relevant to the
topic at hand when conversing. [11]
But slower processing and less accurate executive control does not always mean
loss of memory or intelligence. Perhaps the elderly are slower in part because
they simply have more knowledge. Indeed, older adults have more crystallized intelligence—that is, general
knowledge about the world, as reflected in semantic knowledge, vocabulary,
and language. As a result, adults generally outperform younger people
on measures of history, geography, and even on crossword puzzles, where this
information is useful. [12] This superior knowledge
combined with a slower and more complete processing style and a more
sophisticated understanding of the workings of the world around them, gives the
elderly the advantage of “wisdom” over the advantages of fluid
intelligence—the ability to think and acquire
information quickly and abstractly—which favor the
young. [13] [14]
The differential changes in crystallized versus fluid intelligence help explain
why the elderly do not necessarily show poorer performance on tasks that also
require experience (i.e., crystallized intelligence), although they show poorer
memory overall. A young chess player may think more quickly, for instance, but a
more experienced chess player has more knowledge to draw on. Older adults are
also more effective at understanding the nuances of social interactions than
younger adults are, in part because they have more experience in
relationships. [15]
learn by doing
Understanding the difference between crystallized and fluid intelligence
can help us understand cognitive changes as we age.
References
- Angner, E., Ray, M. N., Saag, K. G., and Allison,
J. J.
(2009).
"Health and happiness among older adults: A community-based study."
Journal of Health Psychology. Volume 14. Number 4. 503–512 Pages.
- Kennedy, Q., Mather, M., and Carstensen,
L. L.
(2004).
"The role of motivation in the age-related positivity effect in
autobiographical memory." Psychological Science. Volume 15. Number 3.
208–214 Pages.
- Myers, D. G., and Diener, E.
(1996).
"The pursuit of happiness." Scientific American. Volume 274. Number 5. 70–72 Pages.
- Rubin, L.
(2007).
60 on Up: The Truth about Aging in America. Beacon Press. Boston.
- Sroufe, L. A., Collins, W. A., Egeland, B., and Carlson, E. A.
(2009).
The Development of the Person: The Minnesota Study of Risk and Adaptation from Birth to Adulthood. Guilford Press. New York.
- Nemmers, T. M.
(2005).
"The influence of ageism and ageist stereotypes on the elderly."
Physical and Occupational Therapy in Geriatrics. Volume 22. Number 4.
11–20 Pages.
- Levy, B. R., Slade, M. D., Kunkel, S. R., and
Kasl, S. V.
(2002).
"Longevity increased by positive self-perceptions of aging."
Journal of Personality and Social Psychology. Volume 83. Number 2.
261–270 Pages.
- Levy, B., and Langer, E.
(1994).
"Aging free from negative stereotypes: Successful memory in China
among the American deaf." Journal of Personality and Social Psychology.
Volume 66. Number 6. 989–997 Pages.
- Burke, D. M., Shafto, M. A., Craik, F. I. M., and Salthouse, T. A.
(2008).
The Handbook of Aging and Cognition. Chapter Language and aging. Wiley. New York. Edition 3. 373–443 Pages. F. I. M. Craik and T. A. Salthouse (Eds.).
- Persad, C. C., Abeles, N., Zacks, R. T.,
and Denburg, N. L.
(2002).
"Inhibitory changes after age 60 and the relationship to measures
of attention and memory." Journals of Gerontology: Series B:
Psychological Sciences and Social Sciences. Volume 57B. Number 3.
P223–P232 Pages.
- Pushkar, D., Basevitz, P., Arbuckle, T., Nohara-LeClair, M., Lapidus, S., and Peled, M.
(2000).
"Social behavior and off-target verbosity in elderly people." Psychology and Aging. Volume 15. Number 2. 361–374 Pages.
- Salthouse, T. A.
(2004).
"What and when of cognitive aging." Current Directions in Psychological Science. Volume 13. Number 4. 140–144 Pages.
- Baltes, P. B., Staudinger, U. M., and
Lindenberger, U.
(1999).
"Life-span psychology: Theory and application to intellectual
functioning." Annual Review of Psychology. Volume 50. Number 2. 471–506
Pages.
- Scheibe, S., Kunzmann, U., and Baltes, P. B.
(2009).
Oxford Handbook of Positive Psychology.
Chapter New territories of positive life-span development: Wisdom and
life longings. Oxford University Press. New York. Edition 2. 171–183
Pages. S. J. E. Lopez and C. R. E. Snyder (Eds.).
- Blanchard-Fields, F.,
Mienaltowski, A., and Seay, R. B.
(2007).
"Age differences in everyday problem-solving effectiveness: Older
adults select more effective strategies for interpersonal problems."
Journals of Gerontology: Series B: Psychological Sciences and Social
Sciences. Volume 62B. Number 1. P671–P64 Pages.
Some older adults suffer from biologically based cognitive impairments in which the brain
is so adversely affected by aging that it becomes very difficult for the person to
continue to function effectively. Dementia is a
progressive neurological disease that includes loss of cognitive abilities
significant enough to interfere with everyday behaviors, and Alzheimer’s disease is a form of dementia that, over a
period of years, leads to a loss of emotions, cognitions, and physical functioning,
and that is ultimately fatal. Dementia and Alzheimer’s disease are most likely
to be observed in individuals who are 65 and older, and the likelihood of developing
Alzheimer’s disease doubles about every 5 years after age 65. After age 85, the risk
reaches nearly 8% per year. [1] Dementia and Alzheimer’s
disease both produce a gradual decline in functioning of the brain cells that produce
the neurotransmitter acetylcholine. Without this neurotransmitter, neurons are unable to
communicate, leaving the brain less and less functional.
Dementia and Alzheimer’s disease are in part heritable, but increasing evidence suggests
that environment also plays a role. And current research is helping us understand the
things that older adults can do to help them slow down or prevent the negative cognitive
outcomes of aging, including dementia and Alzheimer’s disease. [2]
Older adults who
continue to keep their minds active by engaging in cognitive activities, such as
reading, playing musical instruments, attending lectures, or doing crossword puzzles;
who maintain social interactions with others; and who keep themselves physically fit
have a greater chance of maintaining their mental acuity than those who do
not. [3] [4] In short, although
physical illnesses may happen to anyone, the more people keep their brains active and
the more they maintain a healthy and active lifestyle, the more healthy their brains
will remain. [5]
References
- Hebert, L. E., Scherr, P. A., Beckett, L. A.,
Albert, M. S., Pilgrim, D. M., Chown, M. J., et al.
(1995).
"Age-specific incidence of Alzheimer’s disease in a community
population." Journals of the American Medical Association. Volume 273.
Number 17. 1354–1359 Pages.
- Pushkar, D., Bukowski, W. M., Schwartzman, A. E., Stack, D. M., and White, D. R.
(2007).
Responding to the Challenges of late Life: Strategies for Maintaining and Enhancing Competence. Springer. New York.
- Cherkas, L. F., Hunkin, J. L., Kato, B.
S., Richards, J. B., Gardner, J. P., Surdulescu, G. L., et al.
(2008).
"The association between physical activity in leisure time and
leukocyte telomere length." Archives of Internal Medicine. Volume 168.
Number 2. 154–158 Pages.
- Verghese, J., Lipton, R., Katz, M. J.,
Hall, C. B., Derby, C. A., et al.
(2003).
"Leisure activities and the risk of dementia in the elderly." New
England Journal of Medicine. Volume 348. Number 25. 2508–2516 Pages.
- Ertel, K. A., Glymour, M. M., and Berkman,
L. F.
(2008).
"Effects of social integration on preserving memory function in a
nationally representative U.S. elderly population." American Journal of
Public Health. Volume 98. Number 7. 1215–1220 Pages.
Because of increased life expectancy in the 21st century, elderly people can expect to
spend approximately a quarter of their lives in retirement. Leaving a career is a major
life change and can be a time when people experience anxiety, depression, and other
negative changes in self-concept and self-identity. At the same time, retirement may
also serve as an opportunity for a positive transition from work and career roles to
stronger family and community member roles, and the latter may have a variety of
positive outcomes for the individual. Retirement may be a relief for people who have
worked in boring or physically demanding jobs, particularly if they have other outlets
for stimulation and expressing self-identity.
Psychologist Mo Wang [1] observed the well-being of 2,060 people between
the ages of 51 and 61 over an 8-year period and made the following recommendations to
make the retirement phase a positive one:
- Continue to work part time past retirement to ease into retirement status
slowly.
- Plan for retirement—this is a good idea financially, but also making plans to
incorporate other kinds of work or hobbies into postemployment life makes
sense.
- Retire with someone—if the retiree is still married, it is a good idea to retire at
the same time as a spouse so that the couple can continue to work part time and
follow a retirement plan together.
- Have a happy marriage—people with marital problems tend to find retirement more
stressful because they do not have a positive home life to return to and can no
longer seek refuge in long working hours. Couples who work on their marriages can
make their retirements a lot easier.
- Take care of physical and financial health—a sound financial plan and good physical
health can ensure a healthy, peaceful retirement.
- Retire early from a stressful job—people who stay in stressful jobs for fear that
they will lose their pensions or won’t be able to find work somewhere else feel
trapped. Toxic environments can take a severe emotional toll on an employee. Leaving
early from an unsatisfying job may make retirement a relief.
- Retire “on time”—retiring too early or too late can cause people to feel “out of
sync” or to feel they have not achieved their goals.
Whereas these seven tips are helpful for a smooth transition to retirement, Wang also
notes that people tend to be adaptable and that no matter how they do it, retirees will
eventually adjust to their new lifestyles.
References
- Wang, M.
(2007).
"Profiling retirees in the retirement transition and adjustment
process: Examining the longitudinal change patterns of retirees’
psychological well-being." Journal of Applied Psychology. Volume 92.
Number 2. 455–474 Pages.
Living includes dealing with our own and our loved ones’ mortality. In her book On Death and Dying, [1] Elizabeth Kübler-Ross
describes five phases of grief through which people pass in grappling with the knowledge
that they or someone close to them is dying:
-
Denial: “I feel fine.” “This can’t be happening; not to
me.”
-
Anger: “Why me? It’s not fair!” “How can this happen to me?”
“Who is to blame?”
-
Bargaining: “Just let me live to see my children graduate.”
“I’d do anything for a few more years.” “I’d give my life savings if....”
-
Depression: “I’m so sad, why bother with anything?” “I’m going
to die. What’s the point?” “I miss my loved ones—why go on?”
-
Acceptance: “I know my time has come; it’s almost my
time.”
Despite Ross’s popularity, a growing number of critics of her theory argue that her
five-stage sequence is too constraining because attitudes toward death and dying have
been found to vary greatly across cultures and religions, and these variations make the
process of dying different according to culture. [2] As an
example, Japanese Americans restrain their
grief [3] so as not to burden other people with
their pain. By contrast, Jews observe a 7-day, publicly announced mourning period. In
some cultures, the elderly are more likely to be living and coping alone, or perhaps
only with their spouse, whereas in other cultures, such as the Hispanic culture, the
elderly are more likely to be living with their sons and daughters and other relatives,
and this social support may create a better quality of life for
them. [4]
Margaret Stroebe and her colleagues [5] found that although most people
adjust to the loss of a loved one without seeking professional treatment, many have an
increased risk of mortality, particularly within the early weeks and months after the
loss. These researchers also found that people going through the grieving process suffer
more physical and psychological symptoms and illnesses and use more medical
services.
The health of survivors during the end of life is influenced by factors such as
circumstances surrounding the loved one’s death, individual personalities, and ways of
coping. People serving as caretakers to partners or other family members who are ill
frequently experience a great deal of stress themselves, making the dying process even
more stressful. Despite the trauma of the loss of a loved one, people do recover and are
able to continue with effective lives. Grief intervention programs can go a long way in
helping people cope during the bereavement
period. [6]
learn by doing
Consider the following people and descriptions of where they are in Elizabeth
Kübler-Ross’s stages of grief model:
-
Steve: After battling cancer for 4 years, Steve has
come to the realization that he will most likely not survive the illness. He
spends time organizing his financial papers, and he meets with friends for
the last time.
-
Jane: Once Jane heard of her daughter’s pediatrician’s
diagnosis, Jane began to tell the doctor, “I’ll do anything if you can help
my daughter get well.”
-
Jack: When Jack heard others talking about terrorists
attacking New York City, his first reaction was, “No way, that can’t be
happening.”
-
Tom: Tom was very upset that he was diagnosed with
Alzheimer’s disease, stating, “I’ve always been a good person. Why didn’t
this happen to one of those creeps who goes around hurting other people?
It’s people like me who play by the rules who get the short end of the
stick!”
-
Maria: Maria became very sad and withdrawn after
learning that her husband’s cancer was not responding well to treatment.
References
- Kübler-Ross, E.
(1997).
On Death and Dying. Scribner. New York.
- Bonanno, G.
(2009).
The Other Side of Sadness: What the New Science of Bereavement Tells Us about Life after a Loss. Basic Books. New York.
- Corr, C. A., Nabe, C. M., and Corr, D. M.
(2009).
Death and Dying: Life and Living. Wadsworth. Belmont, CA. Edition 6.
- Diaz-Cabello, N.
(2004).
"The Hispanic way of dying: Three families, three perspectives,
three cultures." Illness, Crisis, and Loss. Volume 12. Number 3. 239–255
Pages.
- Stroebe, M. S., Hansson, R. O., Schut, H., and Stroebe, W.
(2008).
Handbook of Bereavement Research and Practice: Advances in Theory and Intervention.
Chapter Bereavement research: Contemporary perspectives. American
Psychological Association. Washington, DC. 3–25 Pages. M. S. Stroebe, R.
O. Hansson, H. Schut, and W. Stroebe (Eds.).
- Neimeyer, R. A., Holland, J. M., Currier, J. M., and Mehta, T.
(2008).
Handbook of Behavioral and Cognitive Therapies with Older Adults.
Chapter Meaning reconstruction in later life: Toward a
cognitive-constructivist approach to grief therapy. Springer-Verlag. New
York. 264–277 Pages. D. Gallagher-Thompson, A. Steffen, and L. Thompson
(Eds.).
He was 3,000 feet up in the air when the sudden loss of power in his
airplane put his life, as well as the lives of 150 other passengers and crew
members, in his hands. Both of the engines on flight 1539 had shut down, and
his options for a safe landing were limited.
Sully kept flying the plane and alerted the control tower to the
situation:
"This is Cactus 1539 . . . hit birds. We lost thrust in both engines. We’re turning back
towards La Guardia."
When the tower gave him the compass setting and runway for a possible
landing, Sullenberger’s extensive experience allowed him to give a calm
response:
"I’m not sure if we can make any runway. . . . Anything in New Jersey?"
Captain Sullenberger was not just any pilot in a crisis, but a former U.S.
Air Force fighter pilot with 40 years of flight experience. He had served as
a flight instructor and the Airline Pilots Association safety chairman.
Training had quickened his mental processes in assessing the threat,
allowing him to maintain what tower operators later called an “eerie calm.”
He knew the capabilities of his plane.
When the tower suggested a runway in New Jersey, Sullenberger calmly
replied:
"We’re unable. We may end up in the Hudson."
Captain Sullenberger and His Plane on the Hudson
 Imagine that you are on a plane that you know is going to crash.
What emotions would you experience, and how would you respond to them?
Would the rush of fear cause you to panic, or could you control your
emotions like Captain Sullenberger did, as he calmly calculated the
heading, position, thrust, and elevation of the plane, and then landed it
on the Hudson River? From Flat World Knowledge, Introduction to Psychology, v1.0. Sullenberger photo courtesy of Ingrid Taylar.
Plane photo courtesy of Greg L.
Imagine that you are on a plane that you know is going to crash.
What emotions would you experience, and how would you respond to them?
Would the rush of fear cause you to panic, or could you control your
emotions like Captain Sullenberger did, as he calmly calculated the
heading, position, thrust, and elevation of the plane, and then landed it
on the Hudson River? From Flat World Knowledge, Introduction to Psychology, v1.0. Sullenberger photo courtesy of Ingrid Taylar.
Plane photo courtesy of Greg L.The last communication from Captain Sullenberger to the tower advised of the
eventual outcome:
"We’re going to be in the Hudson."
He calmly set the plane down on the water. Passengers reported that the landing was like
landing on a rough runway. The crew kept the passengers calm as women, children, and
then the rest of the passengers were evacuated onto the boats of the rescue personnel
that had quickly arrived. Captain Sullenberger then calmly walked the aisle of the plane
to be sure that everyone was out before joining the 150 other rescued
survivors." [1] [2]
Some called it “grace under pressure” and others, the “miracle on the Hudson.” But
psychologists see it as the ultimate in emotion regulation—the ability to control and productively use one’s
emotions.
The topic of this module is affect, defined as the experience of feeling or emotion. Affect is an
essential part of the study of psychology because it plays such an
important role in everyday life. As we will see, affect guides behavior,
helps us make decisions, and has a major impact on our mental and
physical health.
The two fundamental components of affect are emotions and motivation. Both of these
words have the same underlying Latin root, meaning “to move.” In contrast
to cognitive processes that are calm, collected, and frequently rational,
emotions and motivations involve arousal, or our
experiences of the bodily responses created by the sympathetic
division of the autonomic nervous system (ANS). Because they
involve arousal, emotions and motivations are “hot”—they “charge,”
“drive,” or “move” our behavior.
When we experience emotions or strong motivations, we feel the experiences. When we become aroused, the sympathetic
nervous system provides us with energy to respond to our environment. The
liver puts extra sugar into the bloodstream, the heart pumps more blood,
our pupils dilate to help us see better, respiration increases, and we
begin to perspire to cool the body. The stress hormones epinephrine and norepinephrine
are released. We experience these responses as arousal.
An emotion is a mental and
physiological feeling state that directs our attention and guides our
behavior. Whether it is the thrill of a roller-coaster ride that
elicits an unexpected scream, the flush of embarrassment that follows a
public mistake, or the horror of a potential plane crash that creates an
exceptionally brilliant response in a pilot, emotions move our actions.
Emotions normally serve an adaptive role: We care for infants because of
the love we feel for them, we avoid making a left turn onto a crowded
highway because we fear that a speeding truck may hit us, and we are
particularly nice to Mandy because we are feeling guilty that we didn’t
go to her party. But emotions may also be destructive, such as when a
frustrating experience leads us to lash out at others who do not deserve
it.
Motivations are closely related to emotions. A motivation is a driving force that initiates
and directs behavior. Some motivations are biological, such as
the motivation for food, water, and sex. But there are a variety of other
personal and social motivations that can influence behavior, including
the motivations for social approval and acceptance, the motivation to
achieve, and the motivation to take, or to avoid taking, risks. [3]
In each case
we follow our motivations because they are rewarding. As predicted by
basic theories of operant learning, motivations lead us to engage in
particular behaviors because doing so makes us feel good.
References
- Levin, A.
(2009, June 9).
Experience averts tragedy in Hudson landing. USA Today. Retrieved from http://www.usatoday.com/news/nation/2009-06-08-hudson_N.htm.
- National Transportation Safety Board.
(2009, June 9).
Excerpts of Flight 1549 cockpit communications. USA Today. Retrieved from http://www.usatoday.com/news/nation/2009-06-09-hudson-cockpit-transcript_N.htm.
- Morsella, E., Bargh, J. A., and Gollwitzer, P. M.
(2009).
Oxford Handbook of Human Action. Oxford University Press. New York.
We begin this module by considering the role of affect on behavior, discussing the most
important psychological theories of emotions. Then we will consider how emotions
influence our mental and physical health. We will discuss how the experience of
long-term stress causes illness, and then turn to research on positive thinking and what
has been learned about the beneficial health effects of more positive emotions. Finally,
we will review some of the most important human motivations, including the behaviors of
eating and sex. The importance of this unit is not only in helping you gain an
understanding the principles of affect but also in helping you discover the important
roles that affect plays in our everyday lives, and particularly in our mental and
physical health. The study of the interface between affect and
physical health—that principle that “everything that is physiological is also
psychological”—is a key focus of the branch of psychology known as health psychology. The importance of this topic has made health
psychology one of the fastest growing fields in psychology.
The Historical Theories of Cannon-Bard, James-Lange, and Schachter-Singer
Most of us aren’t faced with the need to make a split-second life-or-death
decision as Captain Sullenberger had to do; however, we have all faced times
when we felt strong emotions. Imagine you are awakened in the middle of the
night by a strange noise in your family room. You have no idea of what made the
noise. Immediately, you feel the signs of autonomic arousal: your heart pounds,
you feel flushed and maybe sick to your stomach, you have trouble breathing. You
are afraid of what you might find in your family room, so you pull the covers
over your head trying to muster the courage to take a look. You are experiencing
the physiological part of emotion—arousal—and the emotion—fear. I’m sure you
have had similar feelings in other situations, perhaps when you were in love,
angry, embarrassed, frustrated, or very sad.
If you experience the fear and arousal at the same time—heart pounding and the
fear—your experiences are consistent with the Cannon-Bard
theory of emotions. The Cannon-Bard theory proposes
that emotions and arousal occur at the same time. If your experiences
are like mine, as you reflected on the arousal that you have experienced in
strong emotional situations, you probably thought something like, “I was afraid
and my heart started beating like crazy.” According to the theory of emotion
proposed by Walter Cannon and Philip Bard, the experience of the emotion (in
this case, “I’m afraid”) occurs alongside our experience of the arousal (“my
heart is beating fast”). According to the Cannon-Bard theory of emotion, the
experience of an emotion is accompanied by physiological arousal. Thus,
according to this model of emotion, as we become aware of danger, our heart rate
also increases.
But there is another way to look at the connection between fear and arousal. In
the same story above, you are afraid because you pulled the covers over your
head. You react first and then experience the emotion. This alternative way of
explaining the connection between emotion and arousal was proposed by William
James and Carl Lange and is called the James-Lange theory.
Although the idea that the experience of an emotion occurs alongside the
accompanying arousal seems intuitive to our everyday experiences, James and
Lange had another idea about the role of arousal. According to the James-Lange
theory of emotion, our experience of an emotion is the result
of the arousal that we experience. This approach proposes that the
arousal and the emotion are not independent, but rather that the emotion depends
on the arousal. The fear does not occur along with the racing heart but occurs
because of the racing heart. As William James [1] put it, “We feel sorry because we cry, angry because we
strike, afraid because we tremble” (p. 190). A
fundamental aspect of the James-Lange theory is that different patterns of
arousal may create different emotional experiences.
There is yet another way to look at it. You realize you are experiencing the
physical signs of arousal. Then you think about the situation you are in (an
unexplained noise in the middle of the night) and you explain that arousal as
fear. This third explanation is consistent with Stanley
Schachter and Jerome Singer’s two-factor theory of emotion. The
two-factor theory of emotion argues that the arousal that we
experience is basically the same in every emotion, and that all emotions
(including the basic emotions) are differentiated only by our cognitive
appraisal of the source of the arousal. The two-factor theory of
emotion asserts that the experience of emotion is determined by the intensity of
the arousal we are experiencing, but that the cognitive appraisal of the
situation determines what the emotion will be. Because both arousal and
appraisal are necessary, we can say that emotions have two factors, an arousal
factor and a cognitive factor: [2]
emotion = arousal + cognition.
To fully understand the Schachter-Singer theory, it’s helpful to look at another
example. Let’s say you’re experiencing the same arousal—pounding heart, feeling
flushed, having difficulty catching your breath. But this time you are engaging
in one of your favorite activities—parachute jumping. Now you interpret the same
feelings of arousal as exhilaration not fear. You have different interpretation
of the situation you’re in and therefore a different label for the same
arousal.
Later in our discussion, we look at a physiological view of emotions which offers
some support for the Schachter-Singer two factor theory.
learn by doing
Three Theories of Emotion
You have just learned about three theories of emotion: the Cannon-Bard theory,
the James-Lange theory, and the Schachter-Singer theory. In this activity, you
will complete the following figure so that it represents the association between
arousal and emotion according to each theory.
Adapted from Flat World Knowledge, Introduction to Psychology, v1.0, CC-BY-NC-SA.
References
- James, W.
(1884).
"What is an emotion?." Mind. Volume 9. Number 34. 188–205 Pages.
- Schachter, S., and Singer, J.
(1962).
"Cognitive, social, and physiological determinants of emotional
state." Psychological Review. Volume 69. Number 5. 379–399 Pages.
Research Support for Cannon-Bard and James-Lange
There is research evidence to support each of these theories. The operation of
the fast emotional pathway (see the figure "Slow and Fast Emotional Pathways" in the module)
supports the idea that arousal and emotions occur together. The emotional
circuits in the limbic system are activated when an emotional stimulus is
experienced, and these circuits quickly create corresponding physical reactions. [1]
The process happens so quickly that it may feel to us as if
emotion is simultaneous with our physical arousal.
On the other hand, and as predicted by the James-Lange theory, our experiences of
emotion are weaker without arousal. Patients who have spinal injuries that
reduce their experience of arousal also report decreases in emotional responses. [2]
There is also at least some support for the idea that
different emotions are produced by different patterns of arousal. People who
view fearful faces show more amygdala activation than those who watch angry or
joyful faces, [3] [4] we
experience a red face and flushing when we are embarrassed but not when we
experience other emotions, [5]
and different hormones are released when we experience compassion than when we
experience other emotions. [6]
Research Support for Schachter-Singer: Misattributing Arousal
In some cases it may be difficult for a person who is experiencing a high level
of arousal to accurately determine which emotion she is experiencing. That is,
she may be certain that she is feeling arousal, but the meaning of the arousal
(the cognitive factor) may be less clear. Some romantic relationships, for
instance, have a very high level of arousal, and the partners alternatively
experience extreme highs and lows in the relationship. One day they are madly in
love with each other and the next they are in a huge fight. In situations that
are accompanied by high arousal, people may be unsure what emotion they are
experiencing. In the high arousal relationship, for instance, the partners may
be uncertain whether the emotion they are feeling is love, hate, or both at the
same time (sound familiar?). The tendency for people to
incorrectly label the source of the arousal that they are experiencing
is known as the misattribution of arousal.
In one interesting field study by Dutton and Aron, [7] an attractive
young woman approached individual young men as they crossed a wobbly, long
suspension walkway hanging more than 200 feet above a river in British Columbia,
Canada. The woman asked each man to help her fill out a class questionnaire.
When he had finished, she wrote her name and phone number on a piece of paper,
and invited him to call if he wanted to hear more about the project. More than
half of the men who had been interviewed on the bridge later called the woman.
In contrast, men approached by the same woman on a low solid bridge, or who were
interviewed on the suspension bridge by men, called significantly less
frequently. The idea of misattribution of arousal can explain this result—the
men were feeling arousal from the height of the bridge, but they misattributed
it as romantic or sexual attraction to the woman, making them more likely to
call her.
If you think a bit about your own experiences of different emotions, and if you
consider the equation that suggests that emotions are represented by both
arousal and cognition, you might start to wonder how much was determined by
each. That is, do we know what emotion we are experiencing by monitoring our
feelings (arousal) or by monitoring our thoughts (cognition)? The bridge study
you just read about might begin to provide you an answer: The men seemed to be
more influenced by their perceptions of how they should be feeling (their
cognition) rather than by how they actually were feeling (their arousal).
Stanley Schachter and Jerome Singer [8] directly tested this prediction
of the two-factor theory of emotion in a well-known experiment. Schachter and
Singer believed that the cognitive part of the emotion was critical—in fact,
they believed that the arousal that we are experiencing could be interpreted as
any emotion, provided we had the right label for it. Thus they hypothesized that
if an individual is experiencing arousal for which he has no immediate
explanation, he will “label” this state in terms of the cognitions that are
created in his environment. On the other hand, they argued that people who
already have a clear label for their arousal would have no need to search for a
relevant label, and therefore should not experience an emotion.
In the research, male participants were told that they would be participating in
a study on the effects of a new drug, called “suproxin,” on vision. On the basis
of this cover story, the men were injected with a shot of the neurotransmitter
epinephrine, a drug that normally creates feelings of tremors, flushing, and
accelerated breathing in people. The idea was to give all the participants the
experience of arousal.
Then, according to random assignment to conditions, the men were told that the
drug would make them feel certain ways. The men in the epinephrine informed condition were told the truth about the effects
of the drug—they were told that they would likely experience tremors, their
hands would start to shake, their hearts would start to pound, and their faces
might get warm and flushed. The participants in the epinephrine-uninformed condition, however, were told something
untrue—that their feet would feel numb, that they would have an itching
sensation over parts of their body, and that they might get a slight headache.
The idea was to make some of the men think that the arousal they were
experiencing was caused by the drug (the informed
condition), whereas others would be unsure where the arousal came from
(the uninformed condition).
Then the men were left alone with a confederate who they thought had received the
same injection. While they were waiting for the experiment (which was supposedly
about vision) to begin, the confederate behaved in a wild and crazy (Schachter
and Singer called it “euphoric”) manner. He wadded up spitballs, flew paper
airplanes, and played with a hula-hoop. He kept trying to get the participant to
join in with his games. Then right before the vision experiment was to begin,
the participants were asked to indicate their current emotional states on a
number of scales. One of the emotions they were asked about was euphoria.
If you are following the story, you will realize what was expected: The men who
had a label for their arousal (the informed group) would
not be experiencing much emotion because they already had a label available for
their arousal. The men in the misinformed group,
on the
other hand, were expected to be unsure about the
source of the arousal. They
needed to find an explanation for their arousal, and
the confederate provided
one. As you can see in the left side of the figure
below, this is just what they found. The participants in the misinformed
condition were more likely to be experiencing
euphoria (as measured by their
behavioral responses with the confederate) than were
those in the informed
condition.
Then Schachter and Singer conducted another part of the study, using new
participants. Everything was exactly the same except for the behavior of the
confederate. Rather than being euphoric, he acted angry. He complained about
having to complete the questionnaire he had been asked to do, indicating that
the questions were stupid and too personal. He ended up tearing up the
questionnaire that he was working on, yelling “I don’t have to tell them that!”
Then he grabbed his books and stormed out of the room.
What do you think happened in this condition? The answer is the same thing: The
misinformed participants experienced more anger (again as measured by the
participant’s behaviors during the waiting period) than did the informed
participants as shown on the right side of the figue above. The idea is that
because cognitions are such strong determinants of emotional states, the same
state of physiological arousal could be labeled in many different ways,
depending entirely on the label provided by the social situation. As Schachter
and Singer [8] put it, “Given a state of physiological
arousal for which an individual has no immediate explanation, he will ‘label’
this state and describe his feelings in terms of the cognitions available to
him” (p. 381).
Because it assumes that arousal is constant across emotions, the two-factor
theory also predicts that emotions may transfer or “spill over” from one highly
arousing event to another. My university basketball team recently won the NCAA
basketball championship, but after the final victory some students rioted in the
streets near the campus, lighting fires and burning cars. This seems to be a
very strange reaction to such a positive outcome for the university and the
students, but it can be explained through the spillover of the arousal caused by
happiness to destructive behaviors. The principle of
excitation transfer refers to the phenomenon that occurs when people
who are already experiencing arousal from one event tend to also experience
unrelated emotions more strongly.
In sum, each of the three theories of emotion has something to support it. In terms of
Cannon-Bard, emotions and arousal generally are subjectively experienced together, and
the spread is very fast. In support of the James-Lange theory, there is at least some
evidence that arousal is necessary for the experience of emotion, and that the patterns
of arousal are different for different emotions. And in line with the two-factor model,
there is also evidence that we may interpret the same patterns of arousal differently in
different situations.
References
- LeDoux, J. E.
(2000).
"Emotion circuits in the brain." Annual Review of Neuroscience. Volume 23. Number 1. 155–184 Pages.
- Hohmann, G. W.
(1966).
"Some effects of spinal cord lesions on experienced emotional
feelings." Psychophysiology. Volume 3. Number 2. 143–456 Pages.
- Whalen, P. J., Shin, L. M., McInerney, S.
C., Fischer, H., Wright, C. I., and Rauch, S. L.
(2001).
"A functional MRI study of human amygdala responses to facial
expressions of fear versus anger." Emotion. Volume 1. Number 1. 70–83
Pages.
- Witvliet, C. V., and Vrana, S. R.
(1995).
"Psychophysiological responses as indices of affective dimensions."
Psychophysiology. Volume 32. Number 5. 436–443 Pages.
- Leary, M. R., Britt, T. W., Cutlip, W. D., and Templeton, J. L.
(1992).
"Social blushing." Psychological Bulletin. Volume 112. Number 3. 446–460 Pages.
- Oatley, K., Keltner, D., and Jenkins, J. M.
(2006).
Understanding Emotions. Blackwell. Malden, MA. Edition 2.
- Dutton, D., and Aron, A.
(1974).
"Some evidence for heightened sexual attraction under conditions of
high anxiety." Journal of Personality and Social Psychology. Volume 30.
Number 4. 510–517 Pages.
- Schachter, S., and Singer, J.
(1962).
"Cognitive, social, and physiological determinants of emotional
state." Psychological Review. Volume 69. Number 5. 379–399 Pages.
The most fundamental emotions, known as the basic emotions, are
those of anger, disgust, fear, happiness, sadness, and surprise (and some psychologists also include contempt).
The basic emotions have a long history in human evolution, and they have developed in
large part to help us make rapid judgments about stimuli and to quickly guide
appropriate behavior. [1]
The basic emotions are determined in large part by one of the
oldest parts of our brain, the limbic system, including the amygdala, the hypothalamus,
and the thalamus. Because they are primarily evolutionarily determined, the basic
emotions are experienced and displayed in much the same way across cultures, [2] [3] [4] [5]
and people are quite accurate at judging the facial expressions of people from different
cultures. Watch the following video to see a demonstration of the basic emotions.
Not all of our emotions come from the old parts of our brain; we also interpret our
experiences to create a more complex array of emotional experiences. For instance, the
amygdala may sense fear when it senses that the body is falling, but that fear may be
interpreted completely differently (perhaps even as “excitement”) when we are falling on
a roller-coaster ride than when we are falling from the sky in an airplane that has lost
power. The cognitive interpretations that accompany
emotions—known as cognitive appraisal—allow us to experience
a much larger and more complex set of secondary emotions, as
shown in the following figure. Although they are in large part cognitive, our
experiences of the secondary emotions are determined in part by arousal (on the vertical
axis of the figure) and in part by their valence—that is, whether they are pleasant or
unpleasant feelings (on the horizontal axis of the figure).
When you succeed in reaching an important goal, you might spend some time enjoying your
secondary emotions, perhaps the experience of joy, satisfaction, and contentment. But
when your close friend wins a prize that you thought you had deserved, you might also
experience a variety of secondary emotions (in this case, the negative ones)—for
instance, feeling angry, sad, resentful, and ashamed. You might mull over the event for
weeks or even months, experiencing these negative emotions each time you think about
it. [6]
References
- LeDoux, J. E.
(2000).
"Emotion circuits in the brain." Annual Review of Neuroscience. Volume 23. Number 1. 155–184 Pages.
- Ekman, P.
(1992).
"Are there basic emotions?." Psychological Review. Volume 99. Number 3. 550–553 Pages.
- Elfenbein, H. A., and Ambady, N.
(2002).
"On the universality and cultural specificity of emotion recognition: A
meta-analysis." Psychological Bulletin. Volume 128. Number 2. 203–223 Pages.
- Elfenbein, H. A., and Ambady, N.
(2003).
"When familiarity breeds accuracy: Cultural exposure and facial emotion
recognition." Journal of Personality and Social Psychology. Volume 85. Number 2. 276–290 Pages.
- Fridlund, A. J., Ekman, P., and Oster, H.
(1987).
Nonverbal Behavior and Communication.
Chapter Facial expressions of emotion. Lawrence Erlbaum Associates.
Hillsdale, NJ. Edition 2. 143–223 Pages. A. Siegman and S. Feldstein
(Eds.).
- Martin, L. L., and Tesser, A.
(2006).
Judgments Over Time: The Interplay of Thoughts, Feelings, and
Behaviors. Chapter Extending the goal progress theory of rumination: Goal reevaluation and
growth. Oxford University Press. New York. 145–162 Pages. L. J. Sannaand E. C. Chang (Eds.).
The distinction between the primary and the secondary emotions is paralleled by
two brain pathways: a fast pathway and a slow pathway. [1] [2] [3]
The thalamus acts as the major gatekeeper in this process as shown in the
figure below. Our response to the basic emotion of fear, for instance, is
primarily determined by the fast pathway through the limbic system. When a car
pulls out in front of us on the highway, the thalamus activates and sends an
immediate message to the amygdala. We quickly move our foot to the brake pedal.
Secondary emotions are more determined by the slow pathway through the frontal
lobes in the cortex. When we stew in jealousy over the loss of a partner to a
rival or recollect on our win in the big tennis match, the process is more
complex. Information moves from the thalamus to the frontal lobes for cognitive
analysis and integration, and then from there to the amygdala. We experience
the arousal of emotion, but it is accompanied by a more complex cognitive
appraisal, producing more refined emotions and behavioral responses.
Let’s go back to the example we used earlier when talking about the historical
theories. When you hear a strange noise in your bedroom late at night, you are
likely to react fearfully before your know whether or not there is something to
fear. Which pathway is involved in this reaction? If you guessed the fast
pathway, you’re right. No cognition is involved so the pathway is direct to the
amygdala. Now you go into your bedroom, check, and realize it was just your cat
jumping down from a shelf. You’ve appraised the situation as harmless so the
fear abates. What’s the pathway here? Right, this is the slow pathway because
you’re using your cortex to appraise the situation.
Fast pathway reactions involve no cognition and often can’t be overridden by
cognitive appraisal. A person reacts fearfully (screaming and jumping backward)
to the mere site of any snake, dangerous or not. This person lives in an area
where there are no dangerous snakes and they know it. They can appraise the
snake as harmless but the fear reaction occurs anyway.
Because there are more neural connections that feed into the frontal cortex
from the amygdala than the other way around, it is not uncommon for people to
make decisions based on emotion rather than rational thinking. When voting,
people are unlikely to vote for a candidate they don’t like even if that
candidate’s political beliefs more closely match their own.
Emotionally based decisions are not always a bad thing. Although emotions might
seem to be more frivolous or less important in comparison to our more rational
cognitive processes, both emotions and cognitions can help us make effective
decisions. In some cases we take action after rationally processing the costs
and benefits of different choices, but in other cases we rely on our emotions.
Emotions become particularly important in guiding decisions when the
alternatives between many complex and conflicting alternatives present us with
a high degree of uncertainty and ambiguity, making a complete cognitive
analysis difficult. In these cases we often rely on our emotions to make
decisions, and these decisions may in many cases be more accurate than those
produced by cognitive processing. [4] [5] [6] [7]
References
- Damasio, A.
(2000).
The Feeling of What Happens: Body and Emotion in the Making of Consciousness. Mariner Books. New York.
- LeDoux, J. E.
(2000).
"Emotion circuits in the brain." Annual Review of Neuroscience. Volume 23. Number 1. 155–184 Pages.
- Ochsner, K. N., Bunge, S. A., Gross, J. J.,
and Gabrieli, J. D. E.
(2002).
"Rethinking feelings: An fMRI study of the cognitive regulation of
emotion." Journal of Cognitive Neuroscience. Volume 14. Number 8.
1215–1229 Pages.
- Damasio, A.
(1994).
Descartes’ Error: Emotion, Reason, and the Human Brain. Grosset/Putnam. New York.
- Dijksterhuis, A., Bos, M. W., Nordgren,
L. F., and van Baaren, R. B.
(2006).
"On making the right choice: The deliberation-without-attention
effect." Science. Volume 311. Number 5763. 1005–1007 Pages.
- Nordgren, L. F., and Dijksterhuis, A. P.
(2009).
"The devil is in the deliberation: Thinking too much reduces
preference consistency." Journal of Consumer Research. Volume 36. Number
1. 39–46 Pages.
- Wilson, T. D., and Schooler, J. W.
(1991).
"Thinking too much: Introspection can reduce the quality of
preferences and decisions." Journal of Personality and Social
Psychology. Volume 60. Number 2. 181–192 Pages.
In addition to experiencing emotions internally, we also express our emotions to others,
and we learn about the emotions of others by observing them. This communication process
has evolved over time, and is highly adaptive. One way that we perceive the emotions of
others is through their nonverbal communication, that is, communication that does not
involve words. [1] [2] Nonverbal
communication includes our tone of voice, gait, posture, touch, and facial expressions,
and we can often accurately detect the emotions that other people are experiencing
through these channels.
The most important communicator of emotion is the face. The face contains 43 muscles that
allow it to make more than 10,000 unique configurations and to express a wide variety of
emotions. For example, happiness is expressed by smiles, which are created by two of the
major muscles surrounding the mouth and the eyes, and anger is created by lowered brows
and firmly pressed lips.
In addition to helping us express our emotions, the face also helps us feel emotion. The
facial feedback hypothesis proposes that the movement of our facial
muscles can trigger corresponding emotions. Fritz Strack and his colleagues [3]
asked their research participants to hold a pen in their teeth (mimicking
the facial action of a smile) or between their lips (similar to a frown), and then had
them rate the funniness of a cartoon. They found that the cartoons were rated as more
amusing when the pen was held in the “smiling” position—the subjective experience of
emotion was intensified by the action of the facial muscles.
When we communicate electronically, we can’t see the writer’s nonverbal communications,
so many people add emoticons. The simplest emoticons are created on the keyboard to add
a smiley face or a sad face. When texting on a smartphone, you can use text
symbols such as the following:
1. :-D for laughing
2. :-o for surprise
3. ;-) for happy
4. :-|| for angry
5. :-P for disgust or sticking your tongue out
6. :-( for sad
Acronyms are another way to communicate emotion; for example:
1. LOL for laughing out loud,
2. EWG for evil wicked grin,
3. JT for just teasing,
4. MEGO for my eyes glaze over
5. AML for all my love
6. SB for smiling back
The following table shows some of the important nonverbal behaviors we use to express
emotion and some other information (particularly liking or disliking and dominance or
submission).
| Some Common Nonverbal Communicators |
|---|
| From Flat World Knowledge, Introduction to Psychology, CC-BY-NC-SA. |
| Nonverbal cue |
Description |
Examples |
| Proxemics |
Rules about the appropriate use of personal space |
Standing nearer to someone can express liking or dominance. |
| Body appearance |
Expressions based on alterations to our body |
Body building, breast augmentation, weight loss, piercings, and tattoos are
often used to appear more attractive to others. |
| Body positioning and movement |
Expressions based on how our body appears |
A more “open” body position can denote liking; a faster walking speed can
communicate dominance. |
| Gestures |
Behaviors and signs made with our hands or faces |
The peace sign communicates liking; the “finger” communicates disrespect. |
| Facial expressions |
The variety of emotions we express, or attempt to hide, through our face |
Smiling or frowning and staring or avoiding looking at another can express
liking or disliking as well as dominance or submission. |
| Paralanguage |
Clues to identity or emotions contained in our voices |
Pronunciation, accents, and dialect can be used to communicate identity and
liking. |
|
Just as there is no “universal” spoken language, there is no universal nonverbal
language. For instance, in the United States and many Western cultures, we express
disrespect by showing the middle finger (the “finger” or the “bird”). But in Britain,
Ireland, Australia, and New Zealand, the “V” sign (made with back of the hand facing the
recipient) serves a similar purpose. In countries where Spanish, Portuguese, or French
are spoken, a gesture in which a fist is raised and the arm is slapped on the bicep is
equivalent to the finger, and in Russia, Indonesia, Turkey, and China, a sign in which
the hand and fingers are curled and the thumb is thrust between the middle and index
fingers is used for the same purpose.
These results, and others like them, show that our behaviors, including our facial
expressions, are influenced by, but also influence, our affect. We may smile because we
are happy, but we are also happy because we are smiling. And we may stand up straight
because we are proud, but we are proud because we are standing up straight. [4]
References
- Ambady, N., and Weisbuch, M.
(2010).
Handbook of Social Psychology, Vol. 1. Chapter Nonverbal behavior. Wiley. Hoboken, NJ. Edition 5. 464–497 Pages. S. T. Fiske, D. T. Gilbert, and G. Lindzey (Eds.).
- Andersen, P.
(2007).
Nonverbal Communication: Forms and Functions. Waveland Press. Long Grove, IL. Edition 2.
- Strack, F., Martin, L., and Stepper, S.
(1988).
"Inhibiting and facilitating conditions of the human smile: A
nonobtrusive test of the facial feedback hypothesis." Journal of
Personality and Social Psychology. Volume 54. Number 5. 768–777 Pages.
- Stepper, S., and Strack, F.
(1993).
"Proprioceptive determinants of emotional and nonemotional
feelings." Journal of Personality and Social Psychology. Volume 64.
Number 2. 211–220 Pages.
The stress of the Monday through Friday grind can
be offset by the fun that we can have on the weekend, and the concerns that we have about
our upcoming chemistry exam can be offset by a positive attitude toward school, life, and
other people. Put simply, the best antidote for stress is a happy one: Think positively,
have fun, and enjoy the company of
others.
You have probably heard about the “power of positive thinking”—the idea that thinking
positively helps people meet their goals and keeps them healthy, happy, and able to
effectively cope with the negative events that occur to them. It turns out that positive
thinking really works. People who think positively about their future, who believe that
they can control their outcomes, and who are willing to open up and share with others are
healthier people. [1] A positive thinker doesn’t ignore
negative events that happen in their lives. They are just better able to cope by having a
positive outlook. They are thinking this will get better.
The power of positive thinking comes in different forms, but they are all helpful. Some
researchers have focused on optimism, a general
tendency to expect positive outcomes, finding that optimists are happier and have
less stress. [2] Others have
focused self-efficacy, the belief in our ability
to carry out actions that produce desired outcomes. It’s a belief that we will be
able to succeed in things we try. Our successes improve our self-efficacy. People with high
self-efficacy respond to environmental and other threats in an active, constructive way—by
getting information, talking to friends, and attempting to face and reduce the difficulties
they are experiencing. These people too are better able to ward off their stresses in
comparison to people with less self-efficacy. [3]
Self-efficacy helps in part because it leads us to perceive that we can control the
potential stressors that may affect us. Workers who have control over their work
environment (e.g., by being able to move furniture and control distractions) experience
less stress, as do patients in nursing homes who are able to choose their everyday
activities. [4] Glass, Reim, and
Singer [5] found that participants who believed
that they could stop a loud noise experienced less stress than those who did not think that
they could, even though the people who had the option never actually used it. The ability
to control our outcomes may help explain why animals and people who have higher status live
longer. [6]
Suzanne Kobasa and her colleagues [7] have argued that the
tendency to be less affected by life’s stressors can be characterized as an individual
difference measure that has a relationship to both optimism and self-efficacy known
as hardiness. Hardy individuals are those who are more positive
overall about potentially stressful life events, who take more direct action to understand
the causes of negative events, and who attempt to learn from them what may be of value for
the future. Hardy individuals use effective coping strategies, and they take better care of
themselves.
Taken together, these various coping skills, including optimism, self-efficacy, and
hardiness, have been shown to have a wide variety of positive effects on our health.
Optimists make faster recoveries from illnesses and surgeries. [8] People with high self-efficacy have been found to be
better able to quit smoking and lose weight and are more likely to exercise regularly. [9] And hardy individuals seem
to cope better with stress and other negative life events. [10]
The positive effects of positive
thinking are particularly important when stress is high. Baker [11] found that in periods of low stress, positive thinking made little
difference in responses to stress, but that during stressful periods, optimists were less
likely to smoke on a day-to-day basis and more likely to respond to stress in more
productive ways, such as by exercising.
It is possible to learn to think more positively, and doing so can be beneficial. Antoni
and colleagues [12] found that pessimistic cancer
patients who were given training in optimism reported more optimistic outlooks after the
training and were less fatigued after their treatments. And Maddi, Kahn, and Maddi [13]
found that a “hardiness training” program that included focusing on ways
to effectively cope with stress was effective in increasing satisfaction and decreasing
self-reported stress.
The benefits of taking positive approaches to stress can last a lifetime. Christopher
Peterson and his colleagues [14] found that the
level of optimism reported by people who had first been interviewed when they were in
college during the years between 1936 and 1940 predicted their health over the next 50
years. Students who had a more positive outlook on life in college were less likely to have
died up to 50 years later of all causes, and they were particularly likely to have
experienced fewer accidental and violent deaths, in comparison to students who were less
optimistic. Similar findings were found for older adults. After controlling for loneliness,
marital status, economic status, and other correlates of health, Levy and Myers found that
older adults with positive attitudes and higher self-efficacy had better health and lived
on average almost 8 years longer than their more negative peers. [15] [16]
And Diener, Nickerson,
Lucas, and Sandvik [17] found that people who had
cheerier dispositions earlier in life had higher income levels and less unemployment when
they were assessed 19 years later.
References
- Seligman, M. E. P., and Csikszentmihalyi, M.
(2000).
"Positive psychology: A introduction." American Psychologist. Volume 55. Number 1. 5–14 Pages.
- Carver, C. S., and Scheier, M. F.
(2009).
Handbook of Individual Differences in Social Behavior. Chapter Optimism. Guilford Press. New York. 330–342 Pages. M. R. Leary and R. H. Hoyle (Eds.).
- Thompson, S. C.
(2009).
Oxford Handbook of Positive Psychology.
Chapter The role of personal control in adaptive functioning. Oxford
University Press. New York. Edition 2. 271–278 Pages. S. J. Lopez and C.
R. Snyder (Eds.).
- Rodin, J.
(1986).
"Aging and health: Effects of the sense of control." Science. Volume 233. Number 4770. 1271–1276 Pages.
- Glass, D. C., Reim, B., and Singer, J. E.
(1971).
"Behavioral consequences of adaptation to controllable and
uncontrollable noise." Journal of Experimental Social Psychology. Volume
7. Number 2. 244–257 Pages.
- Sapolsky, R. M.
(2005).
"The influence of social hierarchy on primate health." Science. Volume 308. Number 5722. 648–652 Pages.
- Kobasa, S. C., Maddi, S. R., and Kahn, S.
(1982).
"Hardiness and health: A prospective study." Journal of Personality
and Social Psychology. Volume 42. Number 1. 168–177 Pages.
- Carver, C. S., Smith, R. G., Antoni, M. H.,
Petronis, V. M., Weiss, S., and Derhagopian, R. P.
(2005).
"Optimistic personality and psychosocial well-being during
treatment predict psychosocial well-being among long-term survivors of
breast cancer." Health Psychology. Volume 24. Number 5. 508–516 Pages.
- Cohen, S., and Pressman, S. D.
(2006).
"Positive affect and health." Current Directions in Psychological Science. Volume 15. Number 3. 122–125 Pages.
- Dolbier, C. L., Smith, S. E., and
Steinhardt, M. A.
(2007).
"Relationships of protective factors to stress and symptoms of
illness." American Journal of Health Behavior. Volume 31. Number 4.
423–433 Pages.
- Baker, S. R.
(2007).
"Dispositional optimism and health status, symptoms, and behaviors:
Assessing ideothetic relationships using a prospective daily diary
approach." Psychology and Health. Volume 22. Number 4. 431–455 Pages.
- Antoni, M. H., Lehman, J. M., Klibourn, K.
M., Boyers, A. E., Culver, J. L., Alferi, S. M., et al.
(2001).
"Cognitive-behavioral stress management intervention decreases the
prevalence of depression and enhances benefit finding among women under
treatment for early-stage breast cancer." Health Psychology. Volume 20.
Number 1. 20–32 Pages.
- Maddi, S. R., Kahn, S., and Maddi, K. L.
(1998).
"The effectiveness of hardiness training." Consulting Psychology
Journal: Practice and Research. Volume 50. Number 2. 78–86 Pages.
- Peterson, C., Seligman, M. E. P., Yurko, K. H., Martin, L. R., and Friedman, H. S.
(1998).
"Catastrophizing and untimely death." Psychological Science. Volume 9. Number 2. 127–130 Pages.
- Levy, B., and Myers, L.
(2005).
"Relationship between respiratory mortality and self-perceptions of
aging." Psychology and Health. Volume 20. Number 5. 553–564 Pages.
- Levy, B., Slade, M., and Kasl, S.
(2002).
"Longitudinal benefit of positive self-perceptions of aging on
functional health." Journals of Gerontology Series B: Psychological
Sciences and Social Science. Volume 57B. Number 5. P409–P417 Pages.
- Diener, E., Nickerson, C., Lucas, R., and Sandvik, E.
(2002).
"Dispositional affect and job outcomes." Social Indicators Research. Volume 59. Number 3. 229–259 Pages.
Happiness is determined in part by genetic factors, such that some people are naturally
happier than others, [1] [2] but also
in part by the situations that we create for ourselves. Psychologists have studied
hundreds of variables that influence happiness, but there is one that is by far the most
important. People who report that they have positive social
relationships with others—the perception of social
support—also report being happier than those who report having less social
support. [3] [4]
Married people report being happier than unmarried people, [5] and people who are connected with and accepted by others
suffer less depression, higher self-esteem, and less social anxiety and jealousy than
those who feel more isolated and rejected. [6]
Social support also helps us better cope with stressors. Koopman, Hermanson, Diamond,
Angell, and Spiegel [7] found that women who
reported higher social support experienced less depression when adjusting to a diagnosis
of cancer, and Ashton and colleagues [8] found
a similar buffering effect of social support for AIDS patients. People with social
support are less depressed overall, recover faster from negative events, and are less
likely to commit suicide. [9] [10] [11] [12]
Social support buffers us against stress in several ways. For one, having people we can
trust and rely on helps us directly by allowing us to share favors when we need them.
These are the direct effects of social support. But having
people around us also makes us feel good about ourselves. These are the appreciation effects of social support. Gençöz and
Özlale found that students with more friends felt less stress and
reported that their friends helped them, but they also reported that having friends made
them feel better about themselves. [13]
Taylor, Klein, Lewis, Gruenewald, Gurung, and Updegraff propose tend-and–befriend as a
female alternative to the flight-or-fight response to stress more likely to be used by
men. Taylor and her colleagues say that when women find themselves in stressful
situations, they spend more time tending to their children and families and seek out the
comfort of friends. [14] The
tend-and-befriend response, so often used by women, is an important and effective way to
reduce stress.
References
- Braungart, J. M., Plomin, R., DeFries, J. C.,
and Fulker, D. W.
(1992).
"Genetic influence on tester-rated infant temperament as assessed
by Bayley’s Infant Behavior Record: Nonadoptive and adoptive siblings
and twins." Developmental Psychology. Volume 28. Number 1. 40–47 Pages.
- Lykken, D. T.
(2000).
Happiness: The Nature and Nurture of Joy and Contentment. St. Martin’s Press. New York.
- Diener, E., Suh, E. M., Lucas, R. E., and Smith, H. L.
(1999).
"Subjective well-being: Three decades of progress." Psychological Bulletin. Volume 125. Number 2. 276–302 Pages.
- Diener, E., Tamir, M., and Scollon, C. N.
(2006).
Bridging Social Psychology: Benefits of Transdisciplinary Approaches.
Chapter Happiness, life satisfaction, and fulfillment: The social
psychology of subjective well-being. Lawrence Erlbaum Associates.
Mahwah, NJ. 379–324 Pages. P. A. M. VanLange (Ed.).
- Pew Research Center.
(2006, February 13).
Are we happy yet?. Retrieved from http://pewresearch.org/pubs/301/are-we-happy-yet.
- Leary, M. R.
(1990).
"Responses to social exclusion: Social anxiety, jealousy,
loneliness, depression, and low self-esteem." Journal of Social and
Clinical Psychology. Volume 9. Number 2. 221–229 Pages.
- Koopman, C., Hermanson, K., Diamond, S.,
Angell, K., and Spiegel, D.
(1998).
"Social support, life stress, pain and emotional adjustment to
advanced breast cancer." Psycho-Oncology. Volume 7. Number 2. 101–110
Pages.
- Ashton, E., Vosvick, M., Chesney, M.,
Gore-Felton, C., Koopman, C., O’Shea, K., et al.
(2005).
"Social support and maladaptive coping as predictors of the change
in physical health symptoms among persons living with HIV/AIDS." AIDS
Patient Care and STDs. Volume 19. Number 9. 587–598 Pages.
- Au, A., Lau, S., and Lee, M.
(2009).
"Suicide ideation and depression: The moderation effects of family
cohesion and social self-concept." Adolescence. Volume 44. Number 176.
851–868 Pages.
- Bertera, E.
(2007).
"The role of positive and negative social exchanges between
adolescents, their peers and family as predictors of suicide ideation."
Child and Adolescent Social Work Journal. Volume 24. Number 6. 523–538
Pages.
- Compton, M., Thompson, N., and Kaslow, N.
(2005).
"Social environment factors associated with suicide attempt among
low-income African Americans: The protective role of family
relationships and social support." Social Psychiatry and Psychiatric
Epidemiology. Volume 40. Number 3. 175–185 Pages.
- Skärsäter, I., Langius, A., Ågren, H.,
Häggström, L., and Dencker, K.
(2005).
"Sense of coherence and social support in relation to recovery in
first-episode patients with major depression: A one-year prospective
study." International Journal of Mental Health Nursing. Volume 14.
Number 4. 258–264 Pages.
- Gençöz, T., and Özlale, Y.
(2004).
"Direct and indirect effects of social support on psychological
well-being." Social Behavior and Personality. Volume 32. Number 5.
449–458 Pages.
- Taylor, S. E., Klein, L. C., Lewis, B. P.,
Gruenewald, T. L., Gurung, R. A. R., and Updegraff, J. A.
(2000).
"Biobehavioral responses to stress in females: Tend-and-befriend,
not fight-or-flight." Psychological Review. Volume 107. Number 3.
411–429 Pages.
Historically, psychology has devoted much of its time to describing problems and helping
people deal with them. Psychologists treat psychological disorders, so most of our
efforts are aimed at trying to make them go away. We spend very little time talking
about people without psychological disorders and how we might make their lives better.
This realization is part of what gave birth to the positive psychology movement. In
positive psychology, we are interested in how we might make people’s lives better even
if, and perhaps especially if, they do not have a psychological disorder. Mihaly
Csikszentmihalyi [1] said people were
happiest when in a state of flow. According to Csikszentmihalyi, people are in a state
of flow when they are completely absorbed in what they are doing, so much so that they
become one with the task. Their energy is completely focused on what they are doing to
the exclusion of what’s going on around them. [1]
One difficulty that people face when trying to improve their happiness is that they may
not always know what will make them happy. As one example, many of us think that if we
just had more money we would be happier. While it is true that we do need money to
afford food and adequate shelter for ourselves and our families, after this minimum
level of wealth is reached, more money does not generally buy more happiness. [2] For instance, as
you can see in the figure below, even though income and material success has improved
dramatically in many countries over the past decades, happiness has not. Despite
tremendous economic growth in France, Japan, and the United States between 1946 and
1990, there was no increase in reports of well-being by the citizens of these countries.
Americans today have about three times the buying power they had in the 1950s, and yet
overall happiness has not increased. The problem seems to be that we never seem to have
enough money to make us “really” happy. Csikszentmihalyi [3] reported that people who earned
$30,000 per year felt that they would be happier if they made $50,000 per year, but that
people who earned $100,000 per year said that they would need $250,000 per year to make
them happy.
References
- Csikszentmihalyi, M.
(1990).
Flow: The Psychology of Optimal Experience. Harper and Row. New York.
- Easterlin, R.
(2005).
"Feeding the illusion of growth and happiness: A reply to Hagerty
and Veenhoven." Social Indicators Research. Volume 74. Number 3. 429–443
Pages.
- Csikszentmihalyi, M.
(1999).
"If we are so rich, why aren’t we happy?." American Psychologist. Volume 54. Number 10. 821–827 Pages.
These findings might lead us to conclude that we don’t always know what does or what
might make us happy, and this seems to be at least partially true. For instance, Jean
Twenge and her colleagues [1] found in
several studies that although people with children frequently claim that having children
makes them happy, couples who do not have children actually report being happier than
those who do.
Psychologists have found that people’s ability to predict their future
emotional states is not very accurate. Wilson and Gilbert [2] call this affective
forecasting. For one, people overestimate their emotional reactions to events.
Although people think that positive and negative events that might occur to them will
make a huge difference in their lives, and although these changes do make at least some
difference in life satisfaction, they tend to be less influential than we think they are
going to be. Positive events tend to make us feel good, but their effects wear off
pretty quickly, and the same is true for negative events. For instance, Brickman,
Coates, and Janoff-Bulman [3] interviewed
people who had won more than $50,000 in a lottery and found that they were not happier
than they had been in the past and were also not happier than a control group of similar
people who had not won the lottery. On the other hand, the researchers found that
individuals who were paralyzed as a result of accidents were not as unhappy as might be
expected.
How can this possibly be? There are several reasons. First, people are resilient: they
bring their coping skills to play when negative events occur, and this makes them feel
better. Second, most people do not continually experience very positive, or very
negative, affect over a long period of time but rather adapt to their current
circumstances. Just as we enjoy the second chocolate bar we eat less than we enjoy the
first, as we experience more and more positive outcomes in our daily lives, we habituate
to them and our life satisfaction returns to a more moderate level. [4]
Another reason we may mispredict our happiness is that our social comparisons change when
our own status changes as a result of new events. People who are wealthy compare
themselves to other wealthy people, people who are poor tend to compare with other poor
people, and people who are ill tend to compare with other ill people. When our
comparisons change, our happiness levels are correspondingly influenced. And when people
are asked to predict their future emotions, they may focus only on the positive or
negative event they are asked about, and forget about all the other things that won’t
change. Wilson, Wheatley, Meyers, Gilbert, and Axsom [5] found that when people were asked to focus on all the more regular
things they will still be doing in the future (working, going to church, socializing
with family and friends, and so forth), their predictions about how something really
good or bad would influence them were less extreme.
References
- Twenge, J., Campbell, W., and Foster, C.
(2003).
"Parenthood and marital satisfaction: A meta-analytic review."
Journal of Marriage and Family. Volume 65. Number 3. 574–583 Pages.
- Wilson, T. D., and Gilbert, D. T.
(2005).
"Affective forecasting: Knowing what to want." Current Directions
in Psychological Science. Volume 14. Number 3. 131–134 Pages.
- Brickman, P., Coates, D., and
Janoff-Bulman, R.
(1978).
"Lottery winners and accident victims: Is happiness relative?."
Journal of Personality and Social Psychology. Volume 36. Number 8.
917–927 Pages.
- Small, D. M., Zatorre, R. J., Dagher, A.,
Evans, A. C., and Jones-Gotman, M.
(2001).
"Changes in brain activity related to eating chocolate: From
pleasure to aversion." Brain. Volume 124. Number 9. 1720–1733 Pages.
- Wilson, T. D., Wheatley, T., Meyers, J. M.,
Gilbert, D. T., and Axsom, D.
(2000).
"Focalism: A source of durability bias in affective forecasting."
Journal of Personality and Social Psychology. Volume 78. Number 5.
821–836 Pages.
Motivations are often considered in psychology in terms of drives, which are internal states that are
activated when the physiological characteristics of the body are out of
balance, and goals, which are desired end states that we strive to attain. Motivation can thus be
conceptualized as a series of behavioral responses that lead us to attempt to
reduce drives and to attain goals by comparing our current state with a desired
end state. [1] Like a thermostat
on an air conditioner, the body tries to maintain homeostasis, the natural state of the body’s
systems, with goals, drives, and arousal in balance. When a drive or
goal is aroused—for instance, when we are hungry—the thermostat turns on and we
start to behave in a way that attempts to reduce the drive or meet the goal (in
this case to seek food). As the body works toward the desired end state, the
thermostat continues to check whether or not the end state has been reached.
Eventually, the need or goal is satisfied (we eat), and the relevant behaviors
are turned off. The body’s thermostat continues to check for homeostasis and is
always ready to react to future needs.
One
of the ways psychologists have looked at motivation is to discuss the
difference between intrinsic and extrinsic motivation. Someone who is intrinsically motivated works because they enjoy the task, they believe the task is important and they desire to
do a good job. Intrinsic motivation resides within the individual.
Earlier, we talked about a very good example of intrinsic motivation. People in
a state of flow [2] are intrinsically motivated.
They enjoy the task so much that they get lost in it. On the other hand, a
person extrinsically motivated works because they are getting a reward such as money or praise.
Extrinsic motivation exists outside the person. You learned that reinforcement
and punishment can be used to intrinsic and extrinsic motivation. Someone who
is intrinsically motivated works because they enjoy the task, they believe the
task is important and they desire to do a good job. Intrinsic motivation
resides within the individual.
People
in a state of flow are intrinsically motivated.
They enjoy the task so much that they get lost in it. On the other hand, a
person extrinsically motivated works because they are getting a reward such as
money or praise. Extrinsic motivation exists outside the person. You learned in
the unit on learning that reinforcement and punishment can be used to change
behavior. They are both extrinsic motivators.
When you are intrinsically motivated, you need no external reinforcers such as
good grades. You study and learn because you like the subject material. You are
more likely to continue a task if intrinsically motivated. One danger with
extrinsic motivation is that once the reward such as praise or good grades
stops, you may not continue with the behavior. Using rewards for a task that
the person already enjoys doing may not have the intended effect. Oftentimes it
makes the task less enjoyable. The person may lose their intrinsic motivation
and do the task only for rewards. For example, your child gets good grades in
school because they enjoy learning. Then you start paying your child for every
A or B they receive. You are running the risk that your child will lose their
intrinsic motivation and continue to get good grades only if you pay them. It’s
generally not a good idea to reward a behavior that a person already enjoys
doing.
References
- Lawrence, J. W., Carver, C. S., and Scheier, M.
F.
(2002).
"Velocity toward goal attainment in immediate experience as a
determinant of affect." Journal of Applied Social Psychology. Volume 32.
Number 4. 788–802 Pages.
- Csikszentmihalyi, M.
(1990).
Flow: The Psychology of Optimal Experience. Harper and Row. New York.
Along with the need to drink fresh water, which humans can normally attain in all except
the most extreme situations, the need for food is the most fundamental and important human
need. More than 1 in 10 U.S. households contain people who live without enough nourishing
food, and this lack of proper nourishment has profound effects on their abilities to create
effective lives. [1] When people are
extremely hungry, their motivation to attain food completely changes their behavior. Hungry
people become listless and apathetic to save energy and then become completely obsessed
with food. Ancel Keys and his colleagues [2] found that volunteers
who were placed on severely reduced-calorie diets lost all interest in sex and social
activities, becoming preoccupied with food. Like most interesting psychological phenomena,
the simple behavior of eating has both biological and social determinants as shown in the
figure below. Biologically, hunger is controlled by the interactions among complex pathways
in the nervous system and a variety of hormonal and chemical systems in the brain and body.
The stomach is of course important. We feel more hungry when our stomach is empty than when
it is full. But we can also feel hunger even without input from the stomach. Two areas of
the hypothalamus are known to be particularly important in eating. The lateral part of the
hypothalamus responds primarily to cues to start eating, whereas the ventromedial part of
the hypothalamus primarily responds to cues to stop eating. If the lateral part of the
hypothalamus is damaged, the animal will not eat even if food is present, whereas if the
ventromedial part of the hypothalamus is damaged, the animal will eat until it is
obese. [3]
Hunger is also determined by hormone levels as depicted in the following
figure. Glucose is the main sugar that the body uses for energy, and the brain
monitors blood glucose levels to determine hunger. Glucose levels in the
bloodstream are regulated by insulin, a hormone secreted by the pancreas gland. When insulin is low, glucose
is not taken up by body cells, and the body begins to use fat as an energy
source. Eating and appetite are also influenced by other hormones, including
orexin, ghrelin, and leptin. [4] [5]
Normally the interaction of the various systems that determine hunger creates a
balance, or homeostasis, in which we eat when we are hungry and stop eating
when we feel full. But homeostasis varies among people; some people simply
weigh more than others, and there is little they can do to change their
fundamental weight. Weight is determined in large part by the basal metabolic rate, the amount of energy expended
while at rest. Each person’s basal metabolic rate is different, due to
his or her unique physical makeup and physical behavior. A naturally occurring
low metabolic rate, which is determined entirely by genetics, makes weight
management a very difficult undertaking for many people.
How we eat is also influenced by our environment. When researchers rigged
clocks to move faster, people got hungrier and ate more, as if they thought
they must be hungry again because so much time had passed since they last
ate. [6] And if we forget that we have already eaten,
we are likely to eat again even if we are not actually hungry. [7]
Cultural norms about appropriate weights also influence eating behaviors. Current norms for
women in Western societies are based on a very thin body ideal, emphasized by television
and movie actresses, models, and even children’s dolls, such as the ever-popular Barbie.
These norms for excessive thinness are very difficult for most women to attain: Barbie’s
measurements, if translated to human proportions, would be about 36 in.–18 in.–33 in. at
bust–waist–hips, measurements that are attained by less than 1 in 100,000 women. [8] Many women
idealize being thin and yet are unable to reach the standard that they prefer.
Cultural norms for men are represented by GI Joe and other action figures as well as the
emphasis on lean bodies and six-pack abs. These images are just as unrepresentative of the
average male as Barbie and other media images are of the average female. Men as well as
women are affected by the cultural emphasis on being thin. The changing norms for men and
women play a part too. Because men are no longer always the breadwinner or at the top of
the corporate ladder, they seek other ways to prove their masculinity. Well-sculpted bodies
are one way to do that.
References
- Hunger Notes.
(n.d.).
How many children are hungry in the United States?. Retrieved from http://www.worldhunger.org/articles/04/editorials/hungry_us_children.htm.
- Keys, A., Brožek, J., Henschel, A., Mickelsen, O., and Taylor, H. L.
(1950).
The Biology of Human Starvation, Vols. 1–2. University of Minnesota Press. Minneapolis.
- Wolf, G., and Miller, N. E.
(1964).
"Lateral hypothalamic lesions: Effects on drinking elicited by
carbachol in preoptic area and posterior hypothalamus." Science. Volume
143. Number 3606. 585–587 Pages.
- Brennan, A. M., and Mantzoros, C. S.
(2006).
"Drug insight: The role of leptin in human physiology and
pathophysiology-emerging clinical applications." Nature Clinical
Practice Endocrinology Metabolism. Volume 2. Number 6. 318–327 Pages.
- Nakazato, M., Murakami, N., Date, Y., Kojima, M., Matsuo, H., Kangawa, K., and Matsukura S.
(2001).
"A role for ghrelin in the central regulation of feeding." Nature. Volume 409. Number 6817. 194–198 Pages.
- Schachter, S.
(1968).
"Obesity and eating." Science. Volume 161. Number 3843. 751–756 Pages.
- Rozin, P., Dow, S., Moscovitch, M., and
Rajaram, S.
(1998).
"What causes humans to begin and end a meal? A role for memory for
what has been eaten, as evidenced by a study of multiple meal eating in
amnesic patients." Psychological Science. Volume 9. Number 5. 392–396
Pages.
- Norton, K. I., Olds, T. S., Olive, S., and Dank, S.
(1996).
"Ken and Barbie at life size." Sex Roles. Volume 34. Number 3–4. 287–294 Pages.
In some cases, the desire to be thin can lead to eating disorders, which are estimated to
affect about 1 million males and 10 million females the United States alone. [1] [2]
Anorexia nervosa is an eating disorder
characterized by extremely low body weight, distorted body image, an obsession with
exercise, and an obsessive fear of gaining weight. Nine out of 10 sufferers are
women. Anorexia begins with a severe weight loss diet and develops into a preoccupation
with food and dieting.
Bulimia nervosa is an eating disorder
characterized by binge eating followed by purging. Bulimia nervosa begins after
the dieter has broken a diet and gorged. Bulimia involves repeated episodes of
overeating, followed by vomiting, laxative use, fasting, or excessive exercise. It is
most common in women in their late teens or early 20s, and it is often accompanied by
depression and anxiety, particularly around the time of the binging. The cycle in which
the person eats to feel better, but then after eating becomes concerned about weight
gain and purges, repeats itself over and over again, often with major psychological and
physical results.
Eating disorders are in part heritable, [3]
and it is not impossible that at
least some have been selected through their evolutionary significance in coping with
food shortages. [4] Eating disorders are also related
psychological causes, including low self-esteem, perfectionism, and the perception that
one’s body weight is too high, [5] as well as to cultural
norms about body weight and eating. [6] Because eating
disorders can create profound negative health outcomes, including death, people who
suffer from them should seek treatment. This treatment is often quite effective.
These disorders in men are more common when they are participating in sports that require
a low weight such as being a runner or a wrestler. Runners who weigh less are more
likely to win races. For the wrestler there is advantage in losing a few pounds to be at
the top of a lower weight class than keeping the weight and being near the bottom of a
higher weight class. Many men with eating disorders were overweight at one time in their
lives usually as children. Men are also less likely to come forward for help because
eating disorders are seen as a female problem. Because of this, the 10% estimate is
probably low.
Although thin is in for both sexes, being too thin can be a problem for men. Often
beginning in childhood, boys who are too skinny are teased constantly and may become
adults with an obsession to bulk up. That sometimes leads to illegal steroid use.
Steroids use is one of the ways men can look like the action figures described above. At
least some sports figures such as professional wrestlers and bodybuilders use steroids
to achieve that overly muscled look. Several of these cases have been widely publicized
in recent times. Steroid use has many side effects, some of which are potentially very
serious. They include such problems as acne, testicular atrophy, reduces sperm count,
increased aggression, high blood pressure, liver damage, gynocomastia (breast
development in men) and prostate problems. And this is just a partial list.
Obesity
Although some people eat too little, eating too much is also a major problem. Obesity is a medical condition in which
so much excess body fat has accumulated in the body that it begins to have
an adverse impact on health. In addition to causing people to be
stereotyped and treated less positively by others, [7]
uncontrolled obesity leads to health problems including cardiovascular disease,
diabetes, sleep apnea, arthritis, Alzheimer’s disease, and some types of cancer. [8]
Obesity also reduces life expectancy. [9]
Obesity is determined by calculating the body mass index
(BMI), a measurement that compares one’s weight and
height. People are defined as overweight when their BMI is greater than
25 kg/m2 and as obese when it is greater than 30 kg/m2. If you know your height
and weight, you can calculate your BMI. Remember when
using the BMI, it applies to excess body fat and not well developed muscles.
People like body builders can have a high BMI and not be considered obese.
Obesity is a leading cause of death worldwide. Its prevalence is rapidly
increasing, and it is one of the most serious public health problems of the 21st
century. Although obesity is caused in part by genetics, it is increased by
overeating and a lack of physical activity. [10] [11]
There are really only two approaches to controlling weight: eat less and exercise
more. To be effective, both of these have to involve permanent lifestyle
changes. Dieting is difficult for anyone, but it is particularly difficult for
people with slow basal metabolic rates, who must cope with severe hunger to lose
weight. Although most weight loss can be maintained for about a year, very few
people are able to maintain substantial weight loss through dieting alone for
more than three years. [12] Substantial weight loss of
more than 50 pounds is typically seen only when weight loss surgery has been
performed. [13]
Weight loss surgery reduces stomach volume or bowel length, leading to earlier
satiation and reduced ability to absorb nutrients from food.
Although dieting alone does not produce a great deal of weight loss over time,
its effects are substantially improved when it is accompanied by more physical
activity. People who exercise regularly, and particularly those who combine
exercise with dieting, are less likely to be obese. [14] Exercise not only improves our waistline but also
makes us healthier overall. Exercise increases cardiovascular capacity, lowers
blood pressure, and helps improve diabetes, joint flexibility, and muscle
strength. [15] Exercise
also slows the cognitive impairments that are associated with aging. [16]
Again, changing one’s
eating habits (dieting) and/or increasing one’s time spent exercising for a
short time is not effective for long-term weight loss. The way to maintain
long-term weight loss is to permanently change your eating habits (eat fewer
calories) and exercise more (burn the same amount of calories or more than you
take in).
Because the costs of exercise are immediate but the benefits are long term, it
may be difficult for people who do not exercise to get started. It is important
to make a regular schedule, to work exercise into one’s daily activities, and to
view exercise not as a cost but as an opportunity to improve oneself. [17]
Exercising is more fun when it is done
in groups, so team exercise is recommended. [18]
A recent report found that only about one-half of Americans perform the 30
minutes of exercise 5 times a week that the Centers for Disease Control and
Prevention suggests as the minimum healthy amount. [19]
As for the other
half of Americans, they most likely are listening to the guidelines, but they
are unable to stick to the regimen. Almost half of the people who start an
exercise regimen give it up by the 6-month mark. [15]
This is a problem because
exercise has long-term benefits only if it is continued.
References
- Hoek, H. W., and van Hoeken, D.
(2003).
"Review of the prevalence and incidence of eating disorders."
International Journal of Eating Disorders. Volume 34. Number 4. 383–396
Pages.
- Patrick, L.
(2002).
"Eating disorders: A review of the literature with emphasis on
medical complications and clinical nutrition." Alternative Medicine
Review. Volume 7. Number 3. 184–202 Pages.
- Klump, K. L., Burt, S. A., McGue, M., and
Iacono, W. G.
(2007).
"Changes in genetic and environmental influences on disordered
eating across adolescence: A longitudinal twin study." Archives of
General Psychiatry. Volume 64. Number 12. 1409–1415 Pages.
- Guisinger, S.
(2008).
"Competing paradigms for anorexia nervosa." American Psychologist. Volume 63. Number 3. 199–200 Pages.
- Vohs, K. D., Voelz, Z. R., Pettit, J. W.,
Bardone, A. M., Katz, J., Abramson, L. Y., et al.
(2001).
"Perfectionism, body dissatisfaction, and self-esteem: An
interactive model of bulimic symptom development." Journal of Social and
Clinical Psychology. Volume 20. Number 4. 476–497 Pages.
- Crandall, C. S.
(1988).
"Social contagion of binge eating." Journal of Personality and Social Psychology. Volume 55. Number 4. 588–598 Pages.
- Crandall, C. S., Merman, A., and Hebl, M.
(2009).
Handbook of Prejudice, Stereotyping, and Discrimination. Chapter Anti-fat prejudice. Psychology Press. New York. 469–487 Pages. T. D. Nelson (Ed.).
- Gustafson, D., Rothenberg, E., Blennow,
K., Steen, B., and Skoog, I.
(2003).
"An 18-year follow-up of overweight and risk of Alzheimer disease."
Archives of Internal Medicine. Volume 163. Number 13. 1524–1528 Pages.
- Haslam, D. W., and James, W. P.
(2005).
"Obesity." Lancet. Volume 366. Number 9492. 197–209 Pages.
- Nestle, M., and Jacobson, M. F.
(2000).
"Halting the obesity epidemic: A public health policy approach."
Public Health Reports. Volume 115. Number 1. 12–24 Pages.
- James, W. P.
(2008).
"The fundamental drivers of the obesity epidemic." Obesity Review. Volume 9. Number Suppl. 1. 6–13 Pages.
- Miller, W. C.
(1999).
"How effective are traditional dietary and exercise interventions
for weight loss?." Medicine and Science in Sports and Exercise. Volume
31. Number 8. 1129–1134 Pages.
- Douketis, J. D., Macie C., Thabane, L.,
and Williamson, D. F.
(2005).
"Systematic review of long-term weight loss studies in obese
adults: Clinical significance and applicability to clinical practice."
International Journal of Obesity. Volume 29. Number 10. 1153–1167 Pages.
- Borer, K. T.
(2008).
"How effective is exercise in producing fat loss?." Kinesiology. Volume 40. Number 2. 126–137 Pages.
- American Heart Association
(1998).
"Statement on exercise, benefits and recommendations for physical
activity programs for all Americans." American Heart Association. Volume
94. Number 4. 857–862 Pages.
- Kramer, A. F., Erickson, K. I., and Colcombe, S. J.
(2006).
"Exercise, cognition, and the aging brain." Journal of Applied Physiology. Volume 101. Number 4. 1237–1242 Pages.
- Schomer, H., and Drake, B.
(2001).
"Physical activity and mental health." International SportMed Journal. Volume 2. Number 3. 1–9 Pages.
- Kirchhoff, A., Elliott, L., Schlichting,
J., and Chin, M.
(2008).
"Strategies for physical activity maintenance in African American
women." American Journal of Health Behavior. Volume 32. Number 5.
517–524 Pages.
- Centers for Disease Control and Prevention.
(2007).
"Prevalence of regular physical activity among adults—United
States, 2001–2005." Morbidity and Mortality Weekly Report. Volume 56.
Number 46. 1209–1212 Pages.
Perhaps the most important aspect of human experience is the process of reproduction.
Without it, none of us would be here. Successful reproduction in humans involves the
coordination of a wide variety of behaviors, including courtship, sex, household
arrangements, parenting, and child care. So one might ask, what motivates us to have sex
with another? Or another way to say it, what arouses our sexual interest and attracts us
to others?
Sex hormones play a role in our arousal. For men it’s clear that the male sex hormone
testosterone (an androgen) is the main hormone responsible for arousal. If you're a man
and your testosterone levels are normal, you’ll be motivated to have sex. Interestingly
enough, testosterone operates on an inverted U in the body. There is a maximum level of
it necessary for normal arousal. Levels below that will interfere with arousal as will
levels above that. Earlier we talked about steroid use. Steroids are artificial
androgens and thus function in the body just like testosterone. Because they
artificially increase testosterone, sex drive is likely to be decreased.
The picture with women is not as clear. We know that testosterone levels affect sex drive
in women much as they do in men. In women it’s produced in the adrenals and the ovaries.
The role of estrogens is not clear. Some postmenopausal women (estrogen levels drop
dramatically with menopause) report a decrease in sex drive while others report an
increase or no change.
Oxytocin is another hormone that has received a lot of attention. Sometimes called the
love hormone, it promotes closeness and bonding. Levels increase when we are engaging in
sexual activity. Touching the skin is particularly likely to increase oxytocin levels as
does having an orgasm. High levels of oxytocin are at least partially responsible for
the closeness we feel towards our partners particularly following orgasm.
In your brain, parts of the hypothalamus, several cortical areas, and the limbic system
have been implicated in arousal The neurotransmitter dopamine is also involved in
arousal and pleasure. Your brain generates sexual fantasies. Many if not most people are
aroused by fantasizing about sexual acts or partners.
Our senses are also involved with touch and vision playing the largest roles. Touch is
the number one sense in arousal. The skin is the largest sense organ in the body and
many parts are very sensitive to arousal. Some are biologically based such as the
genitals, the mouth including the lips and tongue, the inner thighs, the breasts and the
nape of the neck. We refer to these as primary erogenous zones.
Others are learned through classical conditioning.
Learned ones are called secondary erogenous zones. Any part of
the body can become one if it is stimulated during a sexual act. For example, if you
constantly stroke your partner’s eyebrows during sex, eventually you’ll be able to
arouse your partner just by stroking the eyebrows.
Both men and women are visually stimulated. The ability of men to be visually stimulated
has never been in doubt. Most commercially available pornography is oriented towards a
male audience. It hasn’t always been so clear for women. However, when women are asked
to view pornography and at the same time connected to physiological measures of arousal,
it shows they are in fact aroused even if they say they aren’t. Visual arousal is
affected by one’s culture. For example, in American culture, a glimpse of female breasts
is considered arousing; however, that is not true in all cultures.
There are three other factors we should consider—attractiveness, proximity, and
similarity. Another’s attractiveness may be the first factor that draws us to them.
Psychologists define attractiveness by facial symmetry and lack of any observable
defects. Most humans regardless of culture will respond to these. Evolution plays a role
here. Facial symmetry and lack of observable defects communicate a healthy person
capable of successful breeding. Youth also conveys this message. Then culture takes
over. What we consider attractive in terms of dress or adornments are cultural issues
and learned. They also change with the times. For example, it’s fashionable to sport one
or more tattoos in the early part of the 21st century. No so long before that, it was
not considered attractive and probably will be that way again. Take a look at the
couples around you. Most people are pretty evenly matched on the attractiveness scale.
They look like they go together. It’s not common to see a really attractive person with
a much less attractive person.
We are also likely to be attracted to someone we come into regular contact with. That’s
the proximity factor. Another way to say it is our partner choices are limited by where
we live, work and play. And finally, we are more likely to be attracted to people with
whom we have something in common—the similarity factor. Contrary to popular opinion,
opposites do not attract. It should make sense if you think about it for a minute. If
you were truly opposites how would you spend your time? Common interests are what make
relationships last.
So what attracts us to another? Our brain and hormones, our senses, our attractiveness,
similarity, and proximity. If these are in harmony, we are likely to be highly motivated
to pursue sexual activity.
Men and women vary in their interest in sex. Men show a more consistent interest in sex,
whereas the sexual desires of women are more likely to vary over time. [1] Men fantasize about sex
more often than do women, and their fantasies are more physical and less intimate. [2] Men are also
more willing than women to have casual, and their standards for sex partners are
lower. [3] [4] However, women
are more likely to put the brakes on sexual behavior. When men are asked by a desirable
partner if they are interested in having casual sex, they are more likely to say yes
than when the roles are reversed.
Sex differences in sexual interest probably occur in part as a result of the evolutionary
predispositions of men and women, and this interpretation is bolstered by the finding
that gender differences in sexual interest are observed cross-culturally. [5] Evolutionarily, women should be more
selective than men in their choices of sex partners because they must invest more time
in bearing and nurturing their children than do men (most men do help out, of course,
but women simply do more. [6] Because they do not need to invest a lot of
time in child rearing, men may be evolutionarily predisposed to be more willing and
desiring of having sex with many different partners and may be less selective in their
choice of mates. Women, on the other hand, because they must invest substantial effort
in raising each child, should be more selective.
The Many Varieties of Sexual Behavior
Sex researchers have found that sexual behavior varies widely, not only between
men and women but within each
sex. [7] [8]
About a quarter of women report having a low sexual desire, and about 1% of
people report feeling no sexual attraction
whatsoever. [9] [10] [11]
There are also people who experience hyperactive sexual drives. For about 3% to
6% of the population (mainly men), the sex drive is so strong
that it dominates life experience and may lead to hyperactive sexual desire
disorder. [12]
There is also variety in sexual orientation, which is the direction of our sexual desire toward people of the
opposite sex, people of the same sex, or people of both sexes. The vast
majority of human beings have a heterosexual orientation—their sexual desire is
focused toward members of the opposite sex. A smaller minority is primarily
homosexual (i.e., they have sexual desire for members of their own sex). Between
3% and 4% of men are gay, and between 1% and 2% of women are lesbian. Another 1%
of the population reports being bisexual (having desires for both sexes). The
love and sexual lives of homosexuals are not different from those of
heterosexuals, except that they choose to have sex with someone that has the
same set of sexual equipment. As with heterosexuals, some gays and lesbians are
celibate, some are promiscuous, but most are in committed, long-term
relationships. [13]
Although homosexuality has been practiced as long as records of human behavior
have been kept, and occurs in many animals at least as frequently as it does in
humans, cultures nevertheless vary substantially in their attitudes toward it.
In Western societies such as the United States and Europe, attitudes are
becoming progressively more tolerant of homosexuality, but it remains
unacceptable in many other parts of the world. The American Psychiatric
Association does not consider homosexuality to be a “mental illness,” although
it did so until 1973. Because prejudice against gays and lesbians can lead to
experiences of ostracism, depression, and even
suicide, [14] these improved
attitudes can benefit the everyday lives of gays, lesbians, and bisexuals.
Historically sexologists looked at the three orientations as mutually exclusive.
First it was about with whom you had sex. You could tell who was in which
category by whom they had sex with. Then it was about with whom you fall in
love. You could tell who was in which category by whom they fell in love with.
Not all people neatly fit into one of these three and even those that do can
change categories over time. Sexuality is more fluid than static. People can
identify themselves as belonging to one category, say heterosexual, and still
have sex with members of their own sex. Others can identify themselves as
homosexual now but later can change to heterosexual or bisexual. Called sexual
fluidity, it is more commonly seen in women but can be seen in both sexes. It is
probably more common in women because there is a greater societal prohibition
against men having sex with men than women having sex with women. Because there
is less of a societal prohibition against women, they are more likely to freely
explore their sexuality than men.
The idea of sexual fluidity closely matches the Kinsey scale of sexual orientation as depicted above.
0—Exclusively heterosexual with no homosexual
1—Predominantly heterosexual, only incidentally homosexual
2—Predominantly heterosexual, but more than incidentally homosexual
3—Equally heterosexual and homosexual
4—Predominantly homosexual, but more than incidentally heterosexual
5—Predominantly homosexual, only incidentally heterosexual
6—Exclusively homosexual
Whether sexual orientation is driven more by nature or by nurture has received a
great deal of research attention, and research has found that sexual orientation
is primarily biological. [15]
Areas of the hypothalamus are different in homosexual men, as well as in animals
with homosexual tendencies, than they are in heterosexual members of the
species, and these differences are in directions such that gay men are more
similar to women than are straight
men. [16] [17] [18]
Twin studies also support the idea that there is a genetic component to sexual
orientation. Among male identical twins, 52% of those with a gay brother also
reported homosexuality, whereas the rate in fraternal twins was just
22%. [19] [20] There is also
evidence that sexual orientation is influenced by exposure and responses to sex
hormones. [21] [22]
References
- Baumeister, R. F.
(2000).
"Gender differences in erotic plasticity: The female sex drive as
socially flexible and responsive." Psychological Bulletin. Volume 126.
Number 3. 347–374 Pages.
- Leitenberg, H., and Henning, K.
(1995).
"Sexual fantasy." Psychological Bulletin. Volume 117. Number 3. 469–496 Pages.
- Petersen, J. L., and Hyde, J. S.
(2010).
"A meta-analytic review of research on gender differences in
sexuality, 1993–2007." Psychological Bulletin. Volume 136. Number 1.
21–38 Pages.
- Saad, G., Eba, A., and Sejean, R.
(2009).
"Sex differences when searching for a mate: A process-tracing
approach." Journal of Behavioral Decision Making. Volume 22. Number 2.
171–190 Pages.
- Buss, D. M.
(1989).
"Sex differences in human mate preferences: Evolutionary hypotheses
tested in 37 cultures." Behavioral and Brain Sciences. Volume 12.
Number 1. 1–49 Pages.
- Buss, D., and Kenrick, D.
(1998).
Handbook of Social Psychology, Vol 2.
Chapter Evolutionary social psychology. McGraw-Hill. Boston. Edition 4.
982–1026 Pages. D. T. Gilbert, S. T. Fiske, and G. Lindzey (Eds.).
- Kinsey, A. C., Pomeroy, W. B., and Martin, C. E.
(1998).
Sexual Behavior in the Human Male. Indiana University Press. Bloomington. Original work published 1948.
- Kinsey, A. C.
(1998).
Sexual Behavior in the Human Female. Indiana University Press. Bloomington. Original work published 1953.
- Bogaert, A.
(2004).
"Asexuality: Prevalence and associated factors in a national
probability sample." Journal of Sex Research. Volume 41. Number 3.
279–287 Pages.
- Feldhaus-Dahir, M.
(2009).
"The causes and prevalence of hypoactive sexual desire disorder:
Part I." Urologic Nursing. Volume 29. Number 4. 259–263 Pages.
- West, S. L., D’Aloisio, A. A., Agans, R. P.,
Kalsbeek, W. D., Borisov, N. N., and Thorp, J. M.
(2008).
"Prevalence of low sexual desire and hypoactive sexual desire
disorder in a nationally representative sample of US women." Archives of
Internal Medicine. Volume 168. Number 13. 1441–1449 Pages.
- Kingston, D. A., and Firestone, P.
(2008).
"Problematic hypersexuality: A review of conceptualization and
diagnosis." Sexual Addictions and Compulsivity. Volume 15. Number 4.
284–310 Pages.
- Laumann, E. O., Gagnon, J. H., Michael, R. T., and Michaels, S.
(1994).
The Social Organization of Sexuality in the United States. University of Chicago Press. Chicago.
- Kulkin, H. S., Chauvin, E. A., and Percle,
G. A.
(2000).
"Suicide among gay and lesbian adolescents and young adults: A
review of the literature." Journal of Homosexuality. Volume 40. Number
1. 1–29 Pages.
- Mustanski, B. S., Chivers, M. L., and
Bailey, J. M.
(2002).
"A critical review of recent biological research on human sexual
orientation." Annual Review of Sex Research. Volume 13. 89–140 Pages.
- Gladue, B. A.
(1994).
"The biopsychology of sexual orientation." Current Directions in
Psychological Science. Volume 3. Number 5. 150–154 Pages.
- Lasco, M., Jordan, T., Edgar, M., Petito,
C., and Byne, W.
(2002).
"A lack of dimorphism of sex or sexual orientation in the human
anterior commissure." Brain Research. Volume 936. Number 1/2. 95–98
Pages.
- Rahman, Q., and Wilson, G. D.
(2003).
"Born gay? The psychobiology of human sexual orientation."
Personality and Individual Differences. Volume 34. Number 8. 1337–1382
Pages.
- Bailey, J., Pillard, R., Dawood, K.,
Miller, M., Farrer, L., Shruti Trivedi, L., et al.
(1999).
"A family history study of male sexual orientation using three
independent samples." Behavior Genetics. Volume 29. Number 2. 79–86
Pages.
- Pillard, R., and Bailey, J.
(1998).
"Human sexual orientation has a heritable component." Human Biology. Volume 70. Number 2. 347–365 Pages.
- Hershberger, S., and Segal, N.
(2004).
"The cognitive, behavioral, and personality profiles of a male
monozygotic triplet set discordant for sexual orientation." Archives of
Sexual Behavior. Volume 33. Number 5. 497–514 Pages.
- Williams, T., Pepitone, M., Christensen, S. E., Cooke, B. M., Huberman, A. D., Breedlove, N. J, et al.
(2000).
"Finger-length ratios and sexual orientation." Nature. Volume 404. Number 6777. 455–514 Pages.
Identical Twins Reunited after 35 Years
Paula Bernstein and Elyse Schein were identical twins who were adopted into
separate families immediately after their births in 1968. It was only at the
age of 35 that the twins were reunited and discovered how similar they were
to each other.
Paula Bernstein grew up in a happy home in suburban New York. She loved her
adopted parents and older brother and even wrote an article titled “Why I
Don’t Want to Find My Birth Mother.” Elyse’s childhood, also a happy one,
was followed by college and then film school abroad.
In 2003, 35 years after she was adopted, Elyse, acting on a whim, inquired about her
biological family at the adoption agency. The response came back: “You were born on
October 9, 1968, at 12:51 p.m., the younger of twin girls. You’ve got a twin sister,
Paula, and she’s looking for you.”
“Oh my God, I’m a twin! Can you believe this? Is
this really happening?” Elyse cried.
Elyse dialed Paula’s phone number: “It’s almost like I’m hearing my own
voice in a recorder back at me,” she said.
“It’s funny because I feel like in a way I was talking to an old, close friend I never
knew I had. . . . We had an immediate intimacy, and yet, we didn’t know each other at
all,” Paula said.
The two women met for the first time at a café for lunch and talked until
the late evening.
“We had 35 years to catch up on,” said Paula. “How do you start asking
somebody, ‘What have you been up to since we shared a womb together?’ Where
do you start?”
With each new detail revealed, the twins learned about their remarkable
similarities. They’d both gone to graduate school in film. They both loved
to write, and they had both edited their high school yearbooks. They have
similar taste in music.
“I think, you know, when we met it was undeniable that we were twins.
Looking at this person, you are able to gaze into your own eyes and see
yourself from the outside. This identical individual has the exact same DNA
and is essentially your clone. We don’t have to imagine,” Paula said.
Now they finally feel like sisters.
“But it’s perhaps even closer than sisters,” Elyse said, “Because we’re also
twins.”
The twins, who both now live in Brooklyn, combined their writing skills to write a book
called Identical Strangers about their childhoods and their
experience of discovering an identical twin in their
mid-30s. [1] [2]
You can learn more about the experiences of Paula Bernstein and Elyse Schein
by viewing the video below.
One of the most fundamental tendencies of human beings is to size up other people. We say
that Bill is fun, that Marian is adventurous, or that Frank is dishonest. When we make
these statements, we mean that we believe that these people have stable individual
characteristics—their personalities. Personality is an individual’s consistent patterns of feeling,
thinking, and behaving. [3]
The tendency to perceive personality is a fundamental part of human nature, and
a most adaptive one. If we can draw accurate generalizations about what other
people are normally like, we can predict how they will behave in the future,
and this can help us determine how they are likely to respond in different
situations. Understanding personality can also help us better understand
psychological disorders and the negative behavioral outcomes they may produce.
In short, personality matters because it guides behavior.
In this module we will consider the wide variety of personality traits found
in human beings. We’ll consider how and when personality influences our
behavior, and how well we perceive the personalities of others. We will also
consider how psychologists measure personality, and the extent to which
personality is caused by nature versus nurture. The fundamental goal of
personality psychologists is to understand what makes people different from
each other (the study of individual differences), but they also find that
people who share genes (as do Paula Bernstein and Elyse Schein) have a
remarkable similarity in personality.
Early theories assumed that personality was expressed in people’s physical appearance. One
early approach, developed by the German physician Franz Joseph Gall (1758–1828) and known
as phrenology, was based on the idea that we could measure
personality by assessing the patterns of bumps on people’s skulls (shown in the figure
below). In the Victorian age, phrenology was taken seriously, and many people promoted its
use as a source of psychological insight and self-knowledge. Machines were even developed
for helping people analyze skulls. [4] However, because careful scientific research did
not validate the predictions of the theory, phrenology has now been discredited in
contemporary psychology.
Another approach, known as somatology, championed by
the psychologist William Herbert Sheldon (1898–1977), was based on the
idea that we could determine personality from people’s body types (shown in the
figure below). Sheldon argued that people with
more body fat and a rounder physique (“endomorphs”) were more likely to be
assertive and bold, whereas thinner people (“ectomorphs”) were more likely to
be introverted and intellectual. [5] As with phrenology, scientific research did
not validate the predictions of the theory, and somatology has now been
discredited in contemporary psychology.
Another approach to detecting personality is known as physiognomy,
or the idea that it is possible to assess personality from facial characteristics. In
contrast to phrenology and somatology, for which no research support has been found,
contemporary research has found that people are able to detect some aspects of a person’s
character—for instance, whether they are gay or straight and whether they are Democrats or
Republicans—at above-chance levels by looking only at his or her face. [6] [7] [8]
Despite these results, the ability to detect personality from faces is not
guaranteed. Olivola and Todorov [9] recently studied
the ability of thousands of people to guess the personality characteristics of
hundreds of thousands of faces on the website "What's My Image?" In contrast to
the predictions of physiognomy, the researchers found that these people would
have made more accurate judgments about the strangers if they had just guessed,
using their expectations about what people in general are like, rather than
trying to use the particular facial features of individuals to help them. It
seems then that the predictions of physiognomy may also, in the end, find
little empirical support.
References
- Spilius, A.
(2007, October 27).
Identical twins reunited after 35 years. Telegraph. Retrieved from http://www.telegraph.co.uk/news/worldnews/1567542/Identical-twins-reunited-after-35-years.html.
- Kuntzman, G.
(2007, October 6).
Separated twins Paula Bernstein and Elyse Schein. The Brooklyn Paper. Retrieved from http://www.brooklynpaper.com/stories/30/39/30_39twins.html.
- John, O. P., Robins, R. W., and Pervin, L. A.
(2008).
Handbook of Personality Psychology: Theory and Research. Guilford Press. New York.
- Simpson, D.
(2005).
"Phrenology and the neurosciences: Contributions of F. J. Gall and
J. G. Spurzheim." ANZ Journal of Surgery. Volume 75. Number 6. 475–482
Pages.
- Sheldon, W.
(1940).
The Varieties of Human Physique: An Introduction to Constitutional Psychology. Harper. New York.
- Rule, N. O., and Ambady, N.
(2010).
"Democrats and Republicans can be differentiated from their faces." PLoS ONE. Volume 5. Number 1. e8733 Pages.
- Rule, N. O., Ambady, N., Adams, R. B., Jr., and
Macrae, C. N.
(2008).
"Accuracy and awareness in the perception and categorization of
male sexual orientation." Journal of Personality and Social Psychology.
Volume 95. Number 5. 1019–1028 Pages.
- Rule, N. O., Ambady, N., and Hallett, K. C.
(2009).
"Female sexual orientation is perceived accurately, rapidly, and
automatically from the face and its features." Journal of Experimental
Social Psychology. Volume 45. Number 6. 1245–1251 Pages.
- Olivola, C. Y., and Todorov, A.
(2010).
"Fooled by first impressions? Reexamining the diagnostic value of
appearance-based inferences." Journal of Experimental Social Psychology.
Volume 46. Number 2. 315–324 Pages.
Personalities are characterized in terms of traits, which are relatively enduring characteristics that influence our
behavior across many situations. Personality traits such as
introversion, friendliness, conscientiousness, honesty, and helpfulness are
important because they help explain consistencies in behavior.
The most popular way of measuring traits is by administering personality tests on which
people self-report about their own characteristics. Psychologists have investigated
hundreds of traits using the self-report approach, and this research has found many
personality traits that have important implications for behavior. You can see some examples
of the personality dimensions that have been studied by psychologists and their
implications for behavior in the following
table.
| Some Personality Traits That Predict Behavior |
|---|
| From Flat World Knowledge, Introduction to Psychology, CC-BY-NC-SA. |
| Trait |
Description |
Examples of Behaviors Exhibited by People Who Have the Trait |
| Authoritarianism [1]
|
A cluster of traits including conventionalism, superstition, toughness,
and exaggerated concerns with sexuality |
Authoritarians are more likely to be prejudiced, to conform to leaders,
and to display rigid behaviors. |
| Individualism-collectivism [2]
|
Individualism is the tendency to focus on oneself and one’s personal
goals; collectivism is the tendency to focus on one’s relations with
others. |
Individualists prefer to engage in behaviors that make them stand out
from others, whereas collectivists prefer to engage in behaviors that
emphasize their similarity to others. |
| Internal versus external locus of control [3]
|
In comparison to those with an external locus of control, people with an
internal locus of control are more likely to believe that life events are
due largely to their own efforts and personal characteristics. |
People with higher internal locus of control are happier, less
depressed, and healthier in comparison to those with an external locus of
control. |
| Need for achievement [4]
|
The desire to make significant accomplishments by mastering skills or
meeting high standards |
Those high in need for achievement select tasks that are not too
difficult to be sure they will succeed in them. |
| Need for cognition [5]
|
The extent to which people engage in and enjoy effortful cognitive
activities |
People high in the need for cognition pay more attention to arguments in
ads. |
| Regulatory focus [6]
|
Refers to differences in the motivations that energize behavior, varying
from a promotion orientation (seeking out new
opportunities) to a prevention orientation
(avoiding negative outcomes) |
People with a promotion orientation are more motivated by goals of
gaining money, whereas those with prevention orientation are more
concerned about losing money. |
| Self-consciousness [7]
|
The tendency to introspect and examine one’s inner self and
feelings |
People high in self-consciousness spend more time preparing their hair
and makeup before they leave the house. |
| Self-esteem [8]
|
High self-esteem means having a positive attitude toward oneself and
one’s capabilities. |
High self-esteem is associated with a variety of positive psychological
and health outcomes. |
| Sensation seeking [9]
|
The motivation to engage in extreme and risky behaviors |
Sensation seekers are more likely to engage in risky behaviors such as
extreme and risky sports, substance abuse, unsafe sex, and crime. |
|
Example of a Trait Measure
As with intelligence tests, the utility of self-report measures of
personality depends on their reliability and construct validity. Some popular measures of
personality are not useful because they are unreliable or invalid.
Perhaps you have heard of a personality test known as the Myers-Briggs
Type Indicator (MBTI). If so, you are not alone, because the MBTI is the
most widely administered personality test in the world, given millions of
times a year to employees in thousands of companies. The MBTI categorizes
people into one of four categories on each of four dimensions: introversion versus extroversion, sensing versus intuiting, thinking versus
feeling, and judging
versus perceiving.
Although completing the MBTI can be useful for helping people think about
individual differences in personality, and for “breaking the ice” at
meetings, the measure itself is not psychologically useful because it is
not reliable or valid. People’s classifications change over time, and
scores on the MBTI do not relate to other measures of personality or to
behavior. [10]
Measures such as the MBTI remind us that it is important to
scientifically and empirically test the effectiveness of personality
tests by assessing their stability over time and their ability to predict
behavior.
One of the challenges of the trait approach to personality is that there are so many
of them: at least 18,000 English words can be used to describe people. [11] Thus a
major goal of psychologists is to take this vast number of descriptors (many of which
are similar to each other) and determine the underlying important or “core” traits
among them. [12]
The trait approach to personality was pioneered by early psychologists,
including Gordon Allport (1897–1967), Raymond
Cattell (1905–1998), and Hans Eysenck (1916–1997). Each of
these psychologists believed in the idea of the trait as the stable unit
of personality, and each attempted to provide a list or taxonomy of the
most important trait dimensions. Their approach was to provide people
with a self-report measure and then to use statistical analyses to look
for the underlying “factors” or “clusters” of traits, according to the
frequency and the co-occurrence of traits in the respondents.
Allport [13]
began his work by reducing the 18,000 traits to a set of
about 4,500 traitlike words that he organized into three levels according to their
importance. He called them “cardinal traits” (the most important traits), “central
traits” (the basic and most useful traits), and “secondary traits” (the less obvious
and less consistent ones). Cattell [14]
used a statistical procedure known as factor analysis to analyze the correlations among traits and to identify the
most important ones. On the basis of his research, he identified what he called
“source” (more important) and “surface” (less important) traits, and he developed a
measure that assesses 16 dimensions of traits based on personality adjectives taken
from everyday language.
Hans Eysenck was particularly interested in the biological and genetic
origins of personality and made an important contribution to
understanding the nature of a fundamental personality trait: extroversion versus introversion. [15] Eysenck
proposed that people who are extroverted (i.e., who enjoy socializing
with others) have lower levels of naturally occurring arousal than do
introverts (who are less likely to enjoy being with others). Eysenck
argued that extroverts have a greater desire to socialize with others to
increase their arousal level, which is naturally too low, whereas
introverts, who have naturally high arousal, do not desire to engage in
social activities because they are overly stimulating.
The fundamental work on trait dimensions conducted by Allport, Cattell,
Eysenck, and many others has led to contemporary trait models, the most
important and well-validated of which is the Five-Factor
(Big Five) Model of Personality. According to this model, there are five fundamental underlying trait dimensions
that are stable across time, cross-culturally shared, and explain a
substantial proportion of
behavior. [16] [17]
As you can see in the following table, the five dimensions (sometimes known
as the “Big Five”) are agreeableness,
conscientiousness, extroversion, neuroticism, and openness to
experience. (You can remember them using the watery acronyms
CANOE or OCEAN.)
| The Five Factors of the Five-Factor Model of Personality |
|---|
| From Flat World Knowledge, Introduction to Psychology, CC-BY-NC-SA. |
| Dimension |
Sample items |
Description |
Examples of Behaviors Predicted by the Trait |
| Openness to experience |
“I have a vivid imagination”; “I have a rich vocabulary”; “I have
excellent ideas.” |
A general appreciation for art, emotion, adventure, unusual ideas,
imagination, curiosity, and variety of experience |
Individuals who are highly open to experience tend to have
distinctive and unconventional decorations in their home. They are
also likely to have books on a wide variety of topics, a diverse
music collection, and works of art on display. |
| Conscientiousness |
“I am always prepared”; “I am exacting in my work”; “I follow a
schedule.” |
A tendency to show self-discipline, act dutifully, and aim for
achievement |
Individuals who are conscientious have a preference for planned
rather than spontaneous behavior. |
| Extroversion |
“I am the life of the party”; “I feel comfortable around people”;
“I talk to a lot of different people at parties.” |
The tendency to experience positive emotions and to seek out
stimulation and the company of others |
Extroverts enjoy being with people. In groups they like to talk,
assert themselves, and draw attention to themselves. |
| Agreeableness |
“I am interested in people”; “I feel others’ emotions”; “I make
people feel at ease.” |
A tendency to be compassionate and cooperative rather than
suspicious and antagonistic toward others; reflects individual
differences in general concern for social harmony |
Agreeable individuals value getting along with others. They are
generally considerate, friendly, generous, helpful, and willing to
compromise their interests with those of others. |
| Neuroticism |
“I am not usually relaxed”; “I get upset easily”; “I am easily
disturbed” |
The tendency to experience negative emotions, such as anger,
anxiety, or depression; sometimes called “emotional
instability” |
Those who score high in neuroticism are more likely to interpret
ordinary situations as threatening and minor frustrations as
hopelessly difficult. They may have trouble thinking clearly,
making decisions, and coping effectively with stress. |
|
A large body of research evidence has supported the five-factor model. The Big Five
dimensions seem to be cross-cultural, because the same five factors have been
identified in participants in China, Japan, Italy, Hungary, Turkey, and many other
countries. [18] The Big Five dimensions
also accurately predict behavior. For instance, a pattern of high conscientiousness,
low neuroticism, and high agreeableness predicts successful job
performance. [19]
Scores on the Big Five dimensions also predict the performance of U.S. presidents;
ratings of openness to experience are correlated positively with ratings of
presidential success, whereas ratings of agreeableness are correlated negatively with
success. [20] The Big
Five factors are also increasingly being used in helping researchers understand the
dimensions of psychological disorders such as anxiety and
depression. [21] [22]
An advantage of the five-factor approach is that it is parsimonious.
Rather than studying hundreds of traits, researchers can focus on only
five underlying dimensions. The Big Five may also capture other
dimensions that have been of interest to psychologists. For instance, the
trait dimension of need for achievement relates
to the Big Five variable of conscientiousness, and self-esteem relates to low neuroticism. On the other hand, the
Big Five factors do not seem to capture all the important dimensions of
personality. For instance, the Big Five does not capture moral behavior,
although this variable is important in many theories of personality. And
there is evidence that the Big Five factors are not exactly the same
across all cultures. [23]
Situational Influences on Personality
One challenge to the trait approach to personality is that traits may not
be as stable as we think they are. When we say that Malik is friendly, we
mean that Malik is friendly today and will be friendly tomorrow and even
next week. And we mean that Malik is friendlier than average in all
situations. But what if Malik were found to behave in a friendly way with
his family members but to be unfriendly with his fellow classmates? This
would clash with the idea that traits are stable across time and
situation.
The psychologist Walter Mischel [24] reviewed the existing
literature on traits and found that there was only a relatively low correlation
(about r = .30) between the traits that a person expressed in
one situation and those that they expressed in other situations. In one relevant
study, Hartshorne, May, Maller, and Shuttleworth [25]
examined the correlations among various behavioral indicators of honesty in children.
They also enticed children to behave either honestly or dishonestly in different
situations, for instance, by making it easy or difficult for them to steal and cheat.
The correlations among children’s behavior was low, generally less than r = .30, showing that children who steal in one situation are
not always the same children who steal in a different situation. And similar low
correlations were found in adults on other measures, including dependency,
friendliness, and conscientiousness. [26]
Psychologists have proposed two possibilities for these low correlations. One
possibility is that the natural tendency for people to see traits in others leads us
to believe that people have stable personalities when they really do not. In short,
perhaps traits are more in the heads of the people who are doing the judging than
they are in the behaviors of the people being observed. The fact that people tend to
use human personality traits, such as the Big Five, to judge animals in the same way
that they use these traits to judge humans is consistent with this
idea. [27] And this idea also fits with research
showing that people use their knowledge representation (schemas) about people to help
them interpret the world around them and that these schemas color their judgments of
others’ personalities. [28]
Research has also shown that people tend to see more traits in other
people than they do in themselves. You might be able to get a feeling for
this by taking the following short quiz. First, think about a person you
know—your mom, your roommate, or a classmate—and choose which of the
three responses on each of the four lines best describes him or her. Then
answer the questions again, but this time about yourself.
| From Flat World Knowledge, Introduction to Psychology, CC-BY-NC-SA. |
| 1. |
Energetic |
Relaxed |
Depends on the situation |
| 2. |
Skeptical |
Trusting |
Depends on the situation |
| 3. |
Quiet |
Talkative |
Depends on the situation |
| 4. |
Intense |
Calm |
Depends on the situation |
|
Richard Nisbett and his colleagues [29]
had college
students complete this same task for themselves, for their best friend, for their
father, and for the (at the time well-known) newscaster Walter Cronkite. As you can
see in the following figure, the participants chose one of the two trait terms more often
for other people than they did for themselves, and chose “depends on the situation”
more frequently for themselves than they did for the other people. These results also
suggest that people may perceive more consistent traits in others than they
should.
The human tendency to perceive traits is so strong that it is very easy
to convince people that trait descriptions of themselves are accurate.
Imagine that you had completed a personality test and the psychologist
administering the measure gave you this description of your
personality:
You have a great need for other people to like and admire you. You have a
tendency to be critical of yourself. You have a great deal of unused
capacity, which you have not turned to your advantage. While you have
some personality weaknesses, you are generally able to compensate for
them. Disciplined and self-controlled outside, you tend to be worrisome
and insecure inside. At times you have serious doubts as to whether you
have made the right decision or done the right thing.
I would imagine that you might find that it described you. You probably
do criticize yourself at least sometimes, and you probably do sometimes
worry about things. The problem is that you would most likely have found
some truth in a personality description that was the opposite. Could this
description fit you too?
You frequently stand up for your own opinions even if it means that
others may judge you negatively. You have a tendency to find the
positives in your own behavior. You work to the fullest extent of your
capabilities. You have few personality weaknesses, but some may show up
under stress. You sometimes confide in others that you are concerned or
worried, but inside you maintain discipline and self-control. You
generally believe that you have made the right decision and done the
right thing.
The Barnum effect refers to the
observation that people tend to believe in descriptions of their
personality that supposedly are descriptive of them but could in fact
describe almost anyone. The Barnum effect helps us understand why
many people believe in astrology, horoscopes, fortune-telling, palm
reading, tarot card reading, and even some personality tests. People are
likely to accept descriptions of their personality if they think that
they have been written for them, even though they cannot distinguish
their own tarot card or horoscope readings from those of others at better
than chance levels. [30] Again, people
seem to believe in traits more than they should.
A second way that psychologists responded to Mischel’s findings was by
searching even more carefully for the existence of traits. One insight
was that the relationship between a trait and a behavior is less than
perfect because people can express their traits in different
ways. [31]
People high in extroversion, for instance, may become teachers, salesmen,
actors, or even criminals. Although the behaviors are very different,
they nevertheless all fit with the meaning of the underlying trait.
Psychologists also found that, because people do behave differently in different
situations, personality will only predict behavior when the behaviors are aggregated
or averaged across different situations. We might not be able to use the personality
trait of openness to experience to determine what Saul will do on Friday night, but
we can use it to predict what he will do over the next year in a variety of
situations. When many measurements of behavior are combined, there is much clearer
evidence for the stability of traits and for the effects of traits on
behavior. [32] [33]
Taken together, these findings make a very important point about personality, which
is that it not only comes from inside us but is also shaped by the situations that we
are exposed to. Personality is derived from our interactions with and observations of
others, from our interpretations of those interactions and observations, and from our
choices of which social situations we prefer to enter or
avoid. [34] In fact, behaviorists such as B. F.
Skinner explain personality entirely in terms of the environmental influences that
the person has experienced. Because we are profoundly influenced by the situations
that we are exposed to, our behavior does change from situation to situation, making
personality less stable than we might expect. And yet personality does matter—we can,
in many cases, use personality measures to predict behavior across situations.
learn by doing
You can try completing a self-report measure of
personality (a short form of the Five-Factor Personality Test). There are
120 questions, and it should take you about 15 to 20 minutes to complete. You will
receive feedback about your personality after you have finished the test.
did I get this
Ben is usually animated and talkative when he is with his girlfriend, but
he is often quiet and reserved at home. He actively participates in many
classroom discussions but frequently seems reluctant to talk with friends
at the campus coffee shop.
Most of Janet’s friends and co-workers would describe her as being quiet
and reserved.
Doug considers John to be a very honest person. In fact, in a psychology
class in which the consistency of traits was being discussed, Doug cited
his friend as an example of consistency.
Gina was informed by a professional palm reader: “You generally
communicate openly with others, but you have certain dark secrets that
even your closest friends could never guess.”
References
- Adorno, T. W., Frenkel-Brunswik, E., Levinson, D. J., and Sanford, R. N.
(1950).
The Authoritarian Personality. Harper. New York.
- Triandis, H.
(1989).
"The self and social behavior in differing cultural contexts." Psychological Review. Volume 96. Number 3. 506–520 Pages.
- Rotter, J.
(1966).
"Generalized expectancies of internal versus external locus of
control of reinforcement." Psychological Monographs. Volume 80. Number
1. 1–28 Pages.
- McClelland, D. C.
(1958).
Motives in Fantasy, Action and Society. Chapter Methods of measuring human motivation. D. Van Nostrand. Princeton, NJ. 12–13 Pages. J. W. Atkinson (Ed.).
- Cacioppo, J. T., and Petty, R. E.
(1982).
"The need for cognition." Journal of Personality and Social Psychology. Volume 42. Number 1. 116–131 Pages.
- Shah, J., Higgins, T., andand Friedman, R. S.
(1998).
"Performance incentives and means: How regulatory focus influences
goal attainment." Journal of Personality and Social Psychology. Volume
74. Number 2. 285–293 Pages.
- Fenigstein, A., Scheier, M. F., and Buss,
A. H.
(1975).
"Public and private self-consciousness: Assessment and theory."
Journal of Consulting and Clinical Psychology. Volume 43. Number 4.
522–527 Pages.
- Rosenberg, M.
(1965).
Society and the Adolescent Self-Image. Princeton University Press. Princeton, NJ.
- Zuckerman, M.
(2007).
Sensation Seeking and Risky Behavior. American Psychological Association. Washington, DC.
- Hunsley, J., Lee, C. M., and Wood, J. M.
(2003).
Science and Pseudoscience in Clinical Psychology.
Chapter Controversial and questionable assessment techniques. Guilford
Press. New York. 39–76 Pages. S. O. Lilienfeld, S. J. Lynn, and J. M.
Lohr (Eds.).
- Allport, G. W., and Odbert, H.
(1936).
Trait-Names: A Psycho-Lexical Study. No. 211. Psychological Review Monographs. Princeton, NJ.
- John, O. P., Angleitner, A., and Ostendorf, F.
(1988).
"The lexical approach to personality: A historical review of trait
taxonomic research." European Journal of Personality. Volume 2. Number
3. 171–203 Pages.
- Allport, G. W.
(1937).
Personality: A Psychological Interpretation. Holt, Rinehart, and Winston. New York.
- Cattell, R. B.
(1990).
Handbook of Personality: Theory and Research. Chapter Advances in Cattellian personality theory. Guilford Press. New York. 101–110 Pages. L. A. Pervin (Ed.).
- Eysenck, H.
(1998).
Dimensions of Personality. Transaction. Piscataway, NJ.
- Costa, P. T., Jr., and McCrae, R. R.
(1992).
Revised NEO Personality Inventory (NEO-PI-R) and NEO Five-Factor Inventory (NEO-FFI) Manual. Psychological Assessment Resources. Odessa, FL.
- Goldberg, L. R.
(1982).
Advances in Personality Assessment, Vol. 1.
Chapter From ace to zombie: Some explorations in the language of
personality. Lawrence Erlbaum Associates. Hillsdale, NJ. 203–234 Pages.
C. D. Spielberger and J. N. Butcher (Eds.).
- Triandis, H. C., and Suh, E. M.
(2002).
"Cultural influences on personality." Annual Review of Psychology. Volume 53. Number 1. 133–160 Pages.
- Tett, R. P., Jackson, D. N., and Rothstein, M.
(1991).
"Personality measures as predictors of job performance: A
meta-analytic review." Personnel Psychology. Volume 44. Number 4.
703–742 Pages.
- Rubenzer, S. J., Faschingbauer, T. R., and
Ones, D. S.
(2000).
"Assessing the U.S. presidents using the revised NEO Personality
Inventory." Assessment. Volume 7. Number 4. 403–420 Pages.
- Rubenzer, S. J., Faschingbauer, T. R., and Ones, D. S.
(2010).
"Borderline personality disorder and DSM-5." Journal of Psychiatric Practice. Volume 16. Number 3. 143–154 Pages.
- Saulsman, L. M., and Page, A. C.
(2004).
"The five-factor model and personality disorder empirical
literature: A meta-analytic review." Clinical Psychology Review. Volume
23. Number 8. 1055–1085 Pages.
- Cheung, F. M., and Leung, K.
(1998).
"Indigenous personality measures: Chinese examples." Journal of
Cross-Cultural Psychology. Volume 29. Number 1. 233–248 Pages.
- Mischel, W.
(1968).
Personality and Assessment. Wiley. New York.
- Hartshorne, H., May, M. A., Maller, J. B., Shuttleworth, F. K.
(1928).
Studies in the Nature of Character. Macmillan. New York.
- Bem, D. J., and Allen, A.
(1974).
"On predicting some of the people some of the time: The search for
cross-situational consistencies in behavior." Psychological Review.
Volume 81. Number 6. 506–520 Pages.
- Gosling, S. D.
(2001).
"From mice to men: What can we learn about personality from animal
research." Psychological Bulletin. Volume 127. Number 1. 45–86 Pages.
- Fiske, S. T., and Taylor, S. E.
(2007).
Social Cognition, from Brains to Culture. McGraw-Hill. New York.
- Nisbett, R. E., Caputo, C., Legant, P., and
Marecek, J.
(1973).
"Behavior as seen by the actor and as seen by the observer."
Journal of Personality and Social Psychology. Volume 27. Number 2.
154–164 Pages.
- Hines, T.
(2003).
Pseudoscience and the Paranormal. Prometheus Books. Amherst, NY.
- Mischel, W., and Shoda, Y.
(2008).
Handbook of Personality Psychology: Theory and Research.
Chapter Toward a unified theory of personality: Integrating
dispositions and processing dynamics within the cognitive-affective
processing system. Guilford Press. New York. Edition 3. 208–241 Pages.
O. P. John, R. W. Robins, and L. A. Pervin (Eds.).
- Roberts, B. W., and DelVecchio, W. F.
(2000).
"The rank-order consistency of personality traits from childhood to
old age: A quantitative review of longitudinal studies." Psychological
Bulletin. Volume 126. Number 1. 3–25 Pages.
- Srivastava, S., John, O. P., Gosling, S.
D., and Potter, J.
(2003).
"Development of personality in early and middle adulthood: Set like
plaster or persistent change?." Journal of Personality and Social
Psychology. Volume 85. Number 5. 1041–1053 Pages.
- Bandura, A.
(1986).
Social Foundations of Thought and Action: A Social Cognitive
Theory. Prentice Hall. Englewood Cliffs, NJ.
One of the most important measures of personality (which is used primarily to
assess deviations from a “normal” or “average” personality) is the Minnesota Multiphasic Personality Inventory (MMPI), a test used around the world to identify personality and
psychological disorders. [1] The MMPI was developed by
creating a list of more than 1,000 true-false questions and choosing those that
best differentiated patients with different psychological disorders from other
people. The current version (the MMPI-2) has more than 500 questions, and the
items can be combined into a large number of different subscales. Some of the
most important of these are shown in the table
below,
but there are also scales that represent family problems, work attitudes, and
many other dimensions. The MMPI also has questions that are designed to detect
the tendency of the respondents to lie, fake, or simply not answer the
questions.
| Some of the Major Subscales of the MMPI |
|---|
| From Flat World Knowledge, Introduction to Psychology, CC-BY-NC-SA. |
| Abbreviation |
Description |
What Is Measured |
No. of Items |
| Hs |
Hypochondriasis |
Concern with bodily symptoms |
32 |
| D |
Depression |
Depressive symptoms |
57 |
| Hy |
Hysteria |
Awareness of problems and vulnerabilities |
60 |
| Pd |
Psychopathic deviate |
Conflict, struggle, anger, respect for society’s rules |
50 |
| MF |
Masculinity/femininity |
Stereotypical masculine or feminine interests/behaviors |
56 |
| Pa |
Paranoia |
Level of trust, suspiciousness, sensitivity |
40 |
| Pt |
Psychasthenia |
Worry, anxiety, tension, doubts, obsessiveness |
48 |
| Sc |
Schizophrenia |
Odd thinking and social alienation |
78 |
| Ma |
Hypomania |
Level of excitability |
46 |
| Si |
Social introversion |
People orientation |
69 |
|
To interpret the results, the clinician looks at the pattern of responses
across the different subscales and makes a diagnosis about the potential
psychological problems facing the patient. Although clinicians prefer to
interpret the patterns themselves, a variety of research has demonstrated that
computers can often interpret the results as well as can
clinicians. [2] [3]
Extensive research has found that the MMPI-2 can accurately predict which of
many different psychological disorders a person suffers
from. [4]
One potential problem with a measure like the MMPI is that it asks people to
consciously report on their inner experiences. But much of our personality is
determined by unconscious processes of which we are only vaguely or not at all
aware. Projective measures are measures of personality in which unstructured stimuli, such as inkblots,
drawings of social situations, or incomplete sentences, are shown to
participants, who are asked to freely list what comes to mind as they think
about the stimuli. Experts then score the responses for clues to
personality. The proposed advantage of these tests is that they are more
indirect—they allow the respondent to freely express whatever comes to mind,
including perhaps the contents of their unconscious experiences.
One commonly used projective test is the Rorschach Inkblot
Test, developed by the Swiss psychiatrist Hermann
Rorschach (1884–1922). The Rorschach Inkblot
Test is a projective measure of personality in which
the respondent indicates his or her thoughts about a series of 10
symmetrical inkblots (shown in the figure below). The Rorschach is
administered millions of time every year. The participants are asked to respond
to the inkblots, and their responses are systematically scored in terms of
what, where, and why they saw what they saw. For example, people who focus on
the details of the inkblots may have obsessive-compulsive tendencies, whereas
those who talk about sex or aggression may have sexual or aggressive
problems.
Another frequently administered projective test is the Thematic Apperception Test (TAT), developed by the
psychologist Henry Murray (1893–1988). The Thematic Apperception Test
(TAT) is a projective measure of personality in which the
respondent is asked to create stories about sketches of ambiguous
situations, most of them of people, either alone or with others (shown
in the figure below). The sketches are shown to individuals, who are asked to
tell a story about what is happening in the picture. The TAT assumes that
people may be unwilling or unable to admit their true feelings when asked
directly but that these feelings will show up in the stories about the
pictures. Trained coders read the stories and use them to develop a personality
profile of the respondent.
Other popular projective tests include those that ask the respondent to draw
pictures, such as the Draw-A-Person
test, [5] and free association tests in
which the respondent quickly responds with the first word that comes to mind
when the examiner says a test word. Another approach is the use of
“anatomically correct” dolls that feature representations of the male and
female genitals. Investigators allow children to play with the dolls and then
try to determine on the basis of the play if the children may have been
sexually abused.
The advantage of projective tests is that they are less direct, allowing people to avoid
using their defense mechanisms and therefore show their “true” personality. The idea is
that when people view ambiguous stimuli, they will describe them according to the aspects
of personality that are most important to them and therefore bypass some of the limitations
of more conscious responding.
Despite their widespread use, however, the empirical evidence supporting the use of
projective tests is mixed. [3] [6] The
reliability of the measures is low because people often produce very different responses on
different occasions. The construct validity of the measures is also suspect because there
are very few consistent associations between Rorschach scores or TAT scores and most
personality traits. The projective tests often fail to distinguish between people with
psychological disorders and those without or to correlate with other measures of
personality or with behavior.
In sum, projective tests are more useful as icebreakers to get to know a person
better, to make the person feel comfortable, and to get some ideas about topics
that may be of importance to that person than for accurately diagnosing
personality.
learn by doing
Instructions: For each of the following test items,
indicate whether it is an example of a self-report personality inventory
or a projective test of personality.
References
- Tellegen, A., Ben-Porath, Y. S., McNulty, J. L., Arbisi, P. A., Graham, J. R., and Kaemmer, B.
(2003).
The MMPI-2 Restructured Clinical Scales: Development, Validation, and Interpretation. University of Minnesota Press. Minneapolis.
- Garb, H. N.
(1998).
Studying the Clinician: Judgment Research and Psychological Assessment. Chapter Computers and judgment. American Psychological Association. Washington, DC. 207–229 Pages. H. N. Garb (Ed.).
- Karon, B. P.
(2000).
"The clinical interpretation of the Thematic Apperception Test,
Rorschach, and other clinical data: A reexamination of statistical
versus clinical prediction." Professional Psychology: Research and
Practice. Volume 31. Number 2. 230–233 Pages.
- Graham, J. R.
(2006).
MMPI-2: Assessing Personality and Psychopathology. Oxford University Press. New York. Edition 4.
- Machover, K.
(1949).
Personality Projection in the Drawing of the Human Figure: A Method of
Personality Investigation. Chapter Personality projection in the drawing of the human figure (a method of
personality investigation). Charles C. Thomas. Springfield, IL. 3–32 Pages. K. Machover (Ed.).
- Wood, J. M., Nezworski, M. T., Lilienfeld, S. O., and Garb, H. N.
(2003).
What’s Wrong with the Rorschach? Science Confronts the Controversial Inkblot Test. Jossey-Bass. San Francisco.
One trait that has been studied in thousands of studies is leadership, the ability to direct or inspire others to achieve
goals. Trait theories of leadership are theories
based on the idea that some people are simply “natural leaders” because they
possess personality characteristics that make them
effective. [1] Consider Steve
Jobs, the founder of the Apple Inc., shown below. What characteristics do you
think he possessed that allowed him to create such a strong company, even
though many similar companies failed?
Research has found that being intelligent is an important characteristic of leaders as long
as the leader communicates to others in a way that is easily understood by his or her
followers. [2] [3] Other research has found that people with
good social skills, such as the ability to accurately perceive the needs and goals of the
group members and to communicate with others, also tend to make good leaders. [4]
Because so many characteristics seem to be related to leader skills, some researchers have
attempted to account for leadership not in terms of individual traits, but rather in terms
of a package of traits that successful leaders seem to have. Some have considered this in
terms of charisma. [5] [6]
Charismatic leaders are leaders who are
enthusiastic, committed, and self-confident; who tend to talk about the importance of
group goals at a broad level; and who make personal sacrifices for the group.
Charismatic leaders express views that support and validate existing group norms but that
also contain a vision of what the group could or should be. Charismatic leaders use their
referent power to motivate, uplift, and inspire others. And research has found a positive
relationship between a leader’s charisma and effective leadership
performance. [7]
Another trait-based approach to leadership is based on the idea that leaders take either
transactional or transformational
leadership styles with their subordinates. [8] [9]
Transactional leaders are the more regular leaders, who work with
their subordinates to help them understand what is required of them and to get the job
done. Transformational leaders, on the other hand, are more like
charismatic leaders—they have a vision of where the group is going, and attempt to
stimulate and inspire their workers to move beyond their present status and to create a new
and better future.
Despite the fact that there appear to be at least some personality traits that
relate to leadership ability, the most important approaches to understanding
leadership take into consideration both the personality characteristics of the
leader as well as the situation in which the leader is operating. In some cases
the situation itself is important. For instance, you might remember that
President George W. Bush’s ratings as a leader increased dramatically after the
September 11, 2001, terrorist attacks on the World Trade Center. This is a
classic example of how a situation can influence the perceptions of a leader’s
skill.
In still other cases, different types of leaders may perform differently in
different situations. Leaders whose personalities lead them to be more focused
on fostering harmonious social relationships among the members of the group,
for instance, are particularly effective in situations in which the group is
already functioning well and yet it is important to keep the group members
engaged in the task and committed to the group outcomes. Leaders who are more
task-oriented and directive, on the other hand, are more effective when the
group is not functioning well and needs a firm hand to guide
it. [10]
References
- Zaccaro, S. J.
(2007).
"Trait-based perspectives of leadership." American Psychologist. Volume 62. Number 1. 6–16 Pages.
- Simonton, D. K.
(1994).
Greatness: Who Makes History and Why. Guilford Press. New York.
- Simonton, D. K.
(1995).
International Handbook of Personality and Intelligence. Perspectives on Individual Differences.
Chapter Personality and intellectual predictors of leadership. Plenum.
New York. 739–757 Pages. D. H. Saklofske and M. Zeidner (Eds.).
- Kenny, D. A., and Zaccaro, S. J.
(1983).
"An estimate of variance due to traits in leadership." Journal of
Applied Psychology. Volume 68. Number 4. 678–685 Pages.
- Sternberg, R., and Lubart, T.
(1995).
Defying the Crowd: Cultivating Creativity in a Culture of Conformity. Free Press. New York.
- Sternberg, R. J.
(2002).
Multiple Intelligences and Leadership.
Chapter Successful intelligence: A new approach to leadership. Lawrence
Erlbaum Associates. Mahwah, NJ. 9–28 Pages. R. E. Riggio, S. E. Murphy,
and F. J. Pirozzolo (Eds.).
- Simonton, D. K.
(1988).
"Presidential style: Personality, biography and performance."
Journal of Personality and Social Psychology. Volume 55. Number 6.
928–936 Pages.
- Bass, B. M.
(1999).
"Current developments in transformational leadership: Research and
applications." Psychologist-Manager Journal. Volume 3. Number 1. 5–21
Pages.
- Pieterse, A. N., Van Knippenberg, D.,
Schippers, M., and Stam, D.
(2010).
"Transformational and transactional leadership and innovative
behavior: The moderating role of psychological empowerment." Journal of
Organizational Behavior. Volume 31. Number 4. 609–623 Pages.
- Ayman, R., Chemers, M. M., and Fiedler, F.
(1995).
"The contingency model of leadership effectiveness: Its level of
analysis." Leadership Quarterly. Volume 6. Number 2. 147–167 Pages.
Although measures such as the Big Five and the Minnesota Multiphasic
Personality Inventory (MMPI) are able to effectively assess personality, they
do not say much about where personality comes from. In this section we will
consider two major theories of the origin of personality: psychodynamic and humanistic approaches.
One of the most important psychological approaches to understanding personality
is based on the theorizing of the Austrian physician and psychologist Sigmund
Freud (1856–1939), who founded what today is known as the psychodynamic approach to understanding personality. Many
people know about Freud because his work has had a huge impact on our everyday
thinking about psychology, and the psychodynamic approach is one of the most
important approaches to psychological
therapy, [1] [2]
Freud is probably the best known of all psychologists, in part because of his
impressive observation and analyses of personality (there are 24 volumes of his
writings). As is true of all theories, many of Freud’s ingenious ideas have
turned out to be at least partially incorrect, and yet other aspects of his
theories are still influencing psychology.
Freud was influenced by the work of the French neurologist Jean-Martin
Charcot (1825–1893), who had been interviewing patients (almost
all women) who were experiencing what was at the time known as hysteria. Although it is no longer used to describe a
psychological disorder, hysteria at the time referred to a set of personality
and physical symptoms that included chronic pain, fainting, seizures, and
paralysis.
Charcot could find no biological reason for the symptoms. For instance, some
women experienced a loss of feeling in their hands and yet not in their arms,
and this seemed impossible given that the nerves in the arms are the same that
are in the hands. Charcot was experimenting with the use of hypnosis, and he
and Freud found that under hypnosis many of the hysterical patients reported
having experienced a traumatic sexual experience, such as sexual abuse, as
children. [3]
Freud and Charcot also found that during hypnosis the remembering of the trauma
was often accompanied by an outpouring of emotion, known as catharsis, and that following the catharsis the patient’s symptoms
were frequently reduced in severity. These observations led Freud and Charcot
to conclude that these disorders were caused by psychological rather than
physiological factors.
Freud used the observations that he and Charcot had made to develop his theory
regarding the sources of personality and behavior, and his insights are central
to the fundamental themes of psychology. In terms of free will, Freud did not
believe that we were able to control our own behaviors. Rather, he believed
that all behaviors are predetermined by motivations that lie outside our
awareness, in the unconscious. These forces show themselves in our dreams, in
neurotic symptoms such as obsessions, while we are under hypnosis, and in
Freudian “slips of the tongue” in which people reveal their unconscious desires
in language. Freud argued that we rarely understand why we do what we do,
although we can make up explanations for our behaviors after the fact. For
Freud the mind was like an iceberg, with the many motivations of the
unconscious being much larger, but also out of sight, in comparison to the
consciousness of which we are
aware.
Id, Ego, and Superego
Freud proposed that the mind is divided into three components: id, ego, and superego, and
that the interactions and conflicts among the components create
personality. [4] According to Freudian theory,
the id is the component of personality that forms the basis of our
most primitive impulses. The id is entirely
unconscious, and it drives our most important motivations, including the sexual drive
(libido) and the aggressive or destructive drive (Thanatos). According to Freud, the id is driven by the pleasure principle—the desire for immediate gratification of
our sexual and aggressive urges. The id is why we smoke cigarettes, drink alcohol,
view pornography, tell mean jokes about people, and engage in other fun or harmful
behaviors, often at the cost of doing more productive activities.
In stark contrast to the id, the superego
represents our sense of morality and oughts. The
superego tell us all the things that we shouldn’t do, or the duties and
obligations of society. The superego strives for perfection, and when we
fail to live up to its demands we feel guilty.
In contrast to the id, which is about the pleasure principle, the
function of the ego is based on the reality principle—the idea that we must delay
gratification of our basic motivations until the appropriate time with
the appropriate outlet. The ego is the largely conscious controller or decision-maker of
personality. The ego serves as the intermediary between the
desires of the id and the constraints of society contained in the
superego.
We may wish to scream, yell, or hit, and yet our ego normally tells us to
wait, reflect, and choose a more appropriate response.
Freud believed that psychological disorders, and particularly the experience of
anxiety, occur when there is conflict or imbalance among the motivations of the id,
ego, and superego. When the ego finds that the id is pressing too hard for immediate
pleasure, it attempts to correct for this problem, often through the use of defense mechanisms—unconscious psychological
strategies used to cope with anxiety and to maintain a positive self-image.
Freud believed that the defense mechanisms were essential for effective coping with
everyday life, but that any of them could be
overused.
| The Major Freudian Defense
Mechanisms |
|---|
| From Flat World Knowledge, Introduction to Psychology, CC-BY-NC-SA. |
| Defense Mechanism |
Definition |
Possible Behavioral Example |
| Displacement |
Diverting threatening impulses away from the source of the anxiety and toward a more acceptable source |
A student who is angry at her professor for a low grade lashes out at her roommate, who is a safer target of her anger. |
| Projection |
Disguising threatening impulses by attributing them to others |
A man with powerful unconscious sexual desires for women claims that women use him as a sex object. |
| Rationalization |
Generating self-justifying explanations for our negative behaviors |
A drama student convinces herself that getting the part in the play wasn’t that important after all. |
| Reaction formation |
Making unacceptable motivations appear as their exact opposite |
Jane is sexually attracted to friend Jake, but she claims in public that she intensely dislikes him. |
| Regression |
Retreating to an earlier, more childlike, and safer stage of development |
A college student who is worried about an important test begins to suck on his finger. |
| Repression (or denial) |
Pushing anxiety-arousing thoughts into the unconscious |
A person who witnesses his parents having sex is later unable to remember anything about the event. |
| Sublimation |
Channeling unacceptable sexual or aggressive desires into acceptable activities |
A person participates in sports to sublimate aggressive drives. A person creates music or art to sublimate sexual drives. |
|
The most controversial, and least scientifically valid, part of Freudian
theory is its explanations of personality development. Freud argued that
personality is developed through a series of psychosexual stages, each focusing on pleasure from a different
part of the body (shown in the table below). Freud believed that sexuality begins in
infancy, and that the appropriate resolution of each stage has
implications for later personality development.
| Freud’s Stages of Psychosexual Development |
|---|
| From Flat World Knowledge, Introduction to Psychology, CC-BY-NC-SA. |
| Stage |
Approximate ages |
Description |
| Oral |
Birth to 18 months |
Pleasure comes from the mouth in the form of sucking, biting, and chewing. |
| Anal |
18 months to 3 years |
Pleasure comes from bowel and bladder elimination and the constraints of toilet training. |
| Phallic |
3 years to 6 years |
Pleasure comes from the genitals, and the conflict is with sexual desires for the opposite-sex parent. |
| Latency |
6 years to puberty |
Sexual feelings are less important. |
| Genital |
Puberty and older |
If prior stages have been properly reached, mature sexual orientation develops. |
|
In the first of Freud’s proposed stages of psychosexual development,
which begins at birth and lasts until about 18 months of age, the focus
is on the mouth. During this oral stage, the
infant obtains sexual pleasure by sucking and drinking. Infants who
receive either too little or too much gratification become fixated or “locked” in the oral stage, and are
likely to regress to these points of fixation under stress, even as
adults. According to Freud, a child who receives too little oral
gratification (e.g., who was underfed or neglected) will become orally dependent as an adult and be likely to
manipulate others to fulfill his or her needs rather than becoming
independent. On the other hand, the child who was overfed or overly
gratified will resist growing up and try to return to the prior state of
dependency by acting helpless, demanding satisfaction from others, and
acting in a needy way.
The anal stage, lasting from about 18 months to 3 years of
age, is when children first experience psychological conflict. During this stage
children desire to experience pleasure through bowel movements, but they are also
being toilet trained to delay this gratification. Freud believed that if this toilet
training was either too harsh or too lenient, children would become fixated in the
anal stage and become likely to regress to this stage under stress as adults. If the
child received too little anal gratification (i.e., if the parents had been very
harsh about toilet training), the adult personality will be anal
retentive—stingy, with a compulsive seeking of order and tidiness. On the
other hand, if the parents had been too lenient, the anal
expulsive personality results, characterized by a lack of self-control and a
tendency toward messiness and carelessness.
The phallic stage, which lasts from age 3 to age
6 is when the penis (for boys) and clitoris (for girls) become the
primary erogenous zone for sexual pleasure. During this stage, Freud
believed that children develop a powerful but unconscious attraction for
the opposite-sex parent, as well as a desire to eliminate the same-sex
parent as a rival. Freud based his theory of sexual development in boys
(the “Oedipus complex”) on the Greek mythological character Oedipus, who
unknowingly killed his father and married his mother, and then put his
own eyes out when he learned what he had done. Freud argued that boys
will normally eventually abandon their love of the mother, and instead
identify with the father, also taking on the father’s personality
characteristics, but that boys who do not successfully resolve the
Oedipus complex will experience psychological problems later in life.
Although it was not as important in Freud’s theorizing, in girls the
phallic stage is often termed the “Electra complex,” after the Greek
character who avenged her father’s murder by killing her mother. Freud
believed that girls frequently experienced penis
envy, the sense of deprivation supposedly experienced by girls
because they do not have a penis.
The latency stage is a period of relative calm
that lasts from about 6 years to 12 years. During this time, Freud
believed that sexual impulses were repressed, leading boys and girls to
have little or no interest in members of the opposite sex.
The fifth and last stage, the genital stage,
begins about 12 years of age and lasts into adulthood. According to
Freud, sexual impulses return during this time frame, and if development
has proceeded normally to this point, the child is able to move into the
development of mature romantic relationships. But if earlier problems
have not been appropriately resolved, difficulties with establishing
intimate love attachments are likely.
References
- Roudinesco, E.
(2003).
Why Psychoanalysis?. Columbia University Press. New York.
- Taylor, E.
(2009).
The Mystery of Personality: A History of Psychodynamic Theories. Springer Science + Business Media. New York.
- Dolnick, E.
(1998).
Madness on the Couch: Blaming the Victim in the Heyday of Psychoanalysis. Simon and Schuster. New York.
- Freud, S.
(1949).
The Ego and the Id. Hogarth Press. London. (Original work published 1923).
Freudian theory was so popular that it led to a number of followers, including
many of Freud’s own students, who developed, modified, and expanded his
theories. Taken together, these approaches are known as neo-Freudian theories. The neo-Freudian theories
are theories based on Freudian principles that emphasize the role of the
unconscious and early experience in shaping personality but place less
evidence on sexuality as the primary motivating force in personality and are
more optimistic concerning the prospects for personality growth and change
in personality in adults.
Alfred Adler (1870–1937) was a follower of Freud who developed his own
interpretation of Freudian theory. Adler proposed that the primary motivation
in human personality was not sex or aggression, but rather the striving for
superiority. According to Adler, we desire to be better than others and we
accomplish this goal by creating a unique and valuable life. We may attempt to
satisfy our need for superiority through our school or professional
accomplishments, or by our enjoyment of music, athletics, or other activities
that seem important to us.
Adler believed that psychological disorders begin in early childhood. He argued
that children who are either overly nurtured or overly neglected by their
parents are later likely to develop an inferiority
complex—a psychological state in which people feel that they are not
living up to expectations, leading them to have low self-esteem, with a
tendency to try to overcompensate for the negative feelings. People with an
inferiority complex often attempt to demonstrate their superiority to others at
all costs, even if it means humiliating, dominating, or alienating them.
According to Adler, most psychological disorders result from misguided attempts
to compensate for the inferiority complex in order meet the goal of
superiority.
Carl Jung (1875–1961) was another student of Freud who developed his own
theories about personality. Jung agreed with Freud about the power of the
unconscious but felt that Freud overemphasized the importance of sexuality.
Jung argued that in addition to the personal unconscious, there was also a collective unconscious, or a collection
of shared ancestral memories. Jung believed that the collective
unconscious contains a variety of archetypes, or
cross-culturally universal symbols, which explain the similarities among people
in their emotional reactions to many stimuli. Important archetypes include the
mother, the goddess, the hero, and the mandala or circle, which Jung believed
symbolized a desire for wholeness or unity. For Jung, the underlying motivation
that guides successful personality is self-realization,
or learning about and developing the self to the fullest possible extent.
Karen Horney (1855–1952; the final syllable of her last name rhymes with “eye”), was a
German physician who applied Freudian theories to create a personality theory that she
thought was more balanced between men and women. Horney believed that parts of Freudian
theory, and particularly the ideas of the Oedipus complex and penis envy, were biased
against women. Horney argued that women’s sense of inferiority was not due to their lack of
a penis but rather to their dependency on men, a condition from which culture made it
difficult for them to break. For Horney, the underlying motivation that guides personality
development is the desire for security, the ability to develop
appropriate and supportive relationships with others.
Another important neo-Freudian was Erich Fromm (1900–1980). Fromm’s
focus was on the negative impact of technology, arguing that the increases in
its use have led people to feel increasingly isolated from others. Fromm
believed that the independence that technology brings us also creates the need
“escape from freedom,” that is, to become closer to others.
Research Focus: How the Fear of Death Causes Aggressive Behavior
Fromm believed that the primary human motivation was to escape the fear of death, and
contemporary research has shown how our concerns about dying can influence our
behavior. In this research, people have been made to confront their death by writing
about it or otherwise being reminded of it, and effects on their behavior are then
observed. In one relevant study, McGregor and colleagues [1]
demonstrated that people who are provoked may be
particularly aggressive after they have been reminded of the possibility of their own
death. The participants in the study had been selected, on the basis of prior
reporting, to have either politically liberal or politically conservative views. When
they arrived at the lab they were asked to write a short paragraph describing their
opinion of politics in the United States. In addition, half of the participants (the
mortality salient condition) were asked to “briefly
describe the emotions that the thought of your own death arouses in you” and to “jot
down, as specifically as you can, what you think will happen to you as you physically
die and once you are physically dead.” Participants in the exam
control condition also thought about a negative event, but not one associated
with a fear of death. They were instructed to “please briefly describe the emotions
that the thought of your next important exam arouses in you” and to “jot down, as
specifically as you can, what you think will happen to you as you physically take
your next exam and once you are physically taking your next exam.”
Then the participants read the essay that had supposedly just been
written by another person. (The other person did not exist, but the
participants didn’t know this until the end of the experiment.) The essay
that they read had been prepared by the experimenters to be very negative
toward politically liberal views or to be very negative toward
politically conservative views. Thus one-half of the participants were
provoked by the other person by reading a statement that strongly
conflicted with their own political beliefs, whereas the other half read
an essay in which the other person’s views supported their own (liberal
or conservative) beliefs.
At this point the participants moved on to what they thought was a
completely separate study in which they were to be tasting and giving
their impression of some foods. Furthermore, they were told that it was
necessary for the participants in the research to administer the food
samples to each other. At this point, the participants found out that the
food they were going to be sampling was spicy hot sauce and that they
were going to be administering the sauce to the very person whose essay
they had just read. In addition, the participants read some information
about the other person that indicated that he very much disliked eating
spicy food. Participants were given a taste of the hot sauce (it was
really hot!) and then instructed to place a quantity of it into a cup for
the other person to sample. Furthermore, they were told that the other
person would have to eat all the sauce.
As you can see in the figure
below,
McGregor et al. found that the participants who had not been reminded of
their own death, even if they had been insulted by the partner, did not
retaliate by giving him a lot of hot sauce to eat. On the other hand, the
participants who were both provoked by the other person and who had also
been reminded of their own death administered significantly more hot
sauce than did the participants in the other three conditions. McGregor
and colleagues [1] argued that thinking about one’s own death creates a
strong concern with maintaining one’s one cherished worldviews (in this
case our political beliefs). When we are concerned about dying we become
more motivated to defend these important beliefs from the challenges made
by others, in this case by aggressing through the hot sauce.
Strengths and Limitations of Freudian and Neo-Freudian
Approaches
Freud has probably exerted a greater impact on the public’s understanding
of personality than any other thinker, and he has also in large part
defined the field of psychology. Although Freudian psychologists no
longer talk about oral, anal, or genital “fixations,” they do continue to
believe that our childhood experiences and unconscious motivations shape
our personalities and our attachments with others, and they still make
use of psychodynamic concepts when they conduct psychological
therapy.
Nevertheless, Freud’s theories, as well as those of the neo-Freudians,
have in many cases failed to pass the test of empiricism, and as a result
they are less influential now than they have been in the past. [2]
The problems are
first, that it has proved to be difficult to rigorously test Freudian
theory because the predictions that it makes (particularly those
regarding defense mechanisms) are often vague and unfalsifiable, and
second, that the aspects of the theory that can be tested often have not
received much empirical support.
As examples, although Freud claimed that children exposed to overly harsh toilet
training would become fixated in the anal stage and thus be prone to excessive
neatness, stinginess, and stubbornness in adulthood, research has found few reliable
associations between toilet training practices and adult personality. [3] And since
the time of Freud, the need to repress sexual desires would seem to have become much
less necessary as societies have tolerated a wider variety of sexual practices. And
yet the psychological disorders that Freud thought we caused by this repression have
not decreased.
There is also little scientific support for most of the Freudian defense
mechanisms. For example, studies have failed to yield evidence for the
existence of repression. People who are exposed to traumatic experiences
in war have been found to remember their traumas only too
well. [4] Although we
may attempt to push information that is anxiety-arousing into our
unconscious, this often has the ironic effect of making us think about
the information even more strongly than if we hadn’t tried to repress
it. [5]
It is true that children remember little of their childhood experiences,
but this seems to be true of both negative as well as positive
experiences, is true for animals as well, and probably is better
explained in terms of the brain’s inability to form long-term memories
than in terms of repression. On the other hand, Freud’s important idea
that expressing or talking through one’s difficulties can be
psychologically helpful has been supported in current
research [6] and has
become a mainstay of psychological therapy.
A particular problem for testing Freudian theories is that almost
anything that conflicts with a prediction based in Freudian theory can be
explained away in terms of the use of a defense mechanism. A man who
expresses a lot of anger toward his father may be seen via Freudian
theory to be experiencing the Oedipus complex, which includes conflict
with the father. But a man who expresses no anger at all toward the
father also may be seen as experiencing the Oedipus complex by repressing
the anger. Because Freud hypothesized that either was possible, but did
not specify when repression would or would not occur, the theory is
difficult to falsify.
In terms of the important role of the unconscious, Freud seems to have
been at least in part correct. More and more research demonstrates that a
large part of everyday behavior is driven by processes that are outside
our conscious awareness. [7] And
yet, although our unconscious motivations influence every aspect of our
learning and behavior Freud probably overestimated the extent to which
these unconscious motivations are primarily sexual and aggressive.
Taken together, it is fair to say that Freudian theory, like most
psychological theories, was not entirely correct and that it has had to
be modified over time as the results of new studies have become
available. But the fundamental ideas about personality that Freud
proposed, as well as the use of talk therapy as an essential component of
therapy, are nevertheless still a major part of psychology and are used
by clinical psychologists every day.
References
- McGregor, H. A., Lieberman, J. D., Greenberg, J.,
Solomon, S., Arndt, J., Simon, L., et al.
(1998).
"Terror management and aggression: Evidence that mortality salience
motivates aggression against worldview-threatening others." Journal of
Personality and Social Psychology. Volume 74. Number 3. 590–605 Pages.
- Crews, F. C.
(1998).
Unauthorized Freud: Doubters Confront a Legend. Viking Press. New York.
- Fisher, S., and Greenberg, R. P.
(1996).
Freud Scientifically Reappraised: Testing the Theories and Therapy. Wiley. Oxford, England.
- Kihlstrom, J. F.
(1997).
"Memory, abuse, and science." American Psychologist. Volume 52. Number 9. 994–995 Pages.
- Newman, L. S., Duff, K. J., and Baumeister,
R. F.
(1997).
"A new look at defensive projection: Thought suppression,
accessibility, and biased person perception." Journal of Personality and
Social Psychology. Volume 72. Number 5. 980–1001 Pages.
- Baddeley, J. L., and Pennebaker, J. W.
(2009).
General Principles and Empirically Supported Techniques of Cognitive Behavior Therapy. Chapter Expressive writing. Wiley. Hoboken, NJ. 295–299 Pages. W. T. O’Donohue and J. E. Fisher (Eds.).
- Kihlstrom, J. F.
(1987).
"The cognitive unconscious." Science. Volume 237. Number 4821. 1445–1452 Pages.
Psychoanalytic models of personality were complemented during the 1950s and
1960s by the theories of humanistic psychologists. In
contrast to the proponents of psychoanalysis, humanists embraced the notion of
free will. Arguing that people are free to choose their own lives and make
their own decisions, humanistic psychologists focused on the underlying
motivations that they believed drove personality, focusing on the nature of the
self-concept, the set of beliefs
about who we are, and self-esteem, our positive feelings about the self.
One of the most important humanists, Abraham Maslow (1908–1970), conceptualized personality
in terms of a pyramid-shaped hierarchy of
motives.
At the base of the pyramid are the lowest-level motivations, including hunger and thirst,
and safety and belongingness. Maslow argued that only when people are able to meet the
lower-level needs are they able to move on to achieve the higher-level needs of
self-esteem, and eventually self-actualization, which is the motivation to develop our innate potential to the fullest possible
extent.
Maslow studied how successful people, including Albert Einstein, Abraham
Lincoln, Martin Luther King Jr., Helen Keller, and Mahatma Gandhi had been able
to lead such successful and productive lives. Maslow [1] believed that self-actualized people are
creative, spontaneous, and loving of themselves and others. They tend to have a
few deep friendships rather than many superficial ones, and are generally
private. He felt that these individuals do not need to conform to the opinions
of others because they are very confident and thus free to express unpopular
opinions. Self-actualized people are also likely to have peak experiences, or transcendent moments of tranquility accompanied
by a strong sense of connection with others.
Perhaps the best-known humanistic theorist is Carl Rogers (1902–1987). Rogers was positive
about human nature, viewing people as primarily moral and helpful to others, and he
believed that we can achieve our full potential for emotional fulfillment if the
self-concept is characterized by unconditional positive regard—a set of behaviors including being genuine, open to experience,
transparent, able to listen to others, and self-disclosing and empathic.
When we treat
ourselves or others with unconditional positive regard, we express understanding and
support, even while we may acknowledge failings. Unconditional positive regard allows us to
admit our fears and failures, to drop our pretenses, and yet at the same time to feel
completely accepted for what we are. The principle of unconditional positive regard has
become a foundation of psychological therapy; therapists who use it in their practice are
more effective than those who do not. [2] [3]
Although there are critiques of the humanistic psychologists (e.g., that Maslow
focused on historically productive rather than destructive personalities in his
research and thus drew overly optimistic conclusions about the capacity of
people to do good), the ideas of humanism are so powerful and optimistic that
they have continued to influence both everyday experiences as well as
psychology. Today the positive psychology movement
argues for many of these ideas, and research has documented the extent to which
thinking positively and openly has important positive consequences for our
relationships, our life satisfaction, and our psychological and physical
health. [4]
Research Focus: Self-Discrepancies, Anxiety, and Depression
Tory Higgins and his colleagues [5] [6]
studied how different aspects of the self-concept relate to personality
characteristics. These researchers focused on the types of emotional distress that we
might experience as a result of how we are currently evaluating our self-concept.
Higgins proposes that the emotions we experience are determined both by our
perceptions of how well our own behaviors meet up to the standards and goals we have
provided ourselves (our internal standards) and by our
perceptions of how others think about us (our external
standards). Furthermore, Higgins argues that different types of self-discrepancies lead to different types of negative
emotions.
In one of Higgins’s experiments, [5]
participants
were first asked to describe themselves using a self-report measure. The participants
listed 10 thoughts they believed described the kind of person they actually are; this
is the actual self-concept. Then, participants listed 10
thoughts they believed described the type of person they would “ideally like to be”
(the ideal self-concept) as well as 10 thoughts describing
the way someone else—for instance, a parent—thinks they “ought to be” (the ought self-concept).
Higgins then divided his participants into two groups. Those with low self-concept discrepancies were those who
listed similar traits on all three lists. Their ideal, ought, and actual
self-concepts were all pretty similar and so they were not considered to
be vulnerable to threats to their self-concept. The other half of the
participants, those with high self-concept
discrepancies, were those for whom the traits listed on the ideal
and ought lists were very different from those listed on the actual self
list. These participants were expected to be vulnerable to threats to the
self-concept.
Then, at a later research session, Higgins first asked people to express
their current emotions, including those related to sadness and anxiety.
After obtaining this baseline measure Higgins activated either ideal or
ought discrepancies for the participants. Participants in the ideal self-discrepancy priming condition were
asked to think about and discuss their own and their parents’ hopes and
goals for them. Participants in the ought self-priming
condition listed their own and their parents’ beliefs concerning
their duty and obligations. Then all participants again indicated their
current emotions.
As you can see in the figure below, for low self-concept
discrepancy participants, thinking about their ideal or ought selves did
not much change their emotions. For high self-concept discrepancy
participants, however, priming the ideal self-concept increased their
sadness and dejection, whereas priming the ought self-concept increased
their anxiety and agitation. These results are consistent with the idea
that discrepancies between the ideal and the actual self lead us to
experience sadness, dissatisfaction, and other depression-related
emotions, whereas discrepancies between the actual and ought self are
more likely to lead to fear, worry, tension, and other anxiety-related
emotions.
One of the critical aspects of Higgins’s approach is that, as is our personality, our
feelings are also influenced both by our own behavior and by our expectations of how
other people view us. This makes it clear that even though you might not care much
about achieving in school, your failure to do well may still produce negative
emotions because you realize your parents do think it is important.
did I get this
Watch the following video of Carl Rogers discussing his beliefs and
approach to the therapeutic relationship:
References
- Maslow, A.
(1970).
Motivation and Personality. Harper. New York. Edition 2.
- Prochaska, J. O., and Norcross, J. C.
(2007).
Systems of Psychotherapy: A Transtheoretical Analysis. Brookes/Cole. Pacific Grove, CA. Edition 6.
- Yalom, I.
(1995).
A Way of Being. Chapter Introduction. Houghton Mifflin. New York. C. Rogers (Ed.).
- Seligman, M. E. P., and Csikszentmihalyi, M.
(2000).
"Positive psychology: A introduction." American Psychologist. Volume 55. Number 1. 5–14 Pages.
- Higgins, E. T., Bond, R. N., Klein, R., and
Strauman, T.
(1986).
"Self-discrepancies and emotional vulnerability: How magnitude,
accessibility, and type of discrepancy influence affect." Journal of
Personality and Social Psychology. Volume 51. Number 1. 5–15 Pages.
- Strauman, T. J., and Higgins, E. T.
(1988).
"Self-discrepancies as predictors of vulnerability to distinct
syndromes of chronic emotional distress." Journal of Personality. Volume
56. Number 4. 685–707 Pages.
One question that is exceedingly important for the study of personality
concerns the extent to which it is the result of nature or nurture. If nature
is more important, then our personalities will form early in our lives and will
be difficult to change later. If nurture is more important, however, then our
experiences are likely to be particularly important, and we may be able to
flexibly alter our personalities over time. In this section we will see that
the personality traits of humans and animals are determined in large part by
their genetic makeup, and thus it is no surprise that identical twins Paula
Bernstein and Elyse Schein turned out to be very similar even though they had
been raised separately. But we will also see that genetics does not determine
everything.
In the nucleus of each cell in your body are 23 pairs of chromosomes. One of each pair comes from your father, and the other
comes from your mother. The chromosomes are made up of strands of the molecule
DNA (deoxyribonucleic acid), and the DNA is grouped
into segments known as genes. A gene is the basic biological unit that transmits
characteristics from one generation to the next. Human cells have about
25,000 genes.
The genes of different members of the same species are almost identical. The
DNA in your genes, for instance, is about 99.9% the same as the DNA in my genes
and in the DNA of every other human being. These common genetic structures lead
members of the same species to be born with a variety of behaviors that come
naturally to them and that define the characteristics of the species. These
abilities and characteristics are known as instincts—complex inborn patterns of behaviors that help ensure
survival and reproduction. [1]
Different animals have different instincts. Birds naturally build nests, dogs
are naturally loyal to their human caretakers, and humans instinctively learn
to walk and to speak and understand language.
But the strength of different traits and behaviors also varies within species.
Rabbits are naturally fearful, but some are more fearful than others; some dogs
are more loyal than others to their caretakers; and some humans learn to speak
and write better than others do. These differences are determined in part by
the small amount (in humans, the 0.1%) of the differences in genes among the
members of the species.
Personality is not determined by any single gene, but rather by the actions of many genes
working together. There is no “IQ gene” that determines intelligence, and there is no “good
marriage partner gene” that makes a person a particularly good marriage bet. Furthermore,
even working together, genes are not so powerful that they can control or create our
personality. Some genes tend to increase a given characteristic and others work to decrease
that same characteristic—the complex relationship among the various genes, as well as a
variety of random factors, produces the final outcome. Furthermore, genetic factors always
work with environmental factors to create personality. Having a given pattern of genes
doesn’t necessarily mean that a particular trait will develop, because some traits might
occur only in some environments. For example, a person may have a genetic variant that is
known to increase his or her risk for developing emphysema from smoking. But if that person
never smokes, then emphysema most likely will not develop.
Perhaps the most direct way to study the role of genetics in personality is to
selectively breed animals for the trait of interest. In this approach the
scientist chooses the animals that most strongly express the personality
characteristics of interest and breeds these animals with each other. If the
selective breeding creates offspring with even stronger traits, then we can
assume that the trait has genetic origins. In this manner, scientists have
studied the role of genetics in how worms respond to stimuli, how fish develop
courtship rituals, how rats differ in play, and how pigs differ in their
responses to stress.
Although selective breeding studies can be informative, they are clearly not
useful for studying humans. For this psychologists rely on behavioral genetics—a variety of research
techniques that scientists use to learn about the genetic and environmental
influences on human behavior by comparing the traits of biologically and
nonbiologically related family
members. [2] Behavioral genetics is based
on the results of family studies, twin studies, and adoptive studies.
A family study
starts with one person who has a trait of interest—for
instance, a developmental disorder such as autism—and examines the
individual’s family tree to determine the extent to which other members of
the family also have the trait. The presence of the trait in
first-degree relatives (parents, siblings, and children) is compared to the
prevalence of the trait in second-degree relatives (aunts, uncles,
grandchildren, grandparents, and nephews or nieces) and in more distant family
members. The scientists then analyze the patterns of the trait in the family
members to see the extent to which it is shared by closer and more distant
relatives.
Although family studies can reveal whether a trait runs in a family, it cannot
explain why. In a twin study, researchers study the personality characteristics of twins. Twin
studies rely on the fact that identical (or monozygotic) twins have essentially
the same set of genes, while fraternal (or dizygotic) twins have, on average, a
half-identical set. The idea is that if the twins are raised in the same
household, then the twins will be influenced by their environments to an equal
degree, and this influence will be pretty much equal for identical and
fraternal twins. In other words, if environmental factors are the same, then
the only factor that can make identical twins more similar than fraternal twins
is their greater genetic similarity.
In a twin study, the data from many pairs of twins are
collected and the rates of similarity for identical and fraternal pairs are
compared. A correlation coefficient is calculated that assesses the
extent to which the trait for one twin is associated with the trait in the
other twin. Twin studies divide the influence of nature and nurture into three
parts:
-
Heritability (i.e., genetic influence) is indicated
when the correlation coefficient for identical twins exceeds that for
fraternal twins, indicating that shared DNA is an important determinant of
personality.
-
Shared environment determinants are indicated when
the correlation coefficients for identical and fraternal twins are greater
than zero and also very similar. These correlations indicate that both twins
are having experiences in the family that make them alike.
-
Nonshared environment is indicated when identical
twins do not have similar traits. These influences refer to experiences that
are not accounted for either by heritability or by shared environmental
factors. Nonshared environmental factors are the experiences that make
individuals within the same family less alike. If a
parent treats one child more affectionately than another, and as a
consequence this child ends up with higher self-esteem, the parenting in
this case is a nonshared environmental factor.
In the typical twin study, all three sources of influence are operating
simultaneously, and it is possible to determine the relative importance of each
type.
An adoption study
compares biologically related people, including twins, who
have been reared either separately or apart. Evidence for genetic
influence on a trait is found when children who have been adopted show traits
that are more similar to those of their biological parents than to those of
their adoptive parents. Evidence for environmental influence is found when the
adoptee is more like his or her adoptive parents than the biological
parents.
The results of family, twin, and adoption studies are combined to get a better
idea of the influence of genetics and environment on traits of interest.
The
table below presents data on the correlations and heritability estimates for a
variety of traits based on the results of behavioral genetics
studies. [3]
If you look in the second column, you will see the observed correlations for the traits
between identical twins who have been raised together in the same house by the same
parents. This column represents the pure effects of genetics, in the sense that
environmental differences have been controlled to be a small as possible. You can see that
these correlations are higher for some traits than for others. Fingerprint patterns are
very highly determined by our genetics (r = .96), whereas the Big
Five trait dimensions have a heritability of 40% to 50%.
You can also see from the table that, overall, there is more influence of
nature than of parents. Identical twins, even when they are raised in separate
households by different parents (column 4), turn out to be quite similar in
personality, and are more similar than fraternal twins who are raised in
separate households (column 5). These results show that genetics has a strong
influence on personality, and helps explain why Elyse and Paula were so similar
when they finally met.
Despite the overall role of genetics, you can see from the table that the correlations
between identical twins (column 2) and heritability estimates for most traits (column 6)
are substantially less than 1.00, showing that the environment also plays an important role
in personality. [4] For instance, for sexual orientation, the estimates of heritability vary
from 18% to 39% of the total across studies, suggesting that 61% to 82% of the total
influence is due to environment.
You might at first think that parents would have a strong influence on the personalities of
their children, but this would be incorrect. As you can see by looking in column 7 of the
table,
research finds that the influence of shared environment (i.e., the effects of parents or
other caretakers) plays little or no role in adult personality. [5] Shared environment does influence the personality
and behavior of young children, but this influence decreases rapidly as the child grows
older. By the time we reach adulthood, the impact of shared environment on our
personalities is weak at best. [6] What this means is that,
although parents must provide a nourishing and stimulating environment for children, no
matter how hard they try they are not likely to be able to turn their children into
geniuses or into professional athletes, nor will they be able to turn them into
criminals.
If parents are not providing the environmental influences on the child, then
what is? The last column in the table
above,
the influence of nonshared environment, represents whatever is “left over”
after removing the effects of genetics and parents. You can see that these
factors—the largely unknown things that happen to us that make us different
from other people—often have the largest influence on personality.
learn by doing
Identical twins Gerald Levey and Mark Newman were separated at birth and raised in
different homes. When reunited at age 31, they discovered, among many other
similarities, that they both volunteered as firefighters.
Because Gerry and Mark are identical twins and share nearly 100% of their genes,
their fingerprints are almost identical, as genetic factors contribute about 96% to
the development of ridges on fingertips. In comparison, Gerry’s and Mark’s scores on
the Big Five personality traits should be less similar. Researchers have broken down
the contributions to personality development into the following four factors:
- Heritability
- Nonshared environmental factors
- Shared environmental factors
- Error
Note: Error refers to the influence on personality development that
cannot as yet be identified and is attributed to errors in testing and
measurement procedures. This error percentage should decrease and other
factors should increase as methodology improves.
Nonshared influences can occur because individual children tend to elicit different
responses from their parents for a variety of reasons—their temperament, gender, or
birth order, or accidents and illnesses they may have had. This explains why, despite
Gerry’s and Mark’s remarkable similarities in personality, they also display some
unique differences.
References
- Tinbergen, N.
(1951).
The Study of Instinct. Clarendon Press. Oxford, England. Edition 1.
- Baker, C.
(2004 ).
Behavioral genetics: An introduction to how
genes and environments interact through development to shape differences
in mood, personality, and intelligence. Retrieved from http://www.aaas.org/spp/bgenes/Intro.pdf.
- Bouchard, T. J., Lykken, D. T., McGue, M.,
Segal, N. L., and Tellegen, A.
(1990).
"Sources of human psychological differences: The Minnesota study of
twins reared apart." Science. Volume 250. Number 4978. 223–228 Pages.
- Turkheimer, E., and Waldron, M.
(2000).
"Nonshared environment: A theoretical, methodological, and
quantitative review." Psychological Bulletin. Volume 126. Number 1.
78–108 Pages.
- Harris, J. R.
(2006).
No Two Alike: Human Nature and Human Individuality. Norton. New York.
- Roberts, B. W., and DelVecchio, W. F.
(2000).
"The rank-order consistency of personality traits from childhood to
old age: A quantitative review of longitudinal studies." Psychological
Bulletin. Volume 126. Number 1. 3–25 Pages.
In addition to the use of behavioral genetics, our understanding of the role of
biology in personality recently has been dramatically increased through the use
of molecular genetics, which is the
study of which genes are associated with which personality
traits. [1] [2]
These advances have occurred as a result of new knowledge about the structure
of human DNA made possible through the Human Genome Project and related work
that has identified the genes in the human body. [3] Molecular
genetics researchers have also developed new techniques that allow them to find
the locations of genes within chromosomes and to identify the effects those
genes have when activated or deactivated.
One approach that can be used in animals, usually in laboratory mice, is the
knockout study. In this approach the researchers use
specialized techniques to remove or modify the influence of a gene in a line of
“knockout” mice. [4] The
researchers harvest embryonic stem cells from mouse embryos and then modify the
DNA of the cells. The DNA is created such that the action of certain genes will
be eliminated or “knocked out.” The cells are then injected into the embryos of
other mice that are implanted into the uteruses of living female mice. When
these animals are born, they are studied to see whether their behavior differs
from a control group of normal animals. Research has found that removing or
changing genes in mice can affect their anxiety, aggression, learning, and
socialization patterns.
In humans, a molecular genetics study normally begins with the collection of a
DNA sample from the participants in the study, usually by taking some cells
from the inner surface of the cheek. In the lab, the DNA is extracted from the
sampled cells and is combined with a solution containing a marker for the
particular genes of interest as well as a fluorescent dye. If the gene is
present in the DNA of the individual, then the solution will bind to that gene
and activate the dye. The more the gene is expressed, the stronger the
reaction.
In one common approach, DNA is collected from people who have a particular
personality characteristic and also from people who do not. The DNA of the two
groups is compared to see which genes differ between them. These studies are
now able to compare thousands of genes at the same time. Research using
molecular genetics has found genes associated with a variety of personality
traits including
novelty-seeking, [5]
attention-deficit/hyperactivity
disorder, [6] and
smoking
behavior. [7]
Reviewing the Literature: Is Our Genetics Our Destiny?
Over the past two decades scientists have made substantial progress in
understanding the important role of genetics in behavior. Behavioral
genetics studies have found that, for most traits, genetics is more
important than parental influence. And molecular genetics studies have
begun to pinpoint the particular genes that are causing these
differences. The results of these studies might lead you to believe that
your destiny is determined by your genes, but this would be a mistaken
assumption.
For one, the results of all research must be interpreted carefully. Over
time we will learn even more about the role of genetics, and our
conclusions about its influence will likely change. Current research in
the area of behavioral genetics is often criticized for making
assumptions about how researchers categorize identical and fraternal
twins, about whether twins are in fact treated in the same way by their
parents, about whether twins are representative of children more
generally, and about many other issues. Although these critiques may not
change the overall conclusions, it must be kept in mind that these
findings are relatively new and will certainly be updated with
time. [8]
Furthermore, it is important to reiterate that although genetics is
important, and although we are learning more every day about its role in
many personality variables, genetics does not determine everything. In
fact, the major influence on personality is nonshared environmental
influences, which include all the things that occur to us that make us
unique individuals. These differences include variability in brain
structure, nutrition, education, upbringing, and even interactions among
the genes themselves.
The genetic differences that exist at birth may be either amplified or
diminished over time through environmental factors. The brains and bodies
of identical twins are not exactly the same, and they become even more
different as they grow up. As a result, even genetically identical twins
have distinct personalities, resulting in large part from environmental
effects.
Because these nonshared environmental differences are nonsystematic and largely
accidental or random, it will be difficult to ever determine exactly what will happen
to a child as he or she grows up. Although we do inherit our genes, we do not inherit
personality in any fixed sense. The effect of our genes on our behavior is entirely
dependent on the context of our life as it unfolds day to day. No one can say, on the
basis of our genes, what kind of human being we will turn out to be or what we will
do in life.
References
- Goldsmith, H., Gernsbacher, M. A., Crabbe, J., Dawson, G., Gottesman, I. I., Hewitt, J., et al.
(2003).
"Research psychologists’ roles in the genetic revolution." American Psychologist. Volume 58. Number 4. 318–319 Pages.
- Strachan, T., and Read, A. P.
(1999).
Human Molecular Genetics. Wiley-Liss. New York. Edition 2. Retrieved from http://www.ncbi.nlm.nih.gov/books/NBK7569/.
- U.S. Department of Energy Office of Science, Office of Biological and Environmental Research, Human Genome Program.
(2010 ).
Human Genome Project information. Retrieved from http://www.ornl.gov/sci/techresources/Human_Genome/home.shtml.
- Crusio, W. E., Goldowitz, D., Holmes, A., and Wolfer, D.
(2009).
"Standards for the publication of mouse mutant studies." Genes, Brain and Behavior. Volume 8. Number 1. 1–4 Pages.
- Ekelund, J., Lichtermann, D., Järvelin, M.
R., and Peltonen, L.
(1999).
"Association between novelty seeking and the type 4 dopamine
receptor gene in a large Finnish cohort sample." American Journal of
Psychiatry. Volume 156. Number 9. 1453–1455 Pages.
- Waldman, I. D., and Gizer, I. R.
(2006).
"The genetics of attention deficit hyperactivity disorder."
Clinical Psychology Review. Volume 26. Number 4. 396–432 Pages.
- Plomin, R.
(2000).
"Behavioural genetics in the 21st century." International Journal
of Behavioral Development. Volume 24. Number 1. 30–34 Pages.
Binge Drinking and the Death of a Homecoming Queen
Sam Spady, a 19-year-old student at Colorado State University, had been a
homecoming queen, a class president, a captain of the cheerleading team, and
an honor student in high school. But despite her outstanding credentials and
her hopes and plans for the future, Sam Spady died on September 5, 2004,
after a night of binge drinking with her friends.
Sam had attended a number of different parties on the Saturday night that
she died, celebrating the CSU football game against the University of
Colorado–Boulder. When she passed out, after consuming 30 to 40 beers and
shots over the evening, her friends left her alone in an empty room in a
fraternity house to sleep it off. The next morning a member of the
fraternity found her dead. [1]
Sam is one of an estimated 1,700 college students between the ages of 18 and
24 who die from alcohol-related injuries each year. These deaths come from
motor vehicle crashes, assaults, and overdosing as a result of binge
drinking. [2]
“Nobody is immune,” said Sam’s father. “She was a smart kid, and she was a
good kid. And if it could happen to her, it could happen to anybody.”
Despite efforts at alcohol education, Pastor Reza Zadeh, a former CSU
student, says little has changed in the drinking culture since Sam’s death:
“People still feel invincible. The bars still have 25-cent shot night and
two-for-ones and no cover for girls.” [1]
Sam’s parents have created a foundation in her memory, dedicated to
informing people, particularly college students, about the dangers of binge
drinking and to helping them resist the peer pressure that brings it on.
You can learn about the signs of alcohol poisoning at the Sam Spady Foundation.
The subdiscipline of psychology discussed in this unit reflects the highest
level of explanation that we will consider. This topic, known as social psychology, is defined as
the scientific study of how we feel about, think about,
and behave toward the other people around us, and how those people influence
our thoughts, feelings, and behavior.
The subject matter of social psychology is our everyday
interactions with
people, including the social groups to which we belong.
Social-psychological questions include why we are often helpful to other
people but at other
times are unfriendly or aggressive; why we sometimes conform to
the behaviors
of others but at other times we assert our independence; and
what
factors help groups work together in effective and productive
ways. A fundamental principle of social
psychology is that, although we may not always be aware of it,
our cognitions,
emotions, and behaviors are substantially influenced by the social situation, or the
people with whom we are interacting.
In this module we introduce the principles of social cognition—the part of
human thinking that helps us understand and predict the behavior of
ourselves and others—and consider the ways that our judgments about
other people guide our behaviors toward them. We explore how we form
impressions of other people, and what makes us like or dislike them. We also
see how our attitudes—our enduring evaluations of people or things—influence,
and are influenced by, our behavior.
Then we consider the social psychology of interpersonal relationships,
including the behaviors of altruism, aggression, and
conformity. We will see that humans have a natural
tendency to help each other but that we may also become aggressive if we feel
we are being threatened. And we will see how social norms, the accepted
beliefs about what we do or what we should do in particular social
situations (such as the norm of binge drinking common on many college
campuses) influence our behavior. Finally, we consider the social
psychology of social groups, with a particular focus on the conditions that
limit and potentially increase productive group performance and
decision-making.
The principles of social psychology can help us understand tragic events such
as the death of Sam Spady. Many people might blame the tragedy on Sam herself,
asking, for instance, “Why did she drink so much?” or “Why didn’t she say no?”
As we will see in this unit, research conducted by social psychologists
shows that the poor decisions Sam made on the night she died may have been due
less to her own personal weaknesses or deficits than to her desires to fit in
with and be accepted by the others around her—desires that in her case led to a
disastrous outcome.
One important aspect of social cognition involves forming impressions of other
people. Making these judgments quickly and accurately helps us guide our
behavior to interact appropriately with the people we know. If we can figure
out why our roommate is angry at us, we can react to resolve the problem; if we
can determine how to motivate the people in our group to work harder on a
project, then the project might be better.
Our initial judgments of others are based in large part on what we see.
The physical features of other people, particularly their gender, race, age,
and physical attractiveness, are very salient, and we often focus our
attention on these
dimensions. [3] [4]
Although it may seem inappropriate or shallow to admit
it, many people are often strongly influenced by the physical
attractiveness of others, and in some situations, physical
attractiveness is the most important determinant of our
initial liking for others. [5]
Infants who are only a year old prefer to look at faces that adults
consider to be attractive than at unattractive
faces. [6]
Evolutionary psychologists have argued that our belief that “what is
beautiful is also good” may be because we use attractiveness as a cue for
health; people whom we find more attractive may also, evolutionarily,
have been healthier. [7]
One indicator of health is youth. Leslie Zebrowitz and her colleagues [8] [9]
extensively studied the tendency for both men and women to prefer people whose faces
have characteristics similar to those of babies. These features include large, round,
and widely spaced eyes, a small nose and chin, prominent cheekbones, and a large
forehead. People who have baby faces (both men and women) are seen as more attractive
than people who do not.
Another indicator of health is symmetry. People are more attracted to faces that are
more symmetrical and this may be
due in part to the perception that people with symmetrical faces are healthier. [10]
Although you might think that we would prefer faces that are unusual or
unique, the opposite is true. Langlois and Roggman [11]
showed college students the faces of men and women. They were
composites of the average of 2, 4, 8, 16, or 32 faces. The
researchers found that the more faces that were averaged into the
stimulus, the more attractive it was judged. Again, our liking for
average faces may be because they appear healthier.
Although preferences for youthful, symmetrical, and average faces have
been observed cross-culturally, and thus appear to be common human
preferences, different cultures may also have unique beliefs about what
is attractive. In modern Western cultures, “thin is in,” and people
prefer those who have little excess
fat. [12] The need to be thin
to be attractive is particularly strong for women in contemporary
society, and the desire to maintain a low body weight can lead to low
self-esteem, eating disorders, and other unhealthy behaviors. However,
the norm of thinness has not always been in place; the preference for
women with slender, masculine, and athletic looks has become stronger
over the past 50 years. In contrast to the relatively universal
preferences for youth, symmetry, and averageness, other cultures do not
show such a strong propensity for thinness. [13]
learn by doing
The “what is beautiful is good” stereotype refers to the common belief
that attractive people possess other desirable characteristics such as
being more friendly, likable, and fun to be around compared to less
attractive individuals. Snyder, Tanke, and Berscheid [14]
conducted a study on the behavioral confirmation of this
stereotype involving physical attractiveness.
In the study, male subjects participated in a getting-acquainted session with females
over the telephone. Prior to the conversation, the male subjects were shown a
photograph of either a physically attractive or physically unattractive female—not
the photograph of the actual person they talked to. This was the experimental
manipulation intended to create different beliefs and expectations on the part of the
male subjects about their interaction partner. The conversations were tape recorded,
and each participant’s conversational behavior was analyzed by naive observer judges
for evidence of behavioral confirmation. Specifically, the judges rated how friendly,
likable, and sociable the male and female interaction partners were during the
conversation. The results revealed evidence of behavioral confirmation, indicating
that a self-fulfilling prophecy had occurred.
References
- Sidman, J.
(2006, June 26).
A college student’s death may help save lives. USA Today. Retrieved from http://www.usatoday.com/news/health/2006-06-26-spady -binge-drinking_x.htm.
- National Institute on Alcohol Abuse and Alcoholism.
(2010).
Statistical snapshot of college drinking. Retrieved from http://www.niaaa.nih.gov/AboutNIAAA/NIAAASponsoredPrograms/StatisticalSnapshotCollegeDrinking.htm.
- Schneider, D. J.
(2004).
The Psychology of Stereotyping. Guilford Press. New York.
- Zebrowitz, L. A., and Montepare, J.
(2006).
Evolution and Social Psychology. Chapter
The ecological approach to person perception: Evolutionary roots and
contemporary offshoots. Psychosocial Press. Madison, CT. 81–113 Pages.
M. Schaller, J. A. Simpson, and D. T. Kenrick (Eds.).
- Walster, E., Aronson, V., Abrahams, D., and
Rottmann, L.
(1966).
"Importance of physical attractiveness in dating behavior." Journal
of Personality and Social Psychology. Volume 4. Number 5. 508–516
Pages.
- Langlois, J. H., Ritter, J. M., Roggman, L.
A., and Vaughn, L. S.
(1991).
"Facial diversity and infant preferences for attractive faces."
Developmental Psychology. Volume 27. Number 1. 79–84 Pages.
- Zebrowitz, L. A., Fellous, J.-M.,
Mignault, A., and Andreoletti, C.
(2003).
"Trait impressions as overgeneralized responses to adaptively
significant facial qualities: Evidence from connectionist modeling."
Personality and Social Psychology Review. Volume 7. Number 3. 194–215
Pages.
- Zebrowitz, L. A.
(1996).
Stereotypes and Stereotyping. Chapter
Physical appearance as a basis of stereotyping. Guilford Press. New
York. 79–120 Pages. C. N. Macrae, C. Stangor, and M. Hewstone (Eds.).
- Zebrowitz, L. A., Luevano, V. X., Bronstad, P. M., and Aharon, I.
(2009).
"Neural activation to babyfaced men matches activation to babies." Social Neuroscience. Volume 4. Number 1. 1–10 Pages.
- Rhodes, G., Zebrowitz, L. A., Clark, A., Kalick, S. M., Hightower, A., and McKay, R.
(2001).
"Do facial averageness and symmetry signal health?." Evolution and Human Behavior. Volume 22. Number 1. 31–46 Pages.
- Langlois, J. H., and Roggman, L. A.
(1990).
"Attractive faces are only average." Psychological Science. Volume 1. Number 2. 115–121 Pages.
- Crandall, C. S., Merman, A., and Hebl, M.
(2009).
Handbook of Prejudice, Stereotyping, and Discrimination. Chapter Anti-fat prejudice. Psychology Press. New York. 469–487 Pages. T. D. Nelson (Ed.).
- Sugiyama, L. S.
(2005).
The Handbook of Evolutionary Psychology. Chapter Physical attractiveness in adaptationist perspective. Wiley. Hoboken, NJ. 292–343 Pages. D. M. Buss (Ed.).
- Snyder, M., Tanke, E. D., and Berscheid, E.
(1977).
"Social perception and interpersonal behavior: On the
self-fulfilling nature of social stereotypes." Journal of Personality
and Social Psychology. Volume 35. Number 9. 656–666 Pages.
We frequently use people’s appearances to form our judgments about them and to determine
our responses to them. The tendency to attribute personality
characteristics to people on the basis of their external appearance or their social
group memberships is known as stereotyping. Our stereotypes about physically attractive people lead
us to see them as more dominant, sexually warm, mentally healthy, intelligent, and
socially skilled than we perceive physically unattractive
people. [1] And our stereotypes lead us to
treat people differently—the physically attractive are given better grades on essay
exams, are more successful on job interviews, and receive lighter sentences in court
judgments than their less attractive
counterparts. [2] [3]
In addition to physical attractiveness, we also regularly stereotype
people on the basis of their gender, race, age, religion, and many other characteristics,
and these stereotypes are frequently negative. [4] This is
unfair because stereotypes are based on our preconceptions and
negative emotional responses to members of the group. Stereotyping is closely related to prejudice, the tendency
to dislike people because of their appearance or group memberships, and discrimination, negative
behaviors toward others based on prejudice. Stereotyping, prejudice, and
discrimination work together. For example, we may not vote for a gay person because
of our negative stereotypes about gays, and we may avoid people from other religions or
those with mental illness because of our prejudices.
Some stereotypes may be accurate—at least in part. Research has found, for instance, that
attractive people are actually more sociable, more popular, and less lonely than less
attractive individuals. [1] And, consistent with the
stereotype that they are “emotional,” women are, on average, more empathic and attuned
to the emotions of others than are men. [5] Group
differences in personality traits may occur in part because people act toward others on
the basis of their stereotypes. This creates a self-fulfilling
prophecy, which is when our expectations about the
personality characteristics of others lead us to behave in ways
that make those beliefs come true. If I have a stereotype that attractive
people are friendly, then I may act in a friendly way toward them.
This friendly behavior may be reciprocated by the attractive person, and if many other
people also engage in the same positive behaviors he or
she may actually become friendlier.
But even if attractive people are on average friendlier than unattractive people, not all
attractive people are friendlier than all unattractive people. And even if women are, on
average, more emotional than men, not all men are less emotional than all women. Social
psychologists believe that it is better to treat people as individuals rather than rely
on our stereotypes and prejudices, because stereotyping and prejudice are always unfair
and often inaccurate. [6] [7] Furthermore, many of our
stereotypes and prejudices exert influence out of our awareness, such that we do not even know
that we are using them.
Implicit Association Test
You might want to test your own stereotypes and prejudices by completing the
Implicit Association
Test, a measure of unconscious stereotyping.
We use our stereotypes and prejudices in part because they are easy: if we can quickly
size up people on the basis of their physical appearance, that can save us a lot of time
and effort. We may be evolutionarily disposed to stereotyping. Because our primitive
ancestors needed to accurately separate members of their own kin group from those of
others, categorizing people into “us” (the ingroup) and “them”
(the outgroup) was useful and even
necessary. [8] And the positive emotions that we experience as a result of our group
memberships—known as social
identity—can be an important and beneficial part of our everyday
experiences. [9] We may gain social identity as members of our
university, our sports teams, our religious and racial groups, and many other
groups.
But the fact that we may use our stereotypes does not mean that
we should use them. Stereotypes, prejudice, and discrimination,
whether they are consciously or unconsciously applied, make it difficult for some people
to effectively contribute to society and may create both mental and physical health
problems for them. [10]
In certain situations, people are concerned that they will be evaluated based
on a negative stereotype. For example, research has shown that the academic
performance of women and African Americans can be affected by concerns
about
confirming the expectation that they will not do
well relative to individuals who belong to stereotypically
high-performing groups. This is known as stereotype threat. In addition, European American students may feel
stereotype threat on the basketball court when competing with African Americans.
For further discussion of stereotype threat, watch the video below.
In some cases getting beyond our prejudices is required by law, as detailed in the U.S.
Civil Rights Act of 1964, the Equal Opportunity Employment Act of 1972, and the Fair
Housing Act of 1978.
There are individual differences in the degree to
which prejudice influences behavior. For example, some people are more
likely to
try to control and confront their stereotypes and
prejudices whereas others apply them
more
freely. [11] [12]
In addition, some people believe that some groups are naturally
better than others—whereas other people are more egalitarian and hold fewer
prejudices. [13] [14]
The tendency
to endorse stereotypes and prejudices and to act on them can be reduced, for instance,
through positive interactions and friendships with members of other groups, through
practice in avoiding using them, and through
education. [15]
Research Focus: Forming Judgments of People in Seconds
Research has demonstrated that people can draw very accurate conclusions about others on
the basis of very limited data. Ambady and Rosenthal [16] made videotapes of
six female and seven male graduate students while they were teaching an undergraduate
course. The courses covered diverse areas of the college curriculum, including
humanities, social sciences, and natural sciences. For each teacher, three 10-second
video clips were taken: 10 seconds from the first 10 minutes of the class, 10 seconds
from the middle of the class, and 10 seconds from the last 10 minutes of the class.
The researchers then asked nine female undergraduates to rate the clips of the teachers
on 15 dimensions including optimistic, confident, active,
enthusiastic, dominant, likable, warm, competent, and supportive. Ambady and
her colleagues then compared the ratings of the participants who had seen the teacher
for only 30 seconds with the ratings of the same instructors that had been made by
students who had spent a whole semester with the teacher, and who had rated her at the
end of the semester on scales such as “Rate the quality of the section overall” and
“Rate section leader’s performance overall.” As you can see in the following table, the ratings of
the participants and the ratings of the students were highly positively correlated.
| Accurate Perceptions in 30 Seconds |
|---|
| This table shows the Pearson
correlation coefficients between the impressions that a group of students made after
they had seen a video of instructors teaching for only 30 seconds and the teaching
ratings of the same instructors made by students who had spent a whole semester in the
class. You can see that the correlations are all positive, and that many of them are
quite large. The conclusion is that people are sometimes able to draw accurate
impressions about other people very quickly. From Flat World Knowledge, Introduction to Psychology, v1.0. Source: Ambady and Rosenthal. [16] |
| Variable |
Pearson Correlation Coefficient (r) |
| Accepting |
0.50 |
| Active |
0.77 |
| Attentive |
0.48 |
| Competent |
0.56 |
| Confident |
0.82 |
| Dominant |
0.79 |
| Empathic |
0.45 |
| Enthusiatic |
0.76 |
| Honest |
0.32 |
| Likable |
0.73 |
| (Not) anxious |
0.26 |
| Optimistic |
0.84 |
| Professional |
0.53 |
| Supportive |
0.55 |
| Warm |
0.67 |
| Overall, across all traits |
0.76 |
|
If the finding that judgments made about people in 30 seconds correlate highly with
judgments made about the same people after a whole semester surprises you, then perhaps
you may be even more surprised to hear that we do not even need that much time. Indeed,
Willis and Todorov [17] found that even a tenth of a second was
enough to make judgments that correlated highly with those same judgments made by other
people who were given several minutes to make the judgments. Other research has found
that we can make accurate judgments, for instance, about salespersons [18]
and about the sexual orientation of other
people, [19] in just a few seconds. Todorov, Mandisodza,
Goren, and Hall [20] found that people voted for political
candidates in large part on the basis of whether or not their faces, seen only for one
second, looked like faces of competent people. Taken together, this research shows that
we are well able to form initial impressions of others quickly and often quite
accurately.
References
- Langlois, J. H., Kalakanis, L., Rubenstein, A.
J., Larson, A., Hallam, M., and Smoot, M.
(2000).
"Maxims or myths of beauty? A meta-analytic and theoretical
review." Psychological Bulletin. Volume 126. Number 3. 390–423 Pages.
- Hosoda, M., Stone-Romero, E. F., and Coats,
G.
(2003).
"The effects of physical attractiveness on job-related outcomes: A
meta-analysis of experimental studies." Personnel Psychology. Volume 56.
Number 2. 431–462 Pages.
- Zebrowitz, L. A., and McDonald, S. M.
(1991).
"The impact of litigants’ baby-facedness and attractiveness on
adjudications in small claims courts." Law and Human Behavior. Volume
15. Number 6. 603–623 Pages.
- Schneider, D. J.
(2004).
The Psychology of Stereotyping. Guilford Press. New York.
- Hall, J. A., and Schmid Mast, M.
(2008).
"Are women always more interpersonally sensitive than men? Impact
of goals and content domain." Personality and Social Psychology
Bulletin. Volume 34. Number 1. 144–155 Pages.
- Fiske, S. T.
(1989).
Unintended Thought. Chapter Examining the
role of intent: Toward understanding its role in stereotyping and
prejudice. Guilford Press. New York. 253–286 Pages. J. S. Uleman and J.
A. Bargh (Eds.).
- Stangor, C.
(1995).
Stereotype Accuracy: Toward Appreciating Group Differences.
Chapter Content and application inaccuracy in social stereotyping.
American Psychological Association. Washington, DC. 275–292 Pages. Y. T.
Lee, L. J. Jussim, and C. R. McCauley (Eds.).
- Neuberg, S. L., Kenrick, D. T., and Schaller, M.
(2010).
Handbook of Social Psychology, Vol. 2.
Chapter Evolutionary social psychology. Wiley. Hoboken, NJ. Edition 5.
761–796 Pages. S. T. Fiske, D. T. Gilbert, and G. Lindzey (Eds.).
- Hogg, M. A.
(2003).
Handbook of Self and Identity. Chapter Social identity. Guilford Press. New York. 462–479 Pages. M. R. Leary and J. P. Tangney (Eds.).
- Swim, J. T., and Stangor, C.
(1998).
Prejudice: The Target’s Perspective. Academic Press. Santa Barbara, CA.
- Czopp, A. M., Monteith, M. J., and Mark, A.
Y.
(2006).
"Standing up for a change: Reducing bias through interpersonal
confrontation." Journal of Personality and Social Psychology. Volume 90.
Number 5. 784–803 Pages.
- Plant, E. A., and Devine, P. G.
(1998).
"Internal and external motivation to respond without prejudice."
Journal of Personality and Social Psychology. Volume 75. Number 3.
811–832 Pages.
- Sidanius, J., and Pratto, F.
(1998).
Social Dominance: An Intergroup Theory of Social Hierarchy and Oppression. Cambridge University Press. New York.
- Stangor, C., and Leary, S.
(2006).
"Intergroup beliefs: Investigations from the social side." Advances
in Experimental Social Psychology. Volume 38. 243–283 Pages.
- Hewstone, M.
(1996).
Stereotypes and Stereotyping. Chapter
Contact and categorization: Social psychological interventions to change
intergroup relations. Guilford Press. New York. 323–368 Pages. C. N.
Macrae, C. Stangor, and M. Hewstone (Eds.).
- Ambady, N., and Rosenthal, R.
(1993).
"Half a minute: Predicting teacher evaluations from thin slices of
nonverbal behavior and physical attractiveness." Journal of Personality
and Social Psychology. Volume 64. Number 3. 431–441 Pages.
- Willis, J., and Todorov, A.
(2006).
"First impressions: Making up your mind after a 100-ms exposure to a
face." Psychological Science. Volume 17. Number 7. 592–598 Pages.
- Ambady, N., Krabbenhoft, M. A., and Hogan,
D.
(2006).
"The 30-sec sale: Using thin-slice judgments to evaluate sales
effectiveness." Journal of Consumer Psychology. Volume 16. Number 1.
4–13 Pages.
- Ambady, N., Hallahan, M., and Conner, B.
(1999).
"Accuracy of judgments of sexual orientation from thin slices of
behavior." Journal of Personality and Social Psychology. Volume 77.
Number 3. 538–547 Pages.
- Todorov, A., Mandisodza, A. N., Goren, A., and Hall, C. C.
(2005).
"Inferences of competence from faces predict election outcomes." Science. Volume 308. Number 5728. 1623–1626 Pages.
One of the most important tasks faced by humans is to develop successful relationships
with others. These include acquaintanceships and friendships but
also the more important close relationships, which are the long-term intimate and romantic relationships that we develop
with another person—for instance, in a marriage
. [1] Because most of us
will want to enter into a close relationship at some point, and because close
relationships are evolutionarily important as they form the basis for effective child
rearing, it is useful to know what psychologists have learned about the principles of
liking and loving within them.
A major interest of social psychologists is the study of interpersonal
attraction, or what makes people like, and even love, each
other. One important factor is a perceived similarity in values and beliefs
between the partners. [2]
Similarity is important for relationships because it is more convenient
(it’s easier if both partners like to ski or go to the
movies), but also because similarity supports our values—I
can feel better about myself and my choice of activities if I see that you also enjoy
doing the same things that I do.
Liking is also enhanced by self-disclosure, the
tendency to communicate frequently, without fear of reprisal, and in an accepting
and empathetic manner. Friends are friends because we can talk to them openly
about our needs and goals, and because they listen to and respond to our
needs. [3] But self-disclosure
must be balanced. If I open up to you about the concerns that are important to me, I
expect you to do the same in return. When self-disclosure is not reciprocal, the
relationship is less likely to last.
Another important determinant of liking is proximity, or the extent to which people are physically near us. Research has
found that we are more likely to develop friendships with people who are nearby, for
instance, those who live in the same dorm that we do, and even with people who just
happen to sit nearer to us in our
classes. [4]
Proximity has its effect on liking through the principle of mere
exposure, which is the tendency to prefer stimuli (including
but not limited to people) that we have seen more frequently. Moreland and
Beach [5] studied mere exposure by having
female confederates attend a large lecture class either 0,
5, 10, or 15 times during a semester. At the end of the term, students
were shown pictures of the confederates and asked to
indicate both if they recognized them and also how much they liked them. The number of
times the confederates had attended class didn’t influence the other students’ ability
to recognize them, but it did influence their liking for them. As predicted by the mere
exposure hypothesis, students who had attended class more often were liked more as shown
in the following table.
The effect of mere exposure is powerful and occurs in a wide variety of situations.
Infants tend to smile at a photograph of someone they have seen already more than they
smile at a photograph of someone they are seeing for the first
time. [6] People prefer side-to-side reversed images of their own
faces over their normal (nonreversed) face, whereas their friends prefer their normal
face over the reversed
one. [7] This is expected on the basis of mere exposure, since people see
their own faces primarily in mirrors and thus are exposed to the reversed face more
often.
Mere exposure may well have an evolutionary basis. We have an initial fear of the
unknown, but as things become more familiar they seem more similar and safe, and thus
produce more positive feelings and seem less threatening and
dangerous. [8] In fact, research has found that stimuli tend to produce more
positive affect as they become more
familiar. [9] When the stimuli are people, there may well be an added
effect. Familiar people become more likely to be seen as part of the ingroup rather than
the outgroup, and this may lead us to like them more. Leslie Zebrowitz and her
colleagues found that we like people of our own race in part because they are perceived
as similar to us. [10]
In the most successful relationships the two people begin to see themselves as a single
unit. Arthur Aron and his colleagues [11] assessed the role of closeness in
relationships using the Inclusion of Other in the Self Scale as
shown in figure below. You might try completing the measure yourself for some different
people that you know—for instance, your family members, friends, spouse, or girlfriend
or boyfriend. The measure is simple to use and to interpret; if people see the circles
representing the self and the other as more overlapping, this means that the
relationship is close. But if they choose the circles that are less overlapping, then
the relationship is less so.
Although the closeness measure is very simple, it has been found to be strongly
correlated with people’s satisfaction with their close relationships, and of the
tendency for couples to stay
together. [12] [13] When the partners in a relationship
feel that they are close, and when they indicate that the relationship is based on
caring, warmth, acceptance and social support, we can say that the relationship is intimate. [3]
When a couple begins to take care of a household together, has children, and perhaps has
to care for elderly parents, the requirements of the relationship will
grow. As a
result, partners in close relationships increasingly turn
to each other for help in coordinating activities, remembering dates and appointments,
and accomplishing tasks. Relationships are close in part because the couple becomes
highly interdependent, relying on each other to meet important
goals. [14]
In relationships in which a positive rapport between the partners is developed and
maintained over a period of time, the partners are naturally happy with the relationship
and they become committed to it. Commitment refers to the feelings and actions that keep partners working together to
maintain the relationship [15] and is characterized by
mutual expectations that the self and the partner will be responsive to each other’s
needs. [16]
Partners who are committed to the relationship see their mates as more attractive, are
less able to imagine themselves with another partner, express less interest in other
potential mates, and are less likely to break
up. [17]
People also find relationships more satisfactory, and stay in them longer, when they feel
that the relationships are rewarding. When
the needs of either or both of the partners are not being met, the relationship is in
trouble. This is not to say that people only think about the benefits they are getting;
they will also consider the needs of the other. But over the long term, both partners
must benefit from the relationship.
Although sexual arousal and excitement are more important early on in relationships,
intimacy is also determined by sexual and romantic attraction. Indeed, intimacy is also
dependent on passion — the partners must display positive affect
toward each other. Happy couples are in positive moods when they are around each other;
they laugh with each other, express approval rather than criticism of each other’s
behaviors, and enjoy physical contact. People are happier in their relationships when
they view the other person in a positive or even an “idealized” sense, rather than a
more realistic and perhaps more negative
one. [18]
Margaret Clark and Edward Lemay [19] recently reviewed
the literature on close relationships and argued that their most important
characteristic is a sense of responsiveness. People are happy,
healthy, and likely to stay in relationships in which they are sure that they can trust
the other person to understand, validate, and care for them. It is this unconditional
giving and receiving of love that promotes the welfare of both partners and provides the
secure base that allows both partners to thrive.
References
- Hendrick, C., and Hendrick, S. S.
(2000).
Close Relationships: A Sourcebook. Sage. Thousand Oaks, CA.
- Davis, J. L., and Rusbult, C. E.
(2001).
"Attitude alignment in close relationships." Journal of Personality
and Social Psychology. Volume 81. Number 1. 65–84 Pages.
- Reis, H. T., and Aron, A.
(2008).
"Love: What is it, why does it matter, and how does it
operate?." Perspectives on Psychological Science. Volume 3. Number 1. 80–86 Pages.
- Back, M. D., Schmukle, S. C., and Egloff, B.
(2008).
"Becoming friends by chance." Psychological Science. Volume 19. Number 5. 439–440 Pages.
- Moreland, R. L., and Beach, S. R.
(1992).
"Exposure effects in the classroom: The development of affinity among
students." Journal of Experimental Social Psychology. Volume 28. Number 3. 255–276 Pages.
- Brooks-Gunn, J., and Lewis, M.
(1981).
"Infant social perception: Responses to pictures of parents and
strangers." Developmental Psychology . Volume 17. Number 5. 647–649 Pages.
- Mita, T. H., Dermer, M., and Knight, J.
(1977).
"Reversed facial images and the mere-exposure hypothesis." Journal
of Personality and Social Psychology . Volume 35. Number 8. 591–601
Pages.
- Freitas, A. L., Azizian, A., Travers, S.,
and Berry, S. A.
(2005).
"The evaluative connotation of processing fluency: Inherently
positive or
moderated by motivational context?." Journal of
Experimental Social Psychology. Volume 41. Number 6. 636–644 Pages.
- Harmon-Jones, E., and Allen, J. J. B.
(2001).
"The role of affect in the mere exposure effect: Evidence from
psychophysiological and individual differences
approaches." Personality and Social Psychology Bulletin. Volume 27.
Number 7. 889–898 Pages.
- Zebrowitz, L. A., Bronstad, P. M., and Lee, H. K.
(2007).
"The contribution of face familiarity to ingroup favoritism and
stereotyping." Social Cognition. Volume 25. Number 2. 306–338 Pages.
- Aron, A., Aron, E. N., and Smollan, D.
(1992).
"Inclusion of other in the self scale and the structure of interpersonal
closeness." Journal of Personality and Social Psychology. Volume 63. Number 4. 596–612 Pages.
- Aron, A., Aron, E. N., Tudor, M., and Nelson,
G.
(1991).
"Close relationships as including other in the self." Journal of
Personality and Social Psychology. Volume 60. Number 2. 241–253 Pages.
- Aron, A., Paris, M., and Aron, E. N.
(1995).
"Falling in love: Prospective studies of self-concept change."
Journal of Personality and Social Psychology. Volume 69. Number 6.
1102–1112 Pages.
- Berscheid, E., and Reis, H. T.
(1998).
The Handbook of Social Psychology, Vol. 1–2.
Chapter Attraction and close relationships. McGraw-Hill. New York.
Edition 4. 323–368 Pages. D. T. Gilbert, S. T. Fiske, and G. Lindzey
(Eds.).
- Rusbult, C. E., Olsen, N., Davis, J. L., and Hannon, P. A.
(2001).
Close Romantic Relationships: Maintenance and Enhancement.
Chapter Commitment and relationship maintenance mechanisms. Lawrence
Erlbaum Associates. Mahwah, NJ. 87–113 Pages. J. Harvey and A. Wenzel
(Eds.).
- Clark, M. S., and Mills, J.
(2004).
Close Relationships: Key Readings. Chapter Interpersonal attraction in exchange and communal
relationships. Taylor and Francis. Philadelphia. 245–256 Pages. H. T. Reis and C. E. Rusbult (Eds.).
- Simpson, J. A., and Harris, B. A.
(1994).
Perspectives on Close Relationships. Chapter Interpersonal attraction. Allyn and Bacon. Boston. 45–66 Pages. A. L. Weber and J. H. Harvey (Eds.).
- Murray, S. L., Holmes, J. G., and Griffin,
D. W.
(1996).
"The benefits of positive illusions: Idealization and the
construction of
satisfaction in close relationships." Journal of
Personality and Social Psychology. Volume 70. Number 1. 79–98 Pages.
- Clark, M. S., and Lemay, E. P., Jr.
(1994).
Handbook of Social Psychology, Vol. 2. Chapter Close relationships. Wiley. Hoboken, NJ. Edition 5. 898–940 Pages. S. T. Fiske, D. T. Gilbert, and G. Lindzey (Eds.).
When we observe people’s behavior, we may attempt to determine if the behavior
really reflects their underlying personality. If Frank hits Joe, we might
wonder if Frank is naturally aggressive or if perhaps Joe had provoked him. If
Leslie leaves a big tip for the waitress, we might wonder if she is a generous
person or if the service was particularly excellent. The
process of trying to determine the causes of people’s behavior, with the
goal of learning about their personalities, is known as causal
attribution. [1]
Making causal attributions is a bit like conducting a research study. We carefully
observe the people we are interested in and note how they behave in different
social situations. After we have made our observations, we draw our
conclusions. Sometimes we may decide that the source or cause of the behavior
was due to characteristics that reside within the individual; this is referred to as a
dispositional attribution. At other times, we may
determine that the behavior was caused primarily by the situation; this is
called making a situational attribution. And at other
times we may decide that the behavior was caused by both the person and the
situation.
It is easier to make personal attributions when behavior is more unusual or
unexpected. Imagine that you go to a party and you are introduced to Tess. Tess
shakes your hand and says “Nice to meet you!” Would you readily conclude, on the
basis of this behavior, that Tess is a friendly person? Probably not. Because
the social situation demands that people act in a friendly way (shaking your
hand and saying “nice to meet you”), it is difficult to know whether Tess was
friendly because of the situation or because she is really friendly. Imagine,
however, that instead of shaking your hand, Tess sticks out her tongue at you
and walks away. I think you would agree that it is easier in this case to infer
that Tess is unfriendly because her behavior is so contrary to what one would
expect. [2]
Although people are reasonably accurate in their attributions (we could say,
perhaps, that they are “good enough”), [3] they are far from
perfect. One error that we frequently make when making judgments about
ourselves is to make self-serving attributions by
judging the causes of our own behaviors in overly positive ways. If you did
well on a test, you will probably attribute that success to dispositional attributions (“I’m
smart,” “I studied really hard”), but if you do poorly on the test you are more
likely to make situational attributions (“The test was hard,” “I had bad luck”).
Although making causal attributions is expected to be logical and scientific,
our emotions are not irrelevant.
Another way that our attributions are often inaccurate is that
we are, by and
large, too quick to attribute the behavior of other people to
something about them rather than to something about their situation. We
are more
likely to say, “Leslie left a big tip, so she must be generous”
than “Leslie
left a big tip, but perhaps that was because the service was
really excellent.”
The common tendency to overestimate the role of
dispositional factors and overlook the impact of situations in judging
others is known as the fundamental attribution error
(or correspondence bias).
The fundamental attribution error occurs in part because other people are so salient in our
social environments. When I look at you, I see you as my focus, and so I am likely to make
personal attributions about you. If the situation is reversed such that people see
situations from the perspectives of others, the fundamental attribution error is
reduced. [4] And when we judge people, we
often see them in only one situation. It’s easy for you to think that your math professor
is “picky and detail-oriented” because that describes her behavior in class, but you don’t
know how she acts with her friends and family, which might be completely different. And we
also tend to make person attributions because they are easy. We are more likely to commit
the fundamental attribution error—quickly jumping to the conclusion that behavior is caused
by underlying personality—when we are tired, distracted, or busy doing other
things. [5]
An important moral about perceiving others applies here: We should not
be too quick to judge other people. It is easy to think that poor people are lazy,
that people who say something harsh are rude or unfriendly, and that all terrorists are
insane madmen. But these attributions may frequently overemphasize the role of the person,
resulting in an inappropriate and inaccurate tendency to blame the
victim. [6] [7] Sometimes people are lazy and rude, and some terrorists
are possibly insane, but these people may also be influenced by the situation in which they
find themselves. Poor people may find it more difficult to get work and education because
of the environment they grow up in, people may say rude things because they are feeling
threatened or are in pain, and terrorists may have learned in their family and school that
committing violence in the service of their beliefs is justified. When you find yourself
making strong person attributions for the behaviors of others, I hope you will stop and
think more carefully. Would you want other people to make person attributions for your
behavior in the same situation, or would you prefer that they more fully consider the
situation surrounding your behavior? Are you perhaps making the fundamental attribution
error?
References
- Jones, E. E., Kanouse, D. E., Kelley, H. H., Nisbett, R. E., Valins, S., and Weiner, B. (Eds.).
(1987).
Attribution: Perceiving the Causes of Behavior. Lawrence Erlbaum Associates. Hillsdale, NJ.
- Jones, E. E., Davis, K. E., and Gergen, K. J.
(1961).
"Role playing variations and their informational value for person
perception." Journal of Abnormal and Social Psychology. Volume 63.
Number 2. 302–310 Pages.
- Fiske, S. T.
(2003).
Social Beings. Wiley. Hoboken, NJ.
- Storms, M. D.
(1973).
"Videotape and the attribution process: Reversing actors’ and
observers’ points of view." Journal of Personality and Social
Psychology. Volume 27. Number 2. 165–175 Pages.
- Trope, Y., and Alfieri, T.
(1997).
"Effortfulness and flexibility of dispositional judgment
processes." Journal of Personality and Social Psychology. Volume 73.
Number 4. 662–674 Pages.
- Lerner, M.
(1980).
The Belief in a Just World: A Fundamental Delusion. Plenum. New York.
- Tennen, H., and Affleck, G.
(1990).
"Blaming others for threatening events." Psychological Bulletin. Volume 108. Number 2. 209–232 Pages.
Attitude refers to our relatively enduring
evaluations of people and
things. [1] We each hold
many thousands of attitudes, including those about family and friends, political parties
and political figures, abortion rights, preferences for music, and much more. Some of
our attitudes, including those about sports, roller coaster rides, and capital
punishment, are at least in part heritable, which explains why we are similar to our parents on
many dimensions. [2] Other
attitudes are learned through direct and indirect experiences with the attitude
objects. [3]
Attitudes are important because they frequently (but not always) predict behavior. If we
know that a person has a more positive attitude toward Frosted Flakes than toward
Cheerios, then we will naturally predict that she will buy more of the former when she
gets to the market. If we know that Charlie is in love with Charlene, then we will
not be surprised when he proposes marriage. Because attitudes often predict behavior,
people who wish to change behavior frequently try to change attitudes through the use of
persuasive communications. The following table presents some
of the many techniques that can be used to change people’s
attitudes. [4]
| Techniques That Can Be Effective in Persuading Others |
|---|
| From Flat World Knowledge, Introduction to Psychology, CC-BY-NC-SA. |
| Technique |
Examples |
| Choose effective communicators. |
Communicators who are attractive, expert, trustworthy, and similar to the
listener are most persuasive. |
| Consider the goals of the listener. |
If the listener wants to be entertained, then it is better to use a humorous ad;
if the listener is processing the ad more carefully, use a more thoughtful
one. |
| Use humor. |
People are more easily persuaded when they are in a good mood. |
| Use classical conditioning. |
Try to associate your product with positive stimuli such as funny jokes or
attractive models. |
| Make use of the listener's emotions. |
Humorous and fear-arousing ads can be effective because they arouse the
listener’s emotions. |
| Use the listener's behavior to modify his or her attitude. |
One approach is the foot-in-the-door technique. First
ask for a minor request, and then ask for a larger request after the smaller
request has been accepted. |
|
Attitudes predict behavior better for some people than for others. People who are high in
self-monitoring—the
tendency to regulate behavior to meet the demands of social situations—tend to
change their behaviors to match the social situation and thus do not always act on their
attitudes. [5] High self-monitors agree with
statements such as, “In different situations and with different people, I often act like
very different persons” and “I guess I put on a show to impress or entertain people.”
Attitudes are more likely to predict behavior for low self-monitors, who are more likely
to act on their own attitudes even when the social situation suggests that they should
behave otherwise. Low self-monitors are more likely to agree with statements such as “At
parties and social gatherings, I do not attempt to do or say things that others will
like” and “I can only argue for ideas that I already believe.”
The match between the social situations in which the attitudes are expressed and the
behaviors are engaged in also matters, such that there is a greater attitude-behavior
correlation when the social situations match. Imagine for a minute the case of Magritte,
a 16-year-old high school student. Magritte tells her parents that she hates the idea of
smoking cigarettes. But how sure are you that Magritte’s attitude will predict her
behavior? Would you be willing to bet that she’d never try smoking when she’s out with
her friends?
The problem here is that Magritte’s attitude is being expressed in one social situation
(when she is with her parents) whereas the behavior (trying a cigarette) is going to
occur in a very different social situation (when she is out with her friends). The
relevant social norms are, of course, much different in the two situations. Magritte’s
friends might be able to convince her to try smoking, despite her initial negative
attitude, by enticing her with peer pressure. Behaviors are more likely to be consistent
with attitudes when the social situation in which the behavior occurs is similar to the
situation in which the attitude is expressed. [6]
Although it might not have surprised you to hear that our attitudes predict our
behaviors, you might be more surprised to learn that our behaviors also have an
influence on our attitudes. It makes sense that if I like Frosted Flakes I’ll buy them,
because my positive attitude toward the product influences my behavior. But my attitudes
toward Frosted Flakes may also become more positive if I decide—for whatever reason—to
buy some. It makes sense that Charlie’s love for Charlene will lead him to propose
marriage, but it is also the case that he will likely love Charlene even more after he
does so.
Behaviors influence attitudes in part through the process of self-perception. Self-perception occurs when we use our own behavior as a guide to help us determine our own thoughts and
feelings. [7] [8] In one demonstration of
the power of self-perception, Wells and Petty [9] assigned their research
participants to shake their heads either up and down or side to side as they read
newspaper editorials. The participants who had shaken their heads up and down later
agreed with the content of the editorials more than the people who had shaken them side
to side. Wells and Petty argued that this occurred because the participants used their
own head-shaking behaviors to determine their attitudes about the editorials.
Persuaders may use the principles of self-perception to change attitudes. The foot-in-the-door technique is a method of persuasion in which
the person is first persuaded to accept a rather minor request and then asked for a
larger one after that. In one demonstration, Guéguen and Jacob [10] found that
students in a computer discussion group were more likely to volunteer to complete a
40-question survey on their food habits (which required 15 to 20 minutes of their time)
if they had already, a few minutes earlier, agreed to help the same requestor with a
simple computer-related question (about how to convert a file type) than if they had not
first been given the smaller opportunity to help. The idea is that when asked the second
time, the people looked at their past behavior (having agreed to the small request) and
inferred that they are helpful people.
Behavior also influences our attitudes through a more emotional process known as cognitive dissonance. Cognitive dissonance refers to the discomfort we experience when we choose to behave in ways that we
see as
inappropriate. [11] [12]
If we feel that we have wasted our time or acted against our own moral principles, we
experience negative emotions (dissonance) and may change our attitudes about the
behavior to reduce the negative feelings.
Elliot Aronson and Judson Mills [13] studied whether the cognitive dissonance
created by an initiation process could explain how much commitment students felt to a
group that they were part of. In their experiment, female college students volunteered
to join a group that would be meeting regularly to discuss various aspects of the
psychology of sex. According to random assignment, some of the women were told that they
would be required to perform an embarrassing procedure (they were asked to read some
obscene words and some sexually oriented passages from a novel in public) before they
could join the group, whereas other women did not have to go through this initiation.
Then all the women got a chance to listen to the group’s conversation, which turned out
to be very boring.
Aronson and Mills found that the women who had gone through the embarrassing experience
subsequently reported more liking for the group than those who had not. They argued that
the more effort an individual expends to become a member of the group (e.g., a severe
initiation), the more they will become committed to the group, to justify the effort
they have put in during the initiation. The idea is that the effort creates dissonant
cognitions (“I did all this work to join the group”), which are then justified by
creating more consonant ones (“OK, this group is really pretty fun”). Thus the women who
spent little effort to get into the group were able to see the group as the dull and
boring conversation that it was. The women who went through the more severe initiation,
however, succeeded in convincing themselves that the same discussion was a worthwhile
experience.
When we put in effort for something—an initiation, a big purchase price, or even some of
our precious time—we will likely end up liking the activity more than we would have if
the effort had been less; not doing so would lead us to experience the unpleasant
feelings of dissonance. After we buy a product, we convince ourselves that we made the
right choice because the product is excellent. If we fail to lose the weight we wanted
to, we decide that we look good anyway. If we hurt someone else’s feelings, we may even
decide that he or she is a bad person who deserves our negative behavior. To escape from
feeling poorly about themselves, people will engage in quite extraordinary
rationalizing. No wonder that most of us believe that “If I had it all to do over again,
I would not change anything important.”
learn by doing
Social psychologists generally define an attitude as an evaluation of a person,
object, or idea. The evaluation can be positive, negative, or even ambivalent.
To elaborate further on the definition of an attitude, consider its three parts:
an affective component, consisting of our emotional reactions toward the
attitude object (e.g., another person or a social issue); a cognitive component,
consisting of our thoughts and beliefs about the attitude object, and a
behavioral component, consisting of our actions or observable behaviors toward
the attitude object.
learn by doing
As we have seen, not only do our attitudes often
predict our behaviors, but our behaviors
often have a substantial effect on our attitudes.
Self-perception theory and
cognitive dissonance theory provide different
explanations of how our behavior
can influence our attitudes. In this activity, you
will see ten scenarios. Each is an example of self-perception, cognitive
dissonance or some other concept. For each of the following scenarios,
indicate which
theory best applies.
References
- Albarracín, D., Johnson, B. T., and Zanna, M. P. (Eds.).
(2005).
The Handbook of Attitudes. Lawrence Erlbaum Associates. Mahwah, NJ.
- Olson, J. M., Vernon, P. A., Harris, J. A.,
and Jang, K. L.
(2001).
"The heritability of attitudes: A study of twins." Journal of
Personality and Social Psychology. Volume 80. Number 6. 845–860 Pages.
- De Houwer, J., Thomas, S., and Baeyens,
F.
(2001).
"Association learning of likes and dislikes: A review of 25 years
of research on human evaluative conditioning." Psychological Bulletin.
Volume 127. Number 6. 853–869 Pages.
- Cialdini, R. B.
(2001).
Influence: Science and Practice. Allyn and Bacon. Boston.
- Gangestad, S. W., and Snyder, M.
(2000).
"Self-monitoring: Appraisal and reappraisal." Psychological Bulletin. Volume 126. Number 4. 530–555 Pages.
- Ajzen, I.
(1991).
"The theory of planned behavior." Organizational Behavior and Human
Decision Processes. Volume 50. Number 2. 179–211 Pages.
- Bem, D. J.
(1972).
Advances in Experimental Social Psychology, Vol. 6. Chapter Self-perception theory. Academic Press. New York. 1–62 Pages. L. Berkowitz (Ed.).
- Olson, J. M., and Stone, J.
(2005).
The Handbook of Attitudes. Chapter The
influence of behavior on attitudes. Lawrence Erlbaum Associates. Mahwah,
NJ. 223–271 Pages. D. Albarracín, B. T. Johnson, and M. P. Zanna
(Eds.).
- Wells, G. L., and Petty, R. E.
(1980).
"The effects of overt head movements on persuasion: Compatibility
and incompatibility of responses." Basic and Applied Social Psychology.
Volume 1. Number 3. 219–230 Pages.
- Guéguen, N., and Jacob, C.
(2002).
"Solicitation by e-mail and solicitor’s status: A field study of
social influence on the web." CyberPsychology and Behavior. Volume 5.
Number 4. 377–383 Pages.
- Festinger, L.
(1957).
A Theory of Cognitive Dissonance. Row, Peterson. Evanston, IL.
- Harmon-Jones, E., and Mills, J.
(1999).
Cognitive Dissonance: Progress on a Pivotal Theory in Social Psychology. American Psychological Association. Washington, DC.
- Aronson, E., and Mills, J.
(1959).
"The effect of severity of initiation on liking for a group."
Journal of Abnormal and Social Psychology. Volume 59. Number 2. 171–181
Pages.
Humans have developed a variety of social skills that enhance our ability to successfully
interact with others. We are often helpful, even when that helping comes at some cost to
ourselves, and we often change our opinions and beliefs to fit in with the opinions of
those whom we care about. Yet we also are able to be aggressive if we feel the situation
warrants it.
Helping Others: Altruism Helps Create Harmonious Relationships
Altruism refers to any behavior that is designed to
increase another person’s welfare, and particularly those actions that do
not seem to provide a direct reward to the person who performs
them. [1] Altruism occurs when we stop to help a stranger who
has been stranded on the highway, when we volunteer at a homeless shelter, or
when we donate to a charity. According to a survey conducted by Independent Sector, a coalition that studies and encourages
volunteering, in 2001 over 83 million
American adults reported that they helped others by volunteering, on
average of 3.6 hours per week.
Why Do We Help?
Because altruism is costly, you might wonder why we engage in it at all. There
are a variety of explanations for the occurrence of altruism, and the following
table summarizes some of the variables that are known to increase helping.
| Some of the Variables Known to Increase Helping |
|---|
| From Flat World Knowledge, Introduction to Psychology, CC-BY-NC-SA. |
| Variable |
Explanation |
| Positive moods |
We help more when we are in a good mood. [2]
|
| Similarity |
We help people who we see as similar to us, for instance, those who
mimic our behaviors. [3]
|
| Guilt |
If we are experiencing guilt, we may help relieve those negative
feelings. |
| Empathy |
We help more when we feel empathy for the other person. [4]
|
| Benefits |
We are more likely to help if we can feel good about ourselves by doing
so. [5]
|
| Personal responsibility |
We are more likely to help if it is clear that others are not
helping. |
| Self-presentation |
We may help in order to show others that we are good people. [6]
|
|
The tendency to help others in need may be a functional evolutionary
adaptation. Although helping others can be costly to us as individuals, helping
people who are related to us can perpetuate our own
genes. [7] [8] [9]
Burnstein, Crandall, and Kitayama [10] found that students indicated
they would be more likely to help a person who was closely related to them
(e.g., a sibling, parent, or child) than they would be to help a person who was
more distantly related (e.g., a niece, nephew, uncle, or grandmother). People
are more likely to donate kidneys to relatives than to
strangers, [11] and even children
indicate that they are more likely to help their siblings than they are to help
a friend. [12]
Although it makes evolutionary sense that we would help people who we are related
to, why would we help people to whom we not related? One explanation for such
behavior is based on the principle of reciprocal
altruism. [13] [14] Reciprocal altruism is the principle
that, if we help other people now, those others will return the favor should
we need their help in the future. By helping others, we
increase
the chances of survival and reproductive success for ourselves and
for those we help. Over the course of evolution, those who engage in
reciprocal
altruism should be able to reproduce more often than those who do
not, thus
enabling this kind of altruism to continue.
We also learn to help by imitating the helpful behavior of others. Although people frequently
worry about the negative impact of the violence in mass media, there is
also a great deal of helping behavior shown on television. Smith and
colleagues [15]
found that 73% of TV shows
had some altruism, and that about three altruistic behaviors were
shown every
hour. Furthermore, the prevalence of altruism was particularly high
in
children’s shows. But just as viewing altruism can increase
helping, imitating behavior that is not altruistic can decrease
altruism. For instance, Anderson
and Bushman [16] found that playing
violent video games led to a decrease in helping.
We are more likely to help when we receive rewards for doing so and less likely
to help when helping is costly. Parents praise their children who share their
toys with others, and may reprimand children who are selfish. In addition, we are more likely
to help when we have plenty of time than when we are in a
hurry. [17] Another potential reward is the status we
gain as a result of helping. When we act altruistically, we gain a reputation as
a person with high status who is able and willing to help others, and this
status makes us more desirable in the eyes of
others. [6]
One outcome of the reinforcement of altruism is the development of
social norms about helping—standards of behavior that we see as appropriate and
desirable . The reciprocity norm
reminds us that we should follow the principles of reciprocal altruism. If
someone helps us, then we should help them in the future, and we should help
people now with the expectation that they will help us later if we need it. The
reciprocity norm is expressed in everyday adages such as “Scratch my back and I’ll
scratch yours” and in religious and philosophical teachings such as the “Golden
Rule”: “Do unto other as you would have them do unto you.”
Because this kind of helping is based on the return of earlier
help and the expectation of a future return from others, it might not seem like
true altruism. We might hope that our children internalize another relevant
social norm that seems more altruistic: the social
responsibility norm, which tells us that we
should try to help others who need assistance, even without any expectation of
future paybacks. This is the basis of many religious and ethical principles: as good human beings, we shoud reach out and help
other people whenever we can.
How the Presence of Others Can Reduce Helping
Late at night on March 13, 1964, 28-year-old Kitty Genovese was murdered within a
few yards of her apartment building in New York City after a violent fight with
her killer in which she struggled and screamed. When the police interviewed
Kitty’s neighbors about the crime, they discovered that 38 people
indicated that they had seen or heard the fight but none of them
intervened, and only one person called the police.
Was Kitty Genovese murdered because there were too many people who
heard her cries? Watch this video for an analysis.
Two social psychologists, Bibb Latané and John Darley, were interested in the
factors that influenced people to help (or to not help) in such
situations. [18]
They developed a model (see
the figure below) that took into consideration the important role
of the social
situation in determining helping. The model has been extensively
tested in many
studies. Social psychologists have
discovered that it was the 38 people themselves that contributed to
the tragedy,
because people are less likely to notice, interpret, and respond to
the emergencies when they are with others than they are when they are
alone.
The first step in the model is noticing the event. Latané and Darley [18] asked research participants to complete a questionnaire in a small
room. Some of the participants completed the questionnaire alone, whereas others
completed it in small groups. A few minutes after the participants had begun
the questionnaires, some white smoke came into
the room through a vent in the wall. The experimenters timed how long it took
before the first person in the room looked up and noticed the smoke.
The people who were working alone noticed the smoke in about 5 seconds, and
within 4 minutes most of the participants who were working alone had taken some
action. On the other hand, on average, the first person in the group conditions
did not notice the smoke until over 20 seconds had elapsed. And, although 75% of
the participants who were working alone reported the smoke within 4 minutes, the
smoke was reported in only 12% of the groups by that time. In fact, in only 3 of
the 8 groups did anyone report the smoke, even after it had filled the room. You
can see that the social situation has a powerful influence on noticing; we
simply don’t see emergencies when other people are with us.
Even if we notice an emergency, we might not interpret it as one. Were the cries
of Kitty Genovese really calls for help, or were they simply an argument with a
boyfriend? The problem is compounded when others are present. When we
are unsure how to interpret events we normally look to others to help us
understand them, and at the same time they also are looking to us for information.
The problem is that each bystander thinks that other people aren’t acting
because they don’t see an emergency. Believing that the others know something
that they don’t, each observer concludes that help is not required.
Even if we have noticed the emergency and interpret it as being one, this does
not necessarily mean that we will come to the rescue of the other person. We
still need to decide that it is our responsibility to do something. The problem
is that when we see others around, it is easy to assume that they are going to
do something, and that we don’t need to do anything ourselves. Diffusion of responsibility occurs when we assume
that others will take action and therefore we do not take action
ourselves. The irony again, of course, is that people are more likely
to help when they are the only ones in the situation than when there are others
around.
Perhaps you have noticed diffusion of responsibility in social media like Facebook. Did you
find that it was easier to get help if you directed your request to a smaller
set of users than when you directed it to a larger number of people?
Markey [19] found that people received help more quickly (in about 37
seconds) when they asked for help by specifying a participant’s name than when
no name was specified (51 seconds).
The final step in the helping model is knowing how to help. Most
of us are not professionals and we have little training in how to help
in
emergencies. People with emergency-response training are more
likely to help. The rest of us just don’t know what to do, and
therefore
we may simply walk by. On the other hand, today many people have
cell phones,
and we can do a lot with a quick call; in fact, a phone call made
in time might
have saved Kitty Genovese’s life.
References
- Dovidio, J. F., Piliavin, J. A., Schroeder, D. A., and Penner, L.
(2006).
The Social Psychology of Prosocial Behavior. Lawrence Erlbaum Associates. Mahwah, NJ.
- Guéguen, N., and De Gail, M.-A.
(2003).
"The effect of smiling on helping behavior: Smiling and Good
Samaritan behavior." Communication Reports. Volume 16. Number 2. 133–140
Pages.
- van Baaren, R. B., Holland, R. W., Kawakami, K., and van Knippenberg, A.
(2004).
"Mimicry and prosocial behavior." Psychological Science. Volume 15. Number 1. 71–74 Pages.
- Batson, C. D., O’Quin, K., Fultz, J.,
Varnderplas, M., and Isen, A.
(1983).
"Influence of self-reported distress and empathy on egoistic versus
altruistic motivation to help." Journal of Personality and Social
Psychology. Volume 45. Number 3. 706–718 Pages.
- Snyder, M., Omoto, A. M., and Lindsay, J. J. (Eds.).
(2004).
Sacrificing Time and Effort for the Good of Others: The Benefits and Costs of Volunteerism. Guilford Press. New York.
- Hardy, C. L., and Van Vugt, M.
(2006).
"Nice guys finish first: The competitive altruism hypothesis."
Personality and Social Psychology Bulletin. Volume 32. Number 10.
1402–1413 Pages.
- Madsen, E. A., Tunney, R. J., Fieldman, G.,
Plotkin, H. C., Dunbar, R. I. M., Richardson, J.-M., et al.
(2007).
"Kinship and altruism: A cross-cultural experimental study."
British Journal of Psychology. Volume 98. Number 2. 339–359 Pages.
- McAndrew, F. T.
(2002).
"New evolutionary perspectives on altruism: Multilevel-selection
and costly-signaling theories." Current Directions in Psychological
Science. Volume 11. Number 2. 79–82 Pages.
- Stewart-Williams, S.
(2007).
"Altruism among kin vs. nonkin: Effects of cost of help and
reciprocal exchange." Evolution and Human Behavior. Volume 28. Number 3.
193–198 Pages.
- Burnstein, E., Crandall, C., and Kitayama, S.
(1994).
"Some neo-Darwinian decision rules for altruism: Weighing cues for
inclusive fitness as a function of the biological importance of the
decision." Journal of Personality and Social Psychology. Volume 67.
Number 5. 773–789 Pages.
- Borgida, E., Conner, C., and Manteufel, L.
(1992).
Understanding Living Kidney Donation: A Behavioral Decision-Making Perspective. Sage. Thousand Oaks, CA.
- Tisak, M. S., and Tisak, J.
(1996).
"My sibling’s but not my friend’s keeper: Reasoning about responses
to aggressive acts." Journal of Early Adolescence. Volume 16. Number 3.
324–339 Pages.
- Krebs, J. R., and Davies, N. B.
(1987).
An Introduction to Behavioural Ecology. Sinauer Associates. Sunderland, MA. Edition 2.
- Trivers, R. L.
(1971).
"The evolution of reciprocal altruism." Quarterly Review of Biology. Volume 46. Number 1. 35–57 Pages.
- Smith, S. W., Smith, S. L., Pieper, K. M., Yoo, J.
H., Ferris, A. L., Downs, E., et al.
(2006).
"Altruism on American television: Examining the amount of, and
context surrounding, acts of helping and sharing." Journal of
Communication. Volume 56. Number 4. 707–727 Pages.
- Anderson, C. A., and Bushman, B. J.
(2001).
"Effects of violent video games on aggressive behavior, aggressive
cognition, aggressive affect, physiological arousal, and prosocial
behavior: A meta-analytic review of the scientific literature."
Psychological Science. Volume 12. Number 5. 353–359 Pages.
- Darley, J. M., and Batson, C. D.
(1973).
"“From Jerusalem to Jericho”: A study of situational and
dispositional variables in helping behavior." Journal of Personality and
Social Psychology. Volume 27. Number 1. 100–108 Pages.
- Latané, B., and Darley, J. M.
(1968).
"Group inhibition of bystander intervention in emergencies."
Journal of Personality and Social Psychology. Volume 10. Number 3.
215–221 Pages.
- Markey, P. M.
(2000).
"Bystander intervention in computer-mediated communication."
Computers in Human Behavior. Volume 16. Number 2. 183–188 Pages.
Aggression is behavior that is intended to harm
another individual. Aggression may occur in the heat of the
moment, for
instance, when a jealous lover strikes out in rage or fans light
fires and destroy cars after an important basketball game. Or it may
occur in a
more cognitive, deliberate, and planned way, such as the aggression
of a bully who
steals another child’s toys, a terrorist who kills civilians to gain
political exposure,
or a hired assassin who kills for money.
Not all aggression is physical. Aggression also occurs in nonphysical ways, as when
children exclude others from activities, call them names, or spread rumors about them.
Paquette and Underwood [1] found that both boys and girls said that nonphysical
aggression such as name-calling made them feel more “sad and bad” than did physical
aggression.
The Ability to Aggress Is Part of Human Nature
We may aggress against others in part because it allows us to gain access to
valuable resources such as food, territory, and desirable mates, or to protect
ourselves from direct attack by others. If aggression helps in the survival of
our genes, then the process of natural selection may well have caused humans, as
it would any other animal, to be
aggressive. [2]
There is evidence for the genetics of aggression. Aggression is
strongly influenced by the amygdala. One of the primary functions of the
amygdala is to
help us learn to associate stimuli with the rewards and the
punishment that they
may provide. The amygdala is particularly activated in our
responses to threatening or fear-arousing stimuli.
But just because we can aggress does not mean that we will aggress. It is not necessarily evolutionarily
adaptive to aggress in all situations. Neither people nor animals are always
aggressive; they rely on aggression only when they feel that they absolutely
need to. [3] The
prefrontal cortex serves as a control center on aggression; when it is more
highly activated, we are more able to control our aggressive impulses. Research
has found that the cerebral cortex is less active in murderers and death row
inmates, suggesting that violent crime may be caused at least in part by a
failure or reduced ability to regulate
aggression. [4]
Hormones are also important in regulating aggression. In particular, testosterone, is
associated with increased aggression in both males and females. Research
conducted on a variety of animals has found a positive correlation between
levels of testosterone and aggression. This relationship seems to be weaker
among humans than among animals, yet it is still
significant. [5]
Consuming alcohol increases the likelihood that people will respond aggressively to
provocations, even for people who are not normally aggressive. [6] Alcohol lowers inhibitions and makes people more self-focused and less aware of the social constraints that
normally prevent them from engaging
aggressively. [7] [8]
Negative Experiences Increase Aggression
If I were to ask you about the times that you have been aggressive, I bet that
you would say it was more likely when you were angry, in a bad mood,
tired, in pain, sick, or frustrated and you would be right: We are much more
likely to aggress when we are experiencing negative emotions especially frustration. When we are frustrated we may lash out
at others, even at people who did not cause it. In some cases the
aggression is displaced aggression, which is aggression that is directed at an object or person other than
the person who caused the frustration.
Other negative emotions also increase aggression. Griffit and Veitch [9]
had students complete questionnaires either in rooms at a normal temperature or where the temperature was over 90 degrees
Fahrenheit. The students in the hot rooms expressed significantly more
hostility. Aggression is greater during heat waves, and most violent riots occur during
the hottest days of the year. [10] Pain
also increases aggression. [11]
If we are aware that we are feeling negative emotions, we might think that we
could release them in a relatively harmless way, such as by punching a
pillow or kicking something, with the hopes that doing so will release our
aggressive tendencies. Catharsis—the
idea that observing or engaging in less harmful aggressive actions will
reduce the tendency to aggress later in a more harmful way—has been
considered by many as a way of decreasing violence, and it was an important part
of the theories of Sigmund Freud.
As far as social psychologists have been able to determine, however, catharsis
simply does not work. Rather than decreasing aggression, engaging in aggressive
behaviors of any type increases the likelihood of later aggression. Bushman,
Baumeister, and Stack [12] first angered their research participants by
having another student insult them. Then half of the participants were allowed
to engage in a cathartic behavior: They were given boxing gloves and then got a
chance to hit a punching bag for 2 minutes. Then all the participants played a
game in which they had a chance to
blast their opponent with a painful blast of white noise. Contrary to the
catharsis hypothesis, the students who hit the punching bag set a higher
noise level and delivered longer bursts of noise than the participants who did
not. It seems that if we hit a punching
bag, punch a pillow, or scream as loud as we can to release our frustration, the
opposite may occur—rather than decreasing aggression, these behaviors in fact
increase it.
Viewing Violent Media Increases Aggression
The average American watches over 4 hours of television every
day, and these programs contain
a substantial amount of aggression. At the same time, children are
also exposed
to violence in movies and video games, as well as in popular music
and music
videos that include violent lyrics and imagery. Research evidence
suggests that, on average, people who watch violent behavior become more
aggressive. The evidence supporting this relationship comes from
many studies
conducted over many years using both correlational designs as well
as experiments in which people have been randomly assigned to view
either violent or
nonviolent material. [13]
Viewing violent behavior also increases aggression in part through observational
learning. Children who witness violence are more likely to be aggressive. One
example is in the studies of Albert Bandura, as shown below.
This video shows Professor Albert Bandura describing his studies on the
observational learning of aggression in children.
Another outcome of viewing large amounts of violent material is desensitization, which is the tendency over time to
show weaker emotional responses to emotional stimuli. When we first see
violence, we are likely to be shocked, aroused, and even repulsed by it.
However, over time, as we see more and more violence, we become habituated to
it, such that the subsequent exposures produce fewer and fewer negative
emotional responses. Continually viewing violence also makes us more distrustful
and more likely to behave
aggressively. [14] [15]
Of course, not everyone who views violent material becomes aggressive; individual
differences also matter. People who experience a lot of negative affect and who
feel that they are frequently rejected by others are more
aggressive . [16] People with
inflated or unstable self-esteem are more prone to anger and are highly
aggressive when their high self-image is
threatened. [17] For instance,
classroom bullies are those children who always want to be the center of
attention, who think a lot of themselves, and who cannot take
criticism. [18] Bullies are highly motivated
to protect their inflated self-concept, and they react with anger and
aggression when it is threatened.
Across cultures, men tend to be more physically violent
than women . [19] [20]
About 99% of rapes and about 90% of robberies, assaults, and murders
are committed by men. [21] These gender differences do not imply that women are never aggressive. Both men and women
respond to insults and provocation with aggression; the differences between men
and women are smaller after they have been frustrated, insulted, or
threatened. [22]
Research Focus: The Culture of Honor
In addition to differences across cultures, there are also regional differences
in the incidence of violence. As one
example, the homicide rate is significantly higher in the southern and the
western states but lower in the eastern and northern states. One explanation for
these differences is variation in cultural norms about the appropriate reactions
to threats against one’s social status. These cultural differences apply
primarily to men. In short, some men react more violently than others when they
believe that others are threatening or insulting them.
The social norm that condones and even encourages responding
to insults with aggression is known as the culture of
honor. The culture of honor leads people to view even relatively minor
conflicts or disputes as challenges to one’s social status and reputation and
can therefore trigger aggressive responses. Beliefs in culture of honor norms
are stronger among men who live or who were raised in the South and West than
among men who are from or living in the North and East.
In one series of experiments, Cohen, Nisbett, Bosdle, and Schwarz [23]
investigated how white male students who had grown up either in the northern or
in the southern regions of the United States responded to insults. The
experiments, involved an
encounter in which the research participant was walking down a narrow hallway.
The experimenters enlisted the help of a confederate who did not give way to the
participant but rather bumped into him and insulted him. Compared with
Northerners, students from the South who had been bumped were more likely to
think that their masculine reputations had been threatened, exhibited greater
physiological signs of being upset, had higher testosterone levels, engaged in
more aggressive and dominant behavior (gave firmer handshakes), and were less
willing to yield to a subsequent confederate.
In another test of the impact of culture of honor, Cohen and Nisbett [24] sent letters to employers across the United States from a
fictitious job applicant who admitted having been convicted of a felony. To half
the employers, the applicant reported that he had impulsively killed a man who
had been having an affair with his fiancée and then taunted him about it in a
crowded bar. To the other half, the applicant reported that he had stolen a car
because he needed the money to pay off debts. Employers from the South and the
West, places in which the culture of honor is strong, were more likely than
employers in the North and East to respond in an understanding and cooperative
way to the letter from the convicted killer, but there were no cultural
differences for the letter from the auto thief.
One possible explanation for regional differences in the culture of honor
involves their history. While people in the northern parts of the United States were usually
farmers who grew crops, people from southern climates were more likely to raise
livestock. Unlike the crops grown by the northerners, the herds were mobile and
vulnerable to theft, and it was difficult for law enforcement officials to
protect them. To be successful in an environment where theft was common, a man
had to build a reputation for strength and toughness, and this was accomplished
by a willingness to use swift, and sometimes violent, punishment against
thieves.
References
- Paquette, J. A., and Underwood, M. K.
(1999).
"Gender differences in young adolescents’ experiences of peer
victimization: Social and physical aggression." Merrill-Palmer
Quarterly. Volume 45. Number 2. 242–266 Pages.
- Buss, D. M., and Duntley, J. D. (Eds.).
(2006).
The Evolution of Aggression. Psychosocial Press. Madison, CT.
- Berkowitz, L.
(1993).
Aggression: Its Causes, Consequences and Control. McGraw-Hill. New York.
- Davidson, R. J., Putnam, K. M., and Larson, C.
L.
(2000).
"Dysfunction in the neural circuitry of emotion regulation—A
possible prelude to violence." Science. Volume 289. Number 5479. 591–594
Pages.
- Dabbs, J. M. Jr., Hargrove, M. F., and Heusel, C.
(1996).
"Testosterone differences among college fraternities: Well-behaved
vs. rambunctious." Personality and Individual Differences. Volume 20.
Number 2. 157–161 Pages.
- Graham, K., Osgood, D. W., Wells, S., and
Stockwell, T.
(2006).
"To what extent is intoxication associated with aggression in bars?
A multilevel analysis." Journal of Studies on Alcohol. Volume 67.
Number 3. 382–390 Pages.
- Bushman, B. J., and Cooper, H. M.
(1990).
"Effects of alcohol on human aggression: An integrative research
review." Psychological Bulletin. Volume 107. Number 3. 341–354 Pages.
- Steele, C. M., and Southwick, L.
(1985).
"Alcohol and social behavior: I. The psychology of drunken excess."
Journal of Personality and Social Psychology. Volume 48. Number 1.
18–34 Pages.
- Griffit, W., and Veitch, R.
(1971).
"Hot and crowded: Influence of population density and temperature
on interpersonal affective behavior." Journal of Personality and Social
Psychology. Volume 17. Number 1. 92–98 Pages.
- Bushman, B. J., Wang, M. C., and Anderson, C. A.
(2005).
"Is the curve relating temperature to aggression linear or
curvilinear? Assaults and temperature in Minneapolis reexamined."
Journal of Personality and Social Psychology. Volume 89. Number 1. 62–66
Pages.
- Berkowitz, L.
(1993).
"Pain and aggression: Some findings and implications." Motivation and Emotion. Volume 17. Number 3. 277–293 Pages.
- Bushman, B. J., Baumeister, R. F., and Stack, A.
D.
(1999).
"Catharsis, aggression, and persuasive influence: Self-fulfilling
or self-defeating prophecies?." Journal of Personality and Social
Psychology. Volume 76. Number 3. 367–376 Pages.
- Anderson, C. A., Berkowitz, L., Donnerstein,
E., Huesmann, L. R., Johnson, J. D., Linz, D., et al.
(2003).
"The influence of media violence on youth." Psychological Science
in the Public Interest. Volume 4. Number 3. 81–110 Pages.
- Bartholow, B. D., Bushman, B. J., and Sestir,
M. A.
(2006).
"Chronic violent video game exposure and desensitization to
violence: Behavioral and event-related brain potential data." Journal of
Experimental Social Psychology. Volume 42. Number 4. 532–539 Pages.
- Nabi, R. L., and Sullivan, J. L.
(2001).
"Does television viewing relate to engagement in protective action
against crime? A cultivation analysis from a theory of reasoned action
perspective." Communication Research. Volume 28. Number 6. 802–825
Pages.
- Downey, G., Irwin, L., Ramsay, M., and Ayduk, O. (Eds.).
(2004).
Rejection Sensitivity and Girls’ Aggression. Kluwer Academic/Plenum. New York.
- Baumeister, R. F., Smart, L., and Boden, J.
M.
(1996).
"Relation of threatened egotism to violence and aggression: The
dark side of high self-esteem." Psychological Review. Volume 103. Number
1. 5–33 Pages.
- Salmivalli, C., and Nieminen, E.
(2002).
"Proactive and reactive aggression among school bullies, victims,
and bully-victims." Aggressive Behavior. Volume 28. Number 1. 30–44
Pages.
- Archer, J., and Coyne, S. M.
(2005).
"An integrated review of indirect, relational, and social
aggression." Personality and Social Psychology Review. Volume 9. Number
3. 212–230 Pages.
- Crick, N. R., and Nelson, D. A.
(2002).
"Relational and physical victimization within friendships: Nobody
told me there’d be friends like these." Journal of Abnormal Child
Psychology. Volume 30. Number 6. 599–607 Pages.
- Graham, K., and Wells, S.
(2001).
"The two worlds of aggression for men and women." Sex Roles. Volume 45. Number 9–10. 595–622 Pages.
- Bettencourt, B., and Miller, N.
(1996).
"Gender differences in aggression as a function of provocation: A
meta-analysis." Psychological Bulletin. Volume 119. Number 3. 422–447
Pages.
- Cohen, D., Nisbett, R. E., Bosdle, B., and
Schwarz, N.
(1996).
"Insult, aggression, and the southern culture of honor: An
experimental ethnography." Journal of Personality and Social Psychology.
Volume 70. Number 5. 945–960 Pages.
- Cohen, D., and Nisbett, R. E.
(1997).
"Field experiments examining the culture of honor: The role of
institutions in perpetuating norms about violence." Personality and
Social Psychology Bulletin. Volume 23. Number 11. 1188–1199 Pages.
When we decide on what courses to enroll in by asking for advice from our friends, change
our beliefs or behaviors as a result of the ideas that we hear from others, or binge
drink because our friends are doing it, we are engaging in conformity, a change in beliefs or behavior that occurs as
the result of the presence of the other people around us. We conform not only
because we believe that other people have accurate information and we want to have
knowledge (informational conformity) but also because we want to
be liked by others (normative conformity).
The typical outcome of conformity is that our beliefs and behaviors become more similar
to those of others around us. But some situations create more conformity than others,
and some of the factors that contribute to conformity are shown in the table below.
| Variables That Increase Conformity |
|---|
| From Flat World Knowledge, Introduction to Psychology.
Sources: Milgram, S., Bickman, L., and Berkowitz, L. (1969). Note on the drawing
power of crowds of different size. Journal of Personality and
Social Psychology 13(2):79–82; and Milgram, S. (1974). Obedience to Authority: An Experimental View. New York: Harper and
Row. |
| Variable |
Description |
Example |
| Number in majority |
As the number of people who are engaging in a behavior increases, the tendency
to conform to those people also increases. |
People are more likely to stop and look up in the air when many, rather than
few, people are also looking
up. [1]
|
| Unanimity |
Conformity reduces sharply when any one person deviates from the norm. |
In Solomon Asch’s line-matching research, when any one person gave a different
answer, conformity was eliminated. |
| Status and authority |
People who have higher status, such as those in authority, create more
conformity. |
Milgram [6]
found that conformity in his obedience studies was greatly reduced
when the person giving the command to shock was described as an “ordinary man”
rather than a scientist at Yale University. |
|
At times conformity occurs in a relatively spontaneous and unconscious way, without any
obvious intent of one person to change the other, or an awareness that the conformity is
occurring. Robert Cialdini and his colleagues [2] found that college students were more
likely to throw litter on the ground themselves when they had just seen another person
throw some paper on the ground, and Cheng and Chartrand [3] found that people unconsciously mimicked the behaviors of others, such
as by rubbing their face or shaking their foot, and that that mimicry was greater when
the other person was of high versus low social status.
Muzafer Sherif [4] studied how norms develop in
ambiguous situations. In his studies, groups of college students were placed in a dark
room with a single point of light and were asked to indicate, each time the light was
turned on and how much it appeared to move. (The movement, which is not actually real,
occurs because of the saccadic movement of the eyes.) Each group member gave his or her
response on each trial aloud and each time in a different random order. As you can see
in figure below, Sherif found a conformity effect: Over time, the responses of the group
members became more and more similar to each other such that after four days they
converged on a common norm. When the participants were interviewed after the study, they
indicated that they had not realized that they were conforming.
Not all conformity is passive. In the research of Solomon Asch [5]
male college students were told that they were to be participating in a test
of visual abilities. The men were seated in front of a board that displayed the visual
stimuli that they were going to judge. The men were told that there would be 18 trials
during the experiment, and on each trial they would see two cards. The standard card had
a single line that was to be judged, and the test card had three lines that varied in
length between about 2 and 10 inches.
On each trial, each person in the group answered out loud, beginning with one end of the
group and moving toward the other end. Although the real research participant did not
know it, the other group members were experimental
confederates who gave predetermined answers on each trial. Because the real participant
was seated next to last in the row, he always made his judgment following most of the
other group members. Although on the first two trials the confederates each gave the
correct answer, on the third trial, and on 11 of the subsequent trials, they all had
been instructed to give the same wrong choice. For instance, even though the correct
answer was Line 1, they would all say it was Line 2. Thus when it became the
participant’s turn to answer, he could either give the clearly correct answer or conform
to the incorrect responses of the confederates.
Remarkably, in this study about 76% of the 123 men who were tested gave at least one
incorrect response when it was their turn, and 37% of the responses, overall, were
conforming. This is indeed evidence for the power of conformity because the participants
were making clearly incorrect responses in public. However, conformity was not absolute;
in addition to the 24% of the men who never conformed, only 5% of the men conformed on
all 12 of the critical trials.
Watch this video to see a demonstration of Asch’s line studies.
The tendency to conform to those in authority, known as obedience, was demonstrated in a remarkable set of studies
performed by Stanley Milgram. [6] Milgram designed
a study in which he could observe the extent to which a person who presented himself as
an authority would be able to produce obedience, even to the extent of leading people to
cause harm to others. Like many other researchers who were interested in conformity,
Milgram’s interest stemmed in part from his desire to understand how the presence of a
powerful social situation—in this case the directives of Adolph Hitler, the German
dictator who ordered the killing of millions of Jews and other “undesirable” people
during World War II—could produce obedience.
Milgram used newspaper ads to recruit men (and in one study, women) from a wide variety
of backgrounds to participate in his research. When the research participant arrived at
the lab, he or she was introduced to a man who was ostensibly another volunteer but who
actually was a confederate working with the
research team. The experimenter
explained that the goal of the research was to study the effects of punishment on
learning. After the participant and the confederate both consented to be in the study,
the researcher explained that one of them would be the teacher, and the other the
learner. They were each given a slip of paper and asked to open it and indicate what it
said. In fact both papers read “teacher,” which allowed the confederate to pretend that
he had been assigned to be the learner and thus to assure that the actual participant
was always the teacher.
While the research participant (now the teacher) looked on, the learner was taken into
the adjoining room and strapped to an electrode that was to deliver the
punishment. The experimenter explained that the teacher’s job would be to sit in the
control room and read a list of word pairs to the learner. After the teacher read the
list once, it would be the learner’s job to remember which words went together. For
instance, if the word pair was “blue sofa,” the teacher would say the word “blue” on the
testing trials, and the learner would have to indicate which of four possible words
(“house,” “sofa,” “cat,” or “carpet”) was the correct answer by pressing one of four
buttons in front of him.
After the experimenter gave the “teacher” a mild shock to demonstrate that the shocks
really were painful, the experiment began. The research participant first read the list
of words to the learner and then began testing him on his learning. The shock apparatus,
shown below, was in front of the teacher, and the learner was not visible in the shock
room. The experimenter sat behind the teacher and explained to him that each time the
learner made a mistake he was to press one of the shock switches to administer the
shock. Moreover, the switch that was to be pressed increased by one level with each
mistake, so that each mistake required a stronger shock.
Once the learner (who was, of course, actually the research confederate) was
alone, he unstrapped himself from the shock machine and
brought out a tape recorder that he used to play a prerecorded series of responses that
the teacher could hear through the wall.
The teacher heard the learner say “ugh!” after the first few shocks. After the next few
mistakes, when the shock level reached 150 Volts, the learner was heard to exclaim, “Let
me out of here. I have heart trouble!” As the shock reached about 270 Volts, the
protests of the learner became more vehement, and after 300 Volts the learner proclaimed
that he was not going to answer any more questions. From 330 Volts and up, the learner
was silent. At this point the experimenter responded to participants’ questions, if any,
with a scripted response indicating that they should continue reading the questions and
applying increasing shock when the learner did not respond.
The results of Milgram’s research were themselves quite shocking. Although all the
participants gave the initial mild levels of shock, responses varied after that. Some
refused to continue after about 150 Volts, despite the insistence of the experimenter to
continue to increase the shock level. Still others, however, continued to present the
questions and to administer the shocks, under the pressure of the experimenter, who
demanded that they continue. In the end, 65% of the participants continued giving the
shock to the learner all the way up to the 450 Volts maximum, even though that shock was
marked as "XXX" and no response had been heard from the
participant for several trials. In other words, well over half of the men who
participated had, as far as they knew, shocked another person to death, all as part of a
supposed experiment on learning.
In case you are thinking that such high levels of obedience would not be observed in
today’s modern culture, there is fact evidence that they would. In a more recent study,
Milgram’s findings were almost exactly replicated, using men and women from a wide
variety of ethnic
groups. [7] In this replication , 67% of
the men and 73% of the women agreed to administer increasingly painful electric shocks
when an authority figure ordered them to. The participants in this study were not,
however, allowed to go beyond the 150-Volt shock switch.
Although it might be tempting to conclude that Burger’s and Milgram’s research
demonstrate that people are innately bad creatures who are ready to shock others to
death, this is not in fact the case. Rather it is the social situation, and not the
people themselves, that is responsible for the behavior. When Milgram created variations
on his original procedure, he found that changes in the situation dramatically
influenced the level of conformity. It was significantly reduced when
people were allowed to choose their own shock level rather than being ordered to use the
level required by the experimenter, when the experimenter communicated by phone rather
than from within the experimental room, or when other research participants refused to
give the shock. These findings are consistent with a basic principle of social
psychology: The situation in which people find themselves has a major influence on their
behavior.
Do We Always Conform?
The research that we have discussed to this point suggests that most people
conform to the opinions and desires of others, but this is not always the
case. For
one, there are individual differences in conformity. People with lower
self-esteem are more likely to conform than are those with higher self-esteem,
and people who are dependent on and who have a strong need for approval from
others are also more conforming. [8] People who highly identify with or who have a high
degree of commitment to a group are also more likely to conform to group norms
than those who care less about the
group. [9] Despite these individual
differences
research has generally found that the impact of individual difference variables
on conformity is smaller than the influence of situational variables, such as
the size and unanimity of the majority.
We have seen that conformity usually occurs such that the opinions and behaviors
of individuals become more similar to the opinions and behaviors of the majority
of the people in the group. However, and although it is much more unusual, there
are cases in which a smaller number of individuals is able to
influence the opinions or behaviors of the larger group—a phenomenon
known as minority influence. Minorities who are consistent
and confident in their opinions may in some cases be able to be persuasive
. [10]
Persuasion that comes from minorities has another, and potentially even more
important, effect on the opinions of majority group members: It can lead
majorities to engage in fuller, as well as more divergent, innovative, and
creative thinking about the topics being
discussed. [11] Nemeth and Kwan [12] found that participants working together in groups solved
problems more creatively when only one person gave a different and unusual
response than the other members did (minority influence) in comparison to when
three people gave the same unusual response.
It is a good thing that minorities can be influential; otherwise, the world would
be pretty boring indeed. When we look back on history, we find that it is the
unusual, divergent, innovative minority groups or individuals, who—although
frequently ridiculed at the time for their unusual ideas—end up being respected
for producing positive changes.
Another case where conformity does not occur is when people feel that their
freedom is being threatened by influence attempts, yet they also have the
ability to resist that persuasion. In these cases they may develop a strong emotional reaction that leads people to resist
pressures to conform known as psychological
reactance. [13]
Reactance is aroused when our autonomy is
threatened.
Under these
conditions, people may
not conform at all, and may move their opinions or
behaviors away from the desires of the influencer. Consider an experiment
conducted by Pennebaker and Sanders, [14] who attempted to get people to stop writing graffiti on the walls of campus
restrooms. In the first group of restrooms they put a sign that read “Do not
write on these walls under any circumstances!” whereas in the second group they
placed a sign that simply said “Please don’t write on these walls.” Two weeks
later, the researchers returned to the restrooms to see if the signs had made a
difference. They found that there was significantly less graffiti in the second
group of restrooms than in the first one. It seems as if people who were given
strong pressures to not engage in the behavior were more likely to react against
those directives than were people who were given a weaker message.
Reactance represents a desire to restore freedom that is being threatened. A
child who feels that his or her parents are forcing him to eat his asparagus may
react quite vehemently with a strong refusal to touch the plate. And an adult
who feels that she is being pressured by a car salesman might feel the same way
and leave the showroom entirely, resulting in the opposite of the salesman’s
intended outcome.
learn by doing
Now that you are more familiar with the distinction between informational
conformity and normative conformity, we can apply these concepts to the studies
conducted by Sherif and Asch.
The behavior of Sherif’s participants is thought to be the result of
informational conformity, or the use of other people—their comments and
actions—as a source of information about what is likely to be correct. The task
Sherif asked his participants to perform was ambiguous, since the light doesn’t
move at all, but just appears to. And that appearance, being so uncertain and
ambiguous, is readily influenced by the expressed judgments of others.
Informational conformity is not thought to be the main source of conformity
pressure in Asch’s study, however. For the most part, the right answer was clear
to participants, as evidenced by the fact that individuals in a control group
who made these judgments by themselves, without any social pressure, almost
never made a mistake. Although some informational conformity likely was present,
the primary reason people conformed was to avoid standing out, negatively, among
the group members. That is, the behavior of Asch’s participants is thought to be
the result of normative conformity due to the desire to avoid the disapproval
and harsh judgments of others.
Informational conformity, by influencing how we come to see the issues or stimuli
before us, tends to influence our private acceptance of the position advanced by
the majority. Tending to assume that others have things right, we adopt the
group’s perspective. Normative conformity, in contrast, often has a greater
influence on public compliance than on private acceptance. To avoid disapproval,
we sometimes do or say one thing but continue to believe another.
learn by doing
Watch the video below on Milgram's study of obedience and answer the questions
that follow.
did I get this
Earlier in this module we reviewed research on helping behavior, or altruism. It
included a model proposed by Latané and Darley, who identified four steps
between an emergency and an individual providing help.
Referring to the following diagram, you will type in each step and submit your
response. Compare your response to the correct answer and then rate your
response. Do this for each step. To get the maximum learning benefit, do this
without consulting your notes or looking back at the text.

References
- Milgram, S., Bickman, L., and Berkowitz, L.
(1969).
"Note on the drawing power of crowds of different size." Journal of
Personality and Social Psychology. Volume 13. Number 2. 79–82 Pages.
- Cialdini, R. B., Reno, R. R., and Kallgren, C. A.
(1990).
"A focus theory of normative conduct: Recycling the concept of norms to
reduce littering in public places." Journal of Personality and Social Psychology. Volume 58. Number 6. 1015–1026 Pages.
- Cheng, C. M., and Chartrand, T. L.
(2003).
"Self-monitoring without awareness: Using mimicry as a nonconscious
affiliation strategy." Journal of Personality and Social Psychology. Volume 85. Number 6. 1170–1179 Pages.
- Sherif, M.
(1936).
The Psychology of Social Norms. Harper and Row. New York.
- Asch, S.
(1955).
"Opinions and social pressure." Scientific American. Volume 193. Number 5. 31–35 Pages.
- Milgram, S.
(1974).
Obedience to Authority: An Experimental View. Harper and Row. New York.
- Burger, M.
(2009).
"Replicating Milgram: Would people still obey today?." American Psychologist. Volume 64. Number 1. 1–11 Pages.
- Bornstein, R. F.
(1993).
The Dependent Personality. Guilford Press. New York.
- Jetten, J., Spears, R., and Manstead, A. S. R.
(1997).
"Strength of identification and intergroup differentiation: The influence
of group norms." European Journal of Social Psychology. Volume 27. Number 5. 603–609 Pages.
- Moscovici, S., Mugny, G., and Van Avermaet, E.
(1985).
Perspectives on Minority Influence. Cambridge University Press. New York.
- Martin, R., Hewstone, M., Martin, P. Y., and Gardikiotis,
A.
(2008).
Attitudes and Attitude Change. Chapter
Persuasion from majority and minority groups. Psychology Press. New
York. 361–384 Pages. W. D. Crano and R. Prislin (Eds.).
- Nemeth, C., and Kwan, J. L.
(1987).
"Minority influence, divergent thinking and the detection of correct
solutions." Journal of Applied Social Psychology. Volume 17. Number 9. 788–799 Pages.
- Miron, A. M., and Brehm, J. W.
(2006).
"Reaktanz theorie—40 Jahre sparer." Zeitschrift fur Sozialpsychologie. Volume 37. Number 1. 9–18 Pages.
- Pennebaker, J. W., and Sanders, D. Y.
(1976).
"American graffiti: Effects of authority and reactance arousal."
Personality and Social Psychology Bulletin. Volume 2. Number 3. 264–267
Pages.
Just as our primitive ancestors lived together in small social groups, including
families, tribes, and clans, people today still spend a great deal of time in groups. We
study together in study groups, we work together on production lines, and we decide the
fates of others in courtroom juries. We work in groups because groups can be beneficial.
A rock band that is writing a new song or a surgical team in the middle of a complex
operation may coordinate their efforts so well that it is clear that the same outcome
could never have occurred if the individuals had worked alone. But group performance
will only be better than individual performance to the extent that the group members are
motivated to meet the group goals, effectively share information, and efficiently
coordinate their efforts. Because these things do not always happen, group performance
is almost never as good as we would expect, given the number of individuals in the
group, and may even in some cases be inferior to that which could have been made by one
or more members of the group working alone.
In an early social psychological study, Norman Triplett [1] found that bicycle
racers who were competing with other bicyclers on the same track rode significantly
faster than bicyclers who were racing alone, against the clock. This led Triplett to
hypothesize that people perform tasks better when there are other people present than
they do when they are alone. Subsequent findings validated Triplett’s results, and
experiments have shown that the presence of others can increase performance on many
types of tasks, including jogging, shooting pool, lifting weights, and solving
problems. [2] The tendency to perform
tasks better or faster in the presence of others is known as social facilitation.
However, although people sometimes perform better when they are in groups than they do
alone, the situation is not that simple. Perhaps you remember an experience when you
performed a task (playing the piano, shooting basketball free throws, giving a public
presentation) very well alone but poorly with, or in front of, others. Thus it seems
that the conclusion that being with others increases performance cannot be entirely
true. The tendency to perform tasks more poorly or more slowly in the
presence of others is known as social inhibition.
Robert Zajonc [3] explained the observed influence of
others on task performance using the concept of physiological arousal. According to
Zajonc, when we are with others we experience more arousal than we do when we are alone,
and this arousal increases the likelihood that we will perform the dominant response, the action that we are most likely to emit in any given
situation.
The most important aspect of Zajonc’s theory was that the experience of arousal and the
resulting increase in the occurrence of the dominant response could be used to predict
whether the presence of others would produce social facilitation or social inhibition.
Zajonc argued that when the task to be performed was relatively easy, or if the
individual had learned to perform the task very well (a task such as pedaling a
bicycle), the dominant response was likely to be the correct response, and the increase
in arousal caused by the presence of others would create social facilitation. On the
other hand, when the task was difficult or not well learned (a task such as giving a
speech in front of others), the dominant response is likely to be the incorrect one, and
thus, because the increase in arousal increases the occurrence of the (incorrect)
dominant response, performance is hindered.
A great deal of experimental research has now confirmed these predictions. A
meta-analysis by Bond and Titus, [2] which looked at the results of over 200
studies using over 20,000 research participants, found that the presence of others
significantly increased the rate of performing on simple tasks, and also decreased both
rate and quality of performance on complex tasks.
Although the arousal model proposed by Zajonc is perhaps the most elegant, other
explanations have also been proposed to account for social facilitation and social
inhibition. One modification argues that we are particularly influenced by others when
we perceive that the others are evaluating us or competing with
us. [4] In one study supporting this idea, Strube, Miles, and
Finch [5] found that the presence of spectators increased joggers’ speed only
when the spectators were facing the joggers, so that the spectators could see the
joggers and assess their performance. The presence of others did not influence joggers’
performance when the joggers were facing in the other direction and thus could not see
them.
The ability of a group to perform well is determined by the characteristics of the group
members (e.g., are they knowledgeable and skilled?) as well as by the group process—that is, the events that occur while the
group is working on the task. When the outcome of group performance is better
than we would expect given the individuals who form the group, we call the outcome a group process gain, and when the group outcome is worse than we
would have expected given the individuals who form the group, we call the outcome a group process loss.
One group process loss that may occur in groups is that the group members may engage in social loafing, a group process loss that
occurs when people do not work as hard in a group as they do when they are working
alone. In one of the earliest social psychology experiments, in 1913,
Maximilien Ringelmann had
individual men, as well as groups of various numbers of men, pull as hard as they could
on ropes while he measured the maximum amount that they were able to pull. [6] As you can see in the figure below, although larger groups
pulled harder than any one individual, Ringelmann also found a substantial process loss.
In fact, the loss was so large that groups of three men pulled at only 85% of their
expected capability, whereas groups of eight pulled at only 37% of their expected
capability. This type of process loss, in which group productivity decreases as the size
of the group increases, has been found to occur on a wide variety of tasks.
learn by doing
Robert Zajonc [3] proposed a theory that would explain
both the social facilitation and the social inhibition study results. For this
activity, take a look at the figure above, titled "Drive-Arousal Model of Social
Facilitation." Zajonc’s theory has three components.
References
- Triplett, N.
(1898).
"The dynamogenic factors in pacemaking and competition." American
Journal of Psychology. Volume 9. Number 4. 507–533 Pages.
- Bond, C. F., and Titus, L. J.
(1983).
"Social facilitation: A meta-analysis of 241 studies." Psychological Bulletin. Volume 94. Number 2. 265–292 Pages.
- Zajonc, R. B.
(1965).
"Social facilitation." Science. Volume 149. Number 3681. 269–274 Pages.
- Baron, R.
(1986).
Advances in Experimental Social Psychology, Vol. 19. Chapter Distraction/conflict theory: Progress and problem. Academic Press. New York. 1–40 Pages. L. Berkowitz (Ed.).
- Strube, M. J., Miles, M. E., and Finch, W. H.
(1981).
"The social facilitation of a simple task: Field tests of
alternative explanations." Personality and Social Psychology Bulletin.
Volume 7. Number 4. 701–707 Pages.
- Kravitz, D. A., and Martin, B.
(1986).
"Ringelmann rediscovered: The original article." Journal of
Personality and Social Psychology. Volume 50. Number 5. 936–941 Pages.
Group process losses can also occur when group members conform to each other rather than
expressing their own divergent ideas. Groupthink is a phenomenon that occurs when a group made up of members who may be
very competent and thus quite capable of making excellent decisions nevertheless
ends up, as a result of a flawed group process and strong conformity pressures,
making a poor decision. [1] [2] Groupthink is
more likely to occur in groups whose members feel a strong group identity, when there is
a strong and directive leader, and when the group needs to make an important decision
quickly. The problem is that groups suffering from groupthink become unwilling to seek
out or discuss discrepant or unsettling information about the topic at hand, and the
group members do not express contradictory opinions. Because the group members are
afraid to express opinions that contradict those of the leader, or to bring in outsiders
who have other information, the group is prevented from making a fully informed
decision. The figure below summarizes the basic causes and outcomes of groupthink.
It has been suggested that groupthink was involved in a number of well-known and
important, but very poor, decisions made by government and business groups, including
the decision to invade Iraq made by President Bush and his advisors in 2002, the crashes
of two Space Shuttle missions in 1986 and 2003, and the decision of President John
Kennedy and his advisors to commit U.S. forces to help invade Cuba and overthrow Fidel
Castro in 1962. Analyses of the decision-making processes in these cases have documented
the role of conformity pressures.
As a result of the high levels of conformity in these groups, the group begins to see
itself as extremely valuable and important, highly capable of making high-quality
decisions, and invulnerable. The group members begin to feel that they are superior and
do not need to seek outside information. Such a situation is conducive to terrible
decision-making and resulting fiascoes.
Psychology in Everyday Life: Do Juries Make Good Decisions?
Although many other countries rely on judges to make judgments in civil and
criminal trials, the jury is the foundation of the legal system in the United
States. The notion of a “trial by one’s peers” is based on the assumption that
average individuals can make informed and fair decisions when they work together
in groups. But given the potential for group process losses, are juries really
the best way to approach these important decisions?
As a small working group, juries have the potential to produce either good or
poor decisions, depending on the outcome of the characteristics of the
individual members as well as the group process. In terms of individual group
characteristics, people who have already served on juries are more likely to be
seen as experts, are more likely to be chosen to be the jury foreman, and give
more input during the deliberation. It has also been found that status matters;
jury members with higher status occupations and education, males rather than
females, and those who talk first are more likely be chosen as the foreman, and
these individuals also contribute more to the jury discussion
. [3]
However, although at least some member characteristics have an influence on jury
decision making, group process plays a more important role in the outcome of
jury decisions than do member characteristics. Like any group, juries develop
their own individual norms, and these norms can have a profound impact on how
they reach their decision. Analysis of group process within juries shows that
different juries take very different approaches to reaching a verdict. Some
spend a lot of time in initial planning, whereas others immediately jump into
the deliberation. Some juries base their discussion around a review and
reorganization of the evidence, waiting to make a vote until it has all been
considered, whereas other juries first determine which decision is preferred in
the group by taking a poll and then (if the first vote does not lead to a final
verdict) organize their discussion around these opinions. These two approaches
are used quite equally but may in some cases lead to different
decisions. [4]
Perhaps most importantly, conformity pressures have a strong impact on jury
decision making. As you can see in the figure below, when there are a greater
number of jury members who hold the majority position, it becomes more and more
certain that their opinion will prevail during the discussion. This does not
mean that minorities can never be persuasive, but it is very difficult for them
to do so. The strong influence of the majority is probably due to both
informational conformity (i.e., that there are more arguments supporting the
favored position) and normative conformity (the people on the majority side have
greater social influence).
Given the potential difficulties that groups face in making good decisions, you
might be worried that the verdicts rendered by juries may not be particularly
effective, accurate, or fair. However, despite these concerns, the evidence
suggests that juries may not do as badly as we would expect. The deliberation
process seems to cancel out many individual juror biases, and the importance of
the decision leads the jury members to carefully consider the evidence
itself.
Using Groups Effectively
Taken together, working in groups has both positive and negative outcomes. On the
positive side, it makes sense to use groups to make decisions because people can
create outcomes working together that any one individual could not hope to
accomplish alone. In addition, once a group makes a decision, the group will
normally find it easier to get other people to implement it, because many people
feel that decisions made by groups are fairer than are those made by
individuals.
Yet groups frequently succumb to process losses, leading them to be less
effective than they should be. Furthermore, group members often don’t realize
that the process losses are occurring around them. For instance, people who
participate in brainstorming groups report that they have been more productive
than those who work alone, even if the group has actually not done that
well. [5] [6]
The tendency for group members to overvalue the
productivity of the groups they work in is known as the illusion of group productivity, and it seems to occur for
several reasons. For one, the productivity of the group as a whole is highly
accessible, and this productivity generally seems quite good, at least in
comparison to the contributions of single individuals. The group members hear
many ideas expressed by themselves and the other group members, and this gives
the impression that the group is doing very well, even if objectively it is not.
And, on the affective side, group members receive a lot of positive social
identity from their group memberships. These positive feelings naturally lead
them to believe that the group is strong and performing well.
What we need to do, then, is to recognize both the strengths and limitations of
group performance and use whatever techniques we can to increase process gains
and reduce process losses. The table below presents some of the techniques that
are known to help groups achieve their goals.
| Techniques That Can Be Used to Improve Group Performance |
|---|
| From Flat World Knowledge, Introduction to Psychology, CC-BY-NC-SA. |
| Technique |
Example |
| Provide rewards for performance. |
Rewarding employees and team members with bonuses will increase their
effort toward the group goal. People will also work harder in groups
when they feel that they are contributing to the group goal than when
they feel that their contributions are not important. |
| Keep group member contributions identifiable. |
Group members will work harder if they feel that their contributions to
the group are known and potentially seen positively by the other group
members than they will if their contributions are summed into the group
total and thus unknown. [7]
|
| Maintain distributive justice (equity). |
Workers who feel that their rewards are proportional to their efforts in
the group will be happier and work harder than will workers who feel
that they are
underpaid. [8]
|
| Keep groups small. |
Larger groups are more likely to suffer from coordination problems and
social loafing. The most effective working groups are of relatively
small size—about four or five members. |
| Create positive group norms. |
Group performance is increased when the group members care about the
ability of the group to do a good job (e.g., a cohesive sports or
military team). On the other hand, some groups develop norms that
prohibit members from working to their full potential and thus encourage
loafing. |
| Improve information sharing. |
Leaders must work to be sure that each member of the group is encouraged
to present the information that he or she has in group discussions. One
approach to increasing full discussion of the issues is to have the
group break up into smaller subgroups for discussion. |
| Allow plenty of time. |
Groups take longer to reach consensus, and allowing plenty of time will
help keep the group from coming to premature consensus and making an
unwise choice. Time to consider the issues fully also allows the group
to gain new knowledge by seeking information and analysis from outside
experts. |
| Set specific and attainable goals. |
Groups that set specific, difficult, yet attainable goals (e.g.,
“improve sales by 10% over the next 6 months”) are more effective than
groups that are given goals that are not very clear (e.g., “let’s sell
as much as we can!”). [9]
|
|
References
- Baron, R. S.
(2005).
Advances in Experimental Social Psychology, Vol. 37.
Chapter So right it’s wrong: Groupthink and the ubiquitous nature of
polarized group decision making. Elsevier Academic Press. San Diego.
219–253 Pages. M. P. Zanna (Ed.).
- Janis, I. L.
(2007).
Leadership: Understanding the Dynamics of Power and Influence in Organizations. Chapter Groupthink. University of Notre Dame Press. Notre Dame, IN. Edition 2. 157–169 Pages. R. P. Vecchio (Ed.).
- Stasser, G., Kerr, N. L., and Bray, R. M.
(1982).
The Psychology of the Courtroom. Chapter
The social psychology of jury deliberations: Structure, process and
product. Academic Press. New York. 221–256 Pages. N. L. Kerr and R. M.
Bray (Eds.).
- Davis, J. H., Stasson, M. F., Ono, K., and
Zimmerman, S.
(1988).
"Effects of straw polls on group decision making: Sequential voting
pattern, timing, and local majorities." Journal of Personality and
Social Psychology. Volume 55. Number 6. 918–926 Pages.
- Nijstad, B. A., Stroebe, W., and Lodewijkx, H.
F. M.
(2006).
"The illusion of group productivity: A reduction of failures
explanation." European Journal of Social Psychology. Volume 36. Number
1. 31–48 Pages.
- Stroebe, W., Diehl, M., and Abakoumkin, G.
(1992).
"The illusion of group effectivity." Personality and Social Psychology Bulletin. Volume 18. Number 5. 643–650 Pages.
- Szymanski, K., and Harkins, S. G.
(1987).
"Social loafing and self-evaluation with a social standard."
Journal of Personality and Social Psychology. Volume 53. Number 5.
891–897 Pages.
- Geurts, S. A., Buunk, B. P., and Schaufeli, W. B.
(1994).
"Social comparisons and absenteeism: A structural modeling
approach." Journal of Applied Social Psychology. Volume 24. Number 21.
1871–1890 Pages.
- Locke, E. A., and Latham, G. P.
(2006).
"New directions in goal-setting theory." Current Directions in
Psychological Science. Volume 15. Number 5. 265–268 Pages.
Picture yourself at your best and then picture the reality of your life. Is there a
difference? In your mind, are you managing the demands of the day, being effective at work
or school, and still have time for family and friends? Typically, throughout the trials of
a given day, people might fantasize about what it would mean to be in a state of “balance.”
Being in a state of balance means being mentally steady or
emotionally stable—having an internal state of harmony or symmetry.
With that definition,
balance becomes open to the interpretation that a person's “mental steadiness” is dependent
on his or her upbringing, culture, and lived experience.
 Photos, from left to right, courtesy of Bryan Gosline, Sacca, wheany, Alaskan Dude,
glasseyes
view, and granth
(CC-BY-2.0).
Photos, from left to right, courtesy of Bryan Gosline, Sacca, wheany, Alaskan Dude,
glasseyes
view, and granth
(CC-BY-2.0).
Take a moment and compartmentalize your life. Within your external “compartments,” does
balance include your job, your family, and social life? Within the internal “compartments,”
does your life include things such as a physical balance and spiritual balance? Also, are
the internal and external components of your life in balance with each other? As you can
see, the way that each of us answers these questions will be unique and intensely personal.
We can speak of balance in a general way, but, in the details, it is different for each
person.
What does “wellness” mean to you? If you were to ask a doctor, a counselor, a personal
trainer, or a nutritionist to define wellness, you are likely get answers that are similar
yet different.
Although it is a challenging term to define, for our purposes, wellness is a state of being in which a person actively
maintains a proper balance of physical, mental, emotional, and social health. This
definition may be described as a bio-psycho-social understanding of wellness. (You will
sometimes see this term written as "biopsychosocial." We will use hyphens to
separate bio, psycho, and social to emphasize the fact that there are separate sources of
influence.) It should come as no surprise that balance and optimal wellness go hand in
hand!
The Biology of Balance
There is a structure in the forebrain called the hypothalamus. The hypothalamus has
been referred to as the thermostat for the body because it is responsible for
maintaining homeostasis. Homeostasis is a technical term that
describes the goal of a system—like your body—that tries to maintain a constant or
optimal level of functioning. The hypothalamus is a system in the human brain that
tries to maintain homeostasis. When the hypothalamus functions properly, it monitors
temperature, fluids, metabolism, and level of nutrients to keep them at constant and
optimal
levels.
The hypothalamus plays a role for other forms of balance. In addition to acting as
the thermostat for the body, the hypothalamus also play a role in primary motivation.
For instance, motivations to drink, eat, and for sex are centered in the
hypothalamus. In addition, the hypothalamus aids in sleep as it contains a
substructure called the suprachiasmatic nucleus (SCN). The SCN is alert to light and
dark and, as such, helps establish the times of day where we feel energized and times
of day where we feel tired. When someone feels tired at night, the experience is due
to the SCN signaling the release of the hormone
melatonin.
Given that wellness is a multifaceted concept, we can think of it as having various
characteristics, also known as dimensions. This notion of wellness having dimensions was
first developed by Dr. Bill Hettler in 1976. His model is based on six dimensions:
physical, social, intellectual, spiritual, emotional, and occupational. [1]
Dimensions of wellness are often depicted as segments of a circle or wheel. Our model of
wellness will reflect external and internal dimensions as components of two, connected
“wellness wheels.” Let’s begin by looking at several important extrinsic characteristics
of wellness. These external characteristics are aspects of our lives outside of our
bodies and mind. Our External Wellness Wheel represents four characteristics: social,
occupational, environmental, and familial.
Social
According to John Bowlby, [2]
attachment theory emphasizes the influence parents have over a
child’s personality development. Consequently, a secure bond results in a secure
child who feels comfortable to explore the environment. The secure bond further
allows the child to become accustomed to, and later involved in, interpersonal
relationships. Overall, caregivers meeting a child’s early emotional needs have
long-lasting, positive social indicators. [3] [4] [5]
For instance, women showed both increased psychological well-being and social
competence when securely attached to both parent figures as they later
transitioned into college. [5]
Well-balanced social interactions are considered from a
developmental perspective. Specifically, gender differences start to appear in
childhood and continue into adolescence. For instance, behaviors of a socially
balanced female child include having emotionally closer relationships when
compared to males. In addition, their interactions tend to be more reciprocal.
Girls also tend to have peer relationships based on an intimate, emotional
exchange. Young boys, however, tend to be more outspoken with their friends, and
it is quite natural for male children to brag and interrupt conversations. Boys
are more physical in their activities, and their exchanges are based on shared
activities.
Well-balanced adult social interactions are more heterogeneous. In addition,
well-balanced social interactions in adults result in increased physical and
emotional health when compared to socially isolated adults. Adults who maintain
social connectedness tend to live longer; this finding is cross-cultural and
also crosses socioeconomic status.
Occupational
A focus of an industrial/organizational psychologist is to measure job
satisfaction. Overall, job satisfaction is positively correlated with age.
Another consistent observation is that those in more of an administrative role
are more satisfied than those who are not.
What might not be so obvious is the correlation between satisfaction and salary.
For instance, job satisfaction tends not to be related to pay for highly paid
workers. Instead, things such as job challenges, independence, and power tend to
be related to job satisfaction for these workers. In addition, how fairly one
believes he or she is paid is related more to job satisfaction than is actual
salary. People also tend to compare their salaries to those around them, and
workers tend to subjectively assess their comparable
worth.
Overall, the greatest factor influencing job satisfaction is whether or not the
job allows the person to use the professional or occupational skills in which he
or she is trained. Low job satisfaction is correlated with high job turnover
rates, and high job satisfaction is correlated with job longevity. Job
dissatisfaction has been correlated with both physical and psychological
consequences such as headaches, fatigue, anxiety, and depression. [6]
Environmental
In 1943, Abraham Maslow created his hierarchy of needs. He believed that the most
basic needs are at the bottom of the hierarchy, and each stage of the hierarchy
has to be satisfied in order to advance to, or feel motivated to achieve, the
next stage. The first needs to be satisfied are basic physiological needs
required for survival: air, food, and water. If these requirements are not met,
the human body cannot continue to function.
When physiological needs are met, the next priority is safety. This is the
environment in which the person lives. In an ideal world, a person lives in an
environment that is dominated by feelings of safety and security. In other
words, the person lives in a well-balanced environment, which sets the stage to
work on other needs within Maslow’s hierarchy. The remaining needs include love
and belonging (feeling accepted as an essential part of something, having
satisfying relationships), esteem (the need for self-respect and the respect of
others), and self-actualization (striving for and realizing one’s full
potential).
Safety needs set the foundation on which all other needs are achieved, and
threats to safety can shake that foundation. People experiencing danger, whether
immediate (e.g., during a war or natural disaster) or imminent (living in a
high-crime area), find it difficult or impossible to address the higher needs in
the hierarchy, such as self-improvement or maintaining healthy
relationships. [7]
Another example of how the environment can influence overall balance is found in
the diathesis-stress hypothesis, a theory of psychopathology that suggests that
certain psychological disorders, if biologically predisposed, can be triggered
by an unstable environment. For instance, numerous studies have found higher
rates of schizophrenia in urban areas and, conversely, lower rates of
schizophrenia in more rural areas. [8]
Familial
For the most part, humans are one of only a few species that maintain
relationships with others. Most nonhuman animals give birth to their young, and
as the animal develops, the mother and her young separate. Humans, on the other
hand, tend to be strongly tied to their families of origin.
In 1978, Mary Ainsworth created the “Strange Situation,” which involved having a
parent and child (age 12 to 18 months) together while the child explored an
unfamiliar environment. After some time, an unfamiliar person entered and spoke
with the parent, who then left the room. With the parent absent, the unfamiliar
person interacted with the child and later left the room. The parent returned,
interacted with the child, and left again. The child was now alone, and the
unknown person reentered and interacted with the child, and then the parent
reentered the room. The unknown person then left, and the Strange Situation had
ended. [9] [10]
The researchers gauged the reaction of each child in the study, which was
recorded, analyzed, and classified into one of four categories: secure,
insecure, avoidant/ambivalent, and disorganized/disoriented. Three of the
categories spoke to the child being off balance. Specifically, the child labeled
as anxious/avoidant showed disinterest in her environment, little distress when
the mother left, and avoided her when she returned. The anxious resistant child
was anxious in the presence of his mother, distressed when she left, and
ambivalent upon her return. The disorganized/disoriented child alternated
between avoidance and proximity seeking when the mother left. The behavior of a
disorganized/disoriented child included restricted movements in the presence of
the parent and rocking on hands and knees following the parent leaving. In
addition, this type of child moved away from the parent when frightened but also
screamed upon separation from the parent. [11] The securely attached, balanced child actively
pursued the environment and demonstrated age-appropriate social skills toward
the stranger. Although the child might have shown distress upon her mother
leaving, she sought her physical contact upon the mother's return.
The Strange Situation has been replicated and expanded to include how a child in
a given classification later functions as an adult. Based on responses to the
Adult Attachment Interview, there are three insecure attachment types and one
secure attachment type. Dismissing adults, for instance, do not believe that
human attachment is all that important. As a defense, such adults tend to
idealize memories of their childhood but cannot justify their claims with
concrete examples. Preoccupied adults tend to have relationships with their
parents that lack clear boundaries. As such, the adult might appear to have
anger and feel that any life issues are permanent. The Unresolved adults were
usually classified in the disorganized type of child. Such adults tend to have
been victims of abuse and neglect and have dysfunctional relationships as
adults. They also tend to have children that are classified as the disorganized
type.
It is the secure-autonomous adult that is the most balanced. Such adults feel
that relationships are something to be valued. They are able to reflect on their
parental bonds with objectivity and have rewarding relationships of their
own.
References
- Hettler, B.
(1976).
The six dimensions of wellness model. Retrieved from http://www.nationalwellness.org/pdf/SixDimensionsFactSheet.pdf.
- Bowlby, J.
(1988).
A Secure Base: Parent-Child Attachment and Healthy Human Development. Basic Books. New York.
- Mallinckrodt, B.
(1992).
"Childhood emotional bonds with parents, development of adult
social competencies, and availability of social support." Journal of
Counseling Psychology. Volume 39. Number 4. 453–461 Pages.
- Bell, N. J., Avery, A. W., Jenkins, D.,
Field, J., and Schoenrock, C. J.
(1985).
"Family relationships and social competence during late
adolescence." Journal of Youth and Adolescence. Volume 14. Number 2.
109–119 Pages.
- Kenney, M. E., and Donaldson, G. E.
(1991).
"Contributions of parental attachment and family structure to the
social and psychological functioning of first-year college students."
Journal of Counseling Psychology. Volume 38. Number 4. 479–486 Pages.
- O’Brien, G. E.
(1982).
"Evaluation of the job characteristics theory of work attitudes and
performance." Australian Journal of Psychology. Volume 34. Number 3.
383–401 Pages.
- Maslow, A. H.
(1999).
Toward a Psychology of Being. Wiley. New York. Edition 3.
- Rickman, M. D., and Davidson, R. J.
(1994).
"Personality and behavior in parents of temperamentally inhibited
and uninhibited children." Developmental Psychology. Volume 30. Number
3. 346–354 Pages.
- Connell, J. P., and Goldsmith, H. H.
(1982).
The Development of Attachment and Affiliative Systems.
Chapter A structural modeling approach to the study of attachment and
strange situation behaviors. Plenum. New York. 213–243 Pages. R. N. Emde
and R. J. Harmon (Eds.).
- Ainsworth, M. S., Blehar, M. C., Waters, E., and Wall, S.
(1978).
Patterns of Attachment: A Psychological Study of the Strange Situation. Lawrence Erlbaum Associates. Hillsdale, NJ.
- Owen, M. T., and Cox, M.
(1997).
"Marital conflict and the development of infant-parent attachment
relationships." Journal of Family Psychology. Volume 11. Number 2.
152–164 Pages.
Now that we’ve explored external characteristics of wellness, we can turn our attention
to several internal dimensions. These aspects of our lives are inherently tied to the
functioning of our bodies, minds, and spirits as we experience them as individuals.
Spiritual
God grant me the serenity
to accept the things I cannot change;
courage to change the things I can;
and wisdom to know the difference.
Living one day at a time;
Enjoying one moment at a time;
Accepting hardships as the pathway to peace;
Taking, as He did, this sinful world
as it is, not as I would have it;
Trusting that He will make all things right
if I surrender to His Will;
That I may be reasonably happy in this life
and supremely happy with Him
Forever in the next.
Amen.
This is the serenity prayer of 12-step programs such as Alcoholics Anonymous
(AA). This prayer is to be fully accepted in the 12 step program in order to
move on the subsequent steps. The serenity prayer is based on the concept of
balance. Let’s take a closer look at this prayer and decipher its latent
content: First is the concept of acceptance. More specifically, internalizing
the serenity prayer means fully accepting that some things are out of your
control. In the case of AA, it is accepting that one is powerless against
alcohol, surrendering the effort to control alcohol use, and instead seeking
guidance from a “higher power.”
Acceptance must take place nonjudgmentally—acknowledging that it is neither good
nor bad to have or not have control over some things. Complete acceptance of
powerlessness over alcohol, or over any stressor that is not within a person's
control, can lift an emotional weight from the person's shoulders.
Finally, the serenity prayer highlights the concept of mindfulness. To be mindful
is to be completely focused on the here and now—the present moment. To focus on
a moment that will be or on a moment that was is not being mindful of the present moment. True
mindfulness is a multisensory, present-focused orientation. Mindfulness helps a
person feel grounded.
In sum, to be in spiritual balance includes accepting present circumstances, or
the moment, in a nonjudgmental way. It also includes being focused on the
present rather than on the past or future.
Physical
The U.S. Department of Agriculture's Center for Nutrition Policy and Promotion
developed a balanced nutrition guide that replaces the well-known Food Pyramid
with a more practical dinner plate showing suggested serving sizes of four food
groups (20% fruits, 30% grains, 30% vegetables, and 20% proteins) and a glass
representing dairy. Unveiled in June 2011, MyPlate is the most recent
representation of over 100 years of nutrition guides. ChooseMyPlate.gov [1] is an interactive
website that includes ideas for daily food plans for children, adults, dieters,
and women who are pregnant or breastfeeding. It also contains advice on eating
healthy on a budget, food safety, physical activity, and other healthy-lifestyle
topics.
The benefits of a balanced diet are many, one of which is to provide the body
with energy for physical activity. The U.S. Department of Health and
Human Services (USDHHS) [2] recommends that, for adults, physical
exercise be divided into aerobic activity and strength training. For aerobic
activity (running, walking), the suggested time is 150 minutes per week of
moderate movement or 75 minutes per week of vigorous movement. Activities such
as mowing the lawn and brisk vacuuming also count as aerobic activity. Strength
training is recommended twice per week and can include activities such as rock
climbing and outdoor physical labor in addition to traditional weight machines.
The USDHHS also provides activity guidelines for children, adolescents, and
older adults.
The government suggestions for diet and exercise establish a good foundation for
physical wellness. Along with a healthy diet and exercise, the government
recommends that all Americans have an annual wellness checkup.
Intellectual
Intellectual wellness and balance is more of an active and challenging process.
To achieve intellectual balance is to feel temporarily unbalanced. For instance,
Lee Vygotsky was a Russian psychologist in the early 1920s. He stated that
intellectual growth in children occurred within the social environment and on
two levels, with assistance from others and within the child. Vygotsky coined a
process called “zone of proximal development.” This is a space between what a
child can cognitively achieve on his own and what he can achieve with
assistance. The process of working within this space is called “scaffolding” and
is where both intellectual growth and age-appropriate intellectual imbalance
occur. So in a sense, intellectual balance is interrupted and later
reestablished once a new concept is grasped.
This process of scaffolding can also occur as adults, although the process is
much more self initiated. In other words, opportunities for intellectual growth
can occur in the workplace, during social interactions, or reading about topics
of interest. As adults become older, the lifelong process of gaining knowledge
and responding to intellectual stimuli manifests into a sense of wisdom.
Psychologist Erik Erikson stated that as adults enter old age, they reflect upon
their lives. If older persons can reflect upon their lives and feel that their
lives were meaningful, a sense of integrity develops . Through satisfaction and
integrity, older adults perceive a sense of wisdom that they can impart on to
others. [3]
Emotional
Like it or not, we all have emotions that need to be expressed. From the
perspective of evolution, for example, humans need to respond to fear in order
to survive. From a cultural perspective, emotions can be nonverbal methods of
communication. For example, there are certain types of universal emotions that
cross cultures. In other words, one person may not be able to understand a
spoken language, but that same person would be able to understand feelings
states in another person. Research suggests that there are six basic emotions
that, no matter what culture, can be accurately interpreted. The six basic,
universal emotions are fear, anger, joy, sadness, surprise, and disgust.
From a biological perspective, emotional stimuli are processed in the brain.
Specifically, the limbic system, located in the forebrain, contains structures
that include the amygdala, septum, and hippocampus. The amygdala helps assign
emotional intensity to a given situation and helps us channel emotional
energy into a behavior, most notably anger and aggression. The septum inhibits
emotions: Damage to this area in animals has resulted in “septal rage syndrome,”
which involves inhibition of rage. Finally, the hippocampus is less related to
emotion and more related to memory.
From a balanced perspective, Marsha Linehan [4] talked about being
in “wise mind.” Linehan developed a treatment model for those diagnosed with
borderline personality disorder, the hallmark of which is emotional instability.
Wise mind, which is the goal of this treatment also known as dialectical
behavior therapy (DBT), means that one is fully aware of the experience of an
emotion. For instance, the tightening of the chest for anxiety, or the physical
heaviness of sadness, are cues that should be responded to in such a way that it
helps process an emotion. At the very least, in cases where there is nothing
that can be done about the emotional situation, being in wise mind will help
temporarily distract a person from the emotion.
References
- U.S. Department of Agriculture, Center for Nutrition Policy and Promotion.
(2011).
ChooseMyPlate.gov. Retrieved from http://www.ChooseMyPlate.gov.
- U.S. Department of Health and Human Services.
(2008).
Physical Activity Guidelines for Americans. Retrieved from http://www.health.gov/paguidelines/.
- Erikson, E. H.
(1963).
Childhood and Society. Norton. New York. Edition 2.
- Linehan, M.
(1993).
Skills Training Manual for Treating Borderline Personality Disorder. Guilford Press. New York.
Picture in your mind the most beautiful lawn you have ever seen: Lush, thick green grass
is nicely manicured, and all blades of grass are of equal length. Did you ever wish your
lawn could be like this? Or did you ever think, “That’s what my lawn is going to look
like?” Overall, proper lawn maintenance depends on the type of grass, such as cool
season and warm season grass. Proper lawn care also includes knowing what to do at a
given time of year. There is basic lawn care that includes mowing, watering, and removal
of small weeds by hand. Proper lawn care also includes grub control, patching, feeding,
and thatching. It also includes maintenance of your lawn mower so dull blades do not
“split” the grass blades. Most important, to maintain a healthy lawn requires active
attention to the soil, including monitoring the pH balance. In other words, lawn care is
not a passive process.
In reality, most homeowners do not monitor the pH of the soil, despite this being
instrumental in overall lawn health. Much like having a healthy lawn, it is also
important to take that same active approach to maintain personal balance. However,
people tend to take a more passive approach to self-care, often attempting to balance
external demands at the expense of their own physical and mental well-being. Consider
your own personal wellness wheel and its individual components.
In broad strokes, it seems that not enough time exists to do things that would create
more balance. Specifically, if a you work 8 hours per day, then must take care of other
external demands such as school, afterschool activities for children, and making dinner
for the family, not much time is left for taking care of personal balance. The more
demands placed on a person, the more likely that person will not make time for
self-care. This can almost be ironic in that, considering the internal and external
wellness wheels, a person would be able to better manage the demands of life if both
internal and external wellness wheels were balanced with each other.
Having said that, there is also balance to self-care. In other words, some people may
take too much self time at the expense of external demands. In other words, after
working 40 hours and playing golf on Saturdays and watching football on Sunday, a
person's relationships may be negatively impacted because of limited attention to family
(if family is included in a person's definition of wellness).
With moderation, personal needs are extremely important for balance because meeting those
needs makes a person more effective in managing external demands. People can create
their own individualized wellness wheel to include physical health, physical exercise,
eating and sleeping habits, and personal time for hobbies.
The first module discussed being in balance. This module discusses maintaining
balance and moving toward optimal balance. As mentioned in the previous module,
overall wellness is comprised of lifestyle and choices. Another aspect to add
is acceptance as this would be a starting point for moving back towards
wellness. Acceptance is required because it allows a person to accept where he
is at a particular moment, as opposed to becoming overwhelmed with where he
wishes he could be, where he was at one point in time, or how he perceives
others to be. Acceptance does not necessarily mean that a person loves where he
is at that moment. Rather, indicates accepting responsibility for he is at that
moment. In other words, he may not love what the doctor has to say about the
number on the scale, but he is willing to take responsibility for it and create
goals. An example of a personal starting point would be the self-care report
card activity that was completed in the previous module.
While reviewing the self-care report card, it is important to be aware of
maintaining the balance of staying challenged while not becoming overwhelmed.
This also applies to life goals as feeling overwhelmed can create the natural
tendency to want to “shut down.” In other words, feeling that there is so much
to do that nothing gets done. A first intervention is to recognize the
connection between the mind and body.
An overall objective of this module is to learn how the mind-body connection
contributes to moving back to, and then ultimately staying in, balance. The
principles of the mind-body connection will become more specific as the module
progresses, however, the following video and activity provides an
introduction to the mind body connection.
learn by doing
Watch this video and answer the questions that follow.
Moving back into balance might not be easy, and the hardest part can be getting started.
In some cases, mental health intervention may be warranted.
We have seen that psychologists and other practitioners employ a variety of treatments in
their attempts to reduce the negative outcomes of psychological disorders. But we have
not yet considered the important question of whether these treatments are effective, and
if they are, which approaches are most effective for which people and for which
disorders. Accurate empirical answers to these questions are important as they help
practitioners focus their efforts on the techniques that have been proven to be most
promising, and will guide societies as they make decisions about how to spend public
money to improve the quality of life of their citizens. [1]
Psychologists use outcome research. Studies that assess the effectiveness of medical
treatments., that is, studies that assess the effectiveness of medical treatments, to
determine the effectiveness of different therapies. Thousands of studies have been
conducted to test the effectiveness of psychotherapy, and by and large they find
evidence that it works. Some outcome studies compare a group that gets treatment with
another (control) group that gets no treatment. For instance, Ruwaard, Broeksteeg,
Schrieken, Emmelkamp, and Lange [2] found that patients who interacted with a
therapist over a website showed more reduction in symptoms of panic disorder than did a
similar group of patients who were on a waiting list but did not get therapy. Although
studies such as this one control for the possibility of natural improvement (the
treatment group improved more than the control group, which would not have happened if
both groups had only been improving naturally over time), they do not control for either
nonspecific treatment effects or for placebo effects. The people in the treatment group
might have improved simply by being in the therapy (nonspecific effects), or they may
have improved because they expected the treatment to help them (placebo effects).
Another type of outcome study compares different approaches with each other. For
instance, Herbert and colleagues [3] tested whether social skills training
could boost the results received for the treatment of social anxiety disorder with
cognitive-behavioral therapy (CBT) alone. As you can see in Figure 13.11, they found
that people in both groups improved, but CBT coupled with social skills training showed
significantly greater gains than CBT alone. A more in depth description of CBT is
described below.
Research Focus: Meta-Analyzing Clinical Outcomes
Because there are thousands of studies testing the effectiveness of
psychotherapy, and the independent and dependent variables in the studies vary
widely, the results are often combined using a meta-analysis. A meta-analysis is
a statistical technique that uses the results of existing studies to integrate
and draw conclusions about those studies. In one important meta-analysis
analyzing the effect of psychotherapy, Smith, Glass, and Miller [4]
summarized studies that compared different types of therapy or that compared the
effectiveness of therapy against a control group. To find the studies, the
researchers systematically searched computer databases and the reference
sections of previous research reports to locate every study that met the
inclusion criteria. Over 475 studies were located, and these studies used over
10,000 research participants.
The results of each of these studies were systematically coded, and a measure of
the effectiveness of treatment known as the effect size was created for each
study. Smith and her colleagues found that the average effect size for the
influence of therapy was 0.85, indicating that psychotherapy had a relatively
large positive effect on recovery. What this means is that, overall, receiving
psychotherapy for behavioral problems is substantially better for the individual
than not receiving therapy.
Other meta-analyses have also found substantial support for the effectiveness of
specific therapies, including cognitive therapy, CBT [5] [6]
couples and family therapy [7] and psychoanalysis. [8] On the basis of these and
other meta-analyses, a list of empirically supported therapies—that is,
therapies that are known to be effective—has been developed. [9] [10]
These therapies include cognitive therapy and behavioral therapy for depression;
cognitive therapy, exposure therapy, and stress inoculation training for
anxiety; CBT for bulimia; and behavior modification for bed-wetting.
Smith, Glass, and Miller [4] did not find much evidence that any one type
of therapy was more effective than any other type, and more recent meta-analyses
have not tended to find many differences either. [11] What this means is that a good part of
the effect of therapy is nonspecific, in the sense that simply coming to any
type of therapy is helpful in comparison to not coming. This is true partly
because there are fewer distinctions among the ways that different therapies are
practiced than the theoretical differences among them would suggest. What a good
therapist practicing psychodynamic approaches does in therapy is often not much
different from what a humanist or a cognitive-behavioral therapist does, and so
no one approach is really likely to be better than the other.
What all good therapies have in common is that they give people hope; help them
think more carefully about themselves and about their relationships with others;
and provide a positive, empathic, and trusting relationship with the
therapist—the therapeutic alliance. [12] This is why
many self-help groups are also likely to be effective and perhaps why having a
psychiatric service dog may also make us feel better.
The idea of the mind-body connection is the foundation of cognitive-behavioral
therapy (CBT). The power of the mind is always interesting. Two people can wake
up on a given day and go to the same job. However, the way one thinks about the
job can affect his or her mood that day. For instance, one person can think,
“This job will never get better” while the other person thinks, “This is how I’m
going to make my job better.” Based on the thoughts, one person can feel
depressed while the other feels optimistic. In moving toward wellness using CBT,
the focus is on changing thoughts that create undesired emotions so to minimize
their intensity. This type of therapy is widely utilized in mental health
settings.
Consider the following table:
| Trigger |
Running late for work and behind a slow driver |
Running late for work and behind a slow driver |
| Thoughts |
“I can’t believe that I’m going to be late"; "It figures, I always get
behind someone going slow when I’m running later"; "This idiot won’t
move." |
"It's a good thing I haven’t been late this year"; "Let me give the
office a call and let them know I’ll be a little late." |
| Feelings |
Anger/frustration |
Contentment/mild frustration |
| Behavior |
Tailgate the driver; flash high beams |
Stay at a safe distance; wait for a safe moment to pass |
| Consequences |
Possible ticket, accident; possible bad mood for the rest of the day |
Get to work a little late with the boss already knowing |
As you can see, there is a domino effect in that triggers create automatic
thoughts, which create feelings, that create behavior, that create consequences.
Sometimes, there is no control over the trigger (such as being behind a slow
driver), but recognizing automatic thoughts and then knowing how to change them
is where a person has control.
Of course, when moving toward emotional wellness, there are therapeutic
interventions that do not necessarily have to include psychotherapy. At present,
there is a movement that incorporates more Eastern approaches to emotional
balance. Once such intervention, or rather, way of life, is the concept of
mindfulness.
learn by doing
Watch the following video and answer the questions.
Although the video states that mindfulness is a “program,” there are likely
episodes of mindfulness that are experienced on a daily basis. Simply stated, to
be mindful is to do one thing at a time with all energy and focus on that one
thing. The ability to be mindful is enhanced when it becomes a multi sensory
experience. For instance, some children and adolescents mindfully play video
games. Playing video games is multisensory, as it incorporates sight, sound, and
touch (manipulating the controller). Adults practice mindfulness when they
become “lost” in a good book or while lying on the beach. No matter how
mindfulness is experienced, it allows a person to be fully conscious of an
experience and serve as a temporary distraction from stressors. Other examples
of mindful experiences can include: petting the dog, taking a hot bath with
scented oils and candles, walking outside and being mindful of the trees
rustling and the wind in your face. Did you ever ask yourself, “Where did the
time go?” or say to yourself, “Wow! I can’t believe this is over already.” That
is likely because you were experiencing mindfulness.
References
- Hunsley, J., and Di Giulio, G.
(2002).
"Dodo bird, phoenix, or urban legend? The question of psychotherapy
equivalence." Scientific Review of Mental Health Practice. Volume 1.
Number 1. 11–22 Pages.
- Ruwaard, J., Broeksteeg, J., Schrieken,
B., Emmelkamp, P., and Lange, A.
(2010).
"Web-based therapist-assisted cognitive behavioral treatment of
panic symptoms: A randomized controlled trial with a three-year
follow-up." Journal of Anxiety Disorders. Volume 24. Number 4. 387–396
Pages.
- Herbert, J. D., Gaudini, B. A., Rheingold,
A. A., Myers, V. H., Dalrymple, K., and Nolan, E. M.
(2005).
"Social skills training augments the effectiveness of cognitive
behavioral group therapy for social anxiety disorder." Behavior Therapy.
Volume 36. Number 2. 125–138 Pages.
- Smith, M. L., Glass, G. V., and Miller, R. L.
(1980).
The Benefits of Psychotherapy. Johns Hopkins University Press. Baltimore.
- Butler A. C., Chapman, J. E., Forman, E.
M., Beck, A. T.
(2006).
"The empirical status of cognitive-behavioral therapy: A review of
meta-analyses." Clinical Psychology Review. Volume 26. Number 1. 17–31
Pages.
- Deacon, B. J., and Abramowitz, J. S.
(2004).
"Cognitive and behavioral treatments for anxiety disorders: A
review of meta-analytic findings." Journal of Clinical Psychology.
Volume 60. Number 4. 429–441 Pages.
- Shadish, W. R., and Baldwin, S. A.
(2002).
Effectiveness Research in Marriage and Family Therapy.
Chapter Meta-analysis of MFT interventions. American Association for
Marriage and Family Therapy. Alexandria, VA. 339–370 Pages. D. H.
Sprenkle (Ed.).
- Shedler, J.
(2010).
"The efficacy of psychodynamic psychotherapy." American Psychologist. Volume 65. Number 2. 98–109 Pages.
- Chambless, D. L., and Hollon, S. D.
(1998).
"Defining empirically supported therapies." Journal of Consulting
and Clinical Psychology. Volume 66. Number 1. 7–18 Pages.
- Hollon, S., Stewart, M., and Strunk, D.
(2006).
"Enduring effects for cognitive therapy in the treatment of
depression and anxiety." Annual Review of Psychology. Volume 57. Number
1. 285–316 Pages.
- Cuijpers, P., van Straten, A., Andersson,
G., and van Oppen, P.
(2008).
"Psychotherapy for depression in adults: A meta-analysis of
comparative outcome studies." Journal of Consulting and Clinical
Psychology. Volume 76. Number 6. 909–922 Pages.
- CuijAhn, H.-N., and Wampold, B. E.
(2001).
"Where oh where are the specific ingredients? A meta-analysis of
component studies in counseling and psychotherapy." Journal of
Counseling Psychology. Volume 48. Number 3. 261–257 Pages.
Healthy Living
There are many activities that can have a positive impact on your
well-being and help you maintain balance in your life.
learn by doing
You’ve been introduced to the concept of mindfulness and how a
meditation practice can help you develop and deepen this form of
awareness.
The following videos offer you an opportunity to explore two common styles of
meditation. The first short video will take you through a body-scan guided
meditation. The second short meditation focuses on the repeated utterance of a
single sound.
Try the guided meditation in this first video and then reflect on
the question that follows. You’ll need about five minutes for the
meditation. Find a quiet, comfortable place, and then start the
video.
What did you experience physically, emotionally, and mentally as
you did the body scan guided meditation?
Give yourself a little time between doing the body-scan guided
meditation and trying the next meditation technique.
This is a short meditation during which you’ll repeat a single
word. Find a quiet place where you feel comfortable speaking aloud.
When you’re ready, begin the video.
What was your experience of meditating on a sound that you made
over and over again? How did this type of meditation influence your
focus and attention?
learn by doing
One of the most well-known forms of movement meditation is yoga.
This ancient practice is focused on integrating your breathing with
movements of your body into and out of different postures, called
asanas. This is one of the primary reasons yoga is a form of
meditation rather than a type of calisthenics.
There are several different schools of yoga, such as Hatha, Vinyasa, Iyengar,
and Kundalini. Many asanas are found in all of these styles of yoga. The
posture known as Downward-Facing Dog is one such asana.
The following video demonstrates how to do Downward-Facing Dog. Give it a
try!
Remember: Go into the posture as much as your
body allows. Don’t force your heels to the floor. If you need to,
bend your knees. And, breathe!
Build and Maintain Healthy Relationships
A final concept with moving back into wellness is to be mindful of having a good
support system in place. Ideally, a support system would include having healthy
relationships. That being said, healthy relationship are not just formed. They are
formed and developed through working on them. (FWK) When good friendships develop,
when people get married and plan to spend the rest of their lives together, and when
families grow closer over time, the relationships take on new dimensions and must be
understood in somewhat different ways. Although humans seem to be the only animals
that are able to develop close relationships in which partners stay sexually faithful
to each other for a lifetime, [1] these
relationships do not come easily. About one half of contemporary marriages in the
United States and Canada end in divorce. [2]
The factors that keep people liking each other in long-term relationships
are at least in part the same as the factors that lead to initial
attraction. For instance, regardless of how long they have been together,
people remain interested in the physical attractiveness of their
partners, although it is relatively less important than for initial
encounters. And similarity remains essential. Relationships are also more
satisfactory and more likely to continue when the individuals develop and
maintain similar interests and continue to share their important values
and beliefs over time. [3] Proximity
also remains important—relationships that undergo the strain of the
partners’ being apart from each other for very long are more at risk for
breakup.
But what about passion? Does it still matter over time? Yes and no.
People in long-term relationships who are most satisfied with their
partners report that they still feel passion for their partners—they
still want to be around them as much as possible, and they enjoy making
love with them. [4] [5] And partners
report that the more they love their partners, the more attractive they
find them. [6] On the
other hand, the high levels of passionate love that are experienced in
initial encounters are not likely to be maintained throughout the course
of a long-term relationship. [7] Over
time, cognition becomes relatively more important than emotion, and close
relationships are more likely to be based on companionate love, which is love that
is based on friendship, mutual attraction, common interests, mutual
respect, and concern for each other’s welfare.
Consider the following benefits of having a good, healthy long-term
relationship as reported by the U.S. Department of Health and Human Services.
For Women
Researchers have found many benefits for women who are in healthy
marriages, compared to unhealthy marriages, including the following:
- More satisfying relationship
- Emotionally healthier
- Wealthier
- Less likely to be victims of domestic violence, sexual assault, or
other violent crimes
- Less likely to attempt or commit suicide
- Decrease risk of drug and alcohol abuse
- Less likely to contract STDs
- Less likely to remain or end up in poverty
- Have better relationships with their children
- Physically healthier
For Men
Researchers have found many benefits for men who are in healthy
marriages, compared to unhealthy marriages, including the following:
- Live longer
- Physically healthier
- Wealthier
- Increase in the stability of employment
- Higher wages
- Emotionally healthier
- Decrease risk of drug and alcohol abuse
- Have better relationships with their children
- More satisfying sexual relationship
- Less likely to commit violent crimes
- Less likely to contract STDs
- Less likely to attempt or commit suicide
It should be noted that having healthy relationship is not just considered in
marriages and long-term relationships. For instance, a relationship with a therapist
should be healthy, but it is also temporary. Other examples of having relationships
include those that people have with their relatives, neighbors, employees or co
workers, and church members.
References
- Barash, D. P., and Lipton, J. E.
(2002).
Gender Gap: The Biology of Male-Female Differences. Transaction Publishers. Piscataway, NJ.
- Centers for Disease Control and Prevention.
(2010).
Marriage and divorce. Retrieved from http://www.cdc.gov/nchs/fastats/divorce.htm.
- Davis, J. L., and Rusbult, C. E.
(2001).
"Attitude alignment in close relationships." Journal of Personality
and Social Psychology. Volume 81. Number 1. 65–84 Pages.
- Simpson, J. A.
(1987).
"The dissolution of romantic relationships: Factors involved in
relationship stability and emotional distress." Journal of Personality
and Social Psychology. Volume 53. Number 4. 683–692 Pages.
- Sprecher, S.
(2006).
Close Relationships: Functions, Forms and Processes.
Chapter Sexuality in close relationships. Psychology Press/Taylor and
Francis. Hove, England. 267–284 Pages. P. Noller and J. A. Feeney
(Eds.).
- Simpson, J. A., Gangestad, S. W., and Lerma,
M.
(1990).
"Perception of physical attractiveness: Mechanisms involved in the
maintenance of romantic relationships." Journal of Personality and
Social Psychology. Volume 59. Number 6. 1192–1201 Pages.
- Acker, M., and Davis, M. H.
(1992).
"Intimacy, passion and commitment in adult romantic relationships: A
test of the triangular theory of love." Journal of Social and Personal
Relationships. Volume 9. Number 1. 21–50 Pages.
If you have ever been on a plane, you have seen the safety instructions provided by the flight
attendants. First, someone from the flight crew directs passengers to the Fasten Seat
Belt sign and reminds them to stow any carry-on luggage underneath the seat in front of
you or in an overhead bin. Flight attendants also remind passengers to put seats back
and folding trays in the upright position. Selected passengers are then reminded that
those who are seated next to an emergency exit should read the instruction card and are
then given the opportunity to move their seat if they do not wish to assume such a
responsibility. Flight crew will also remind passengers that the flight is a nonsmoking
one and that all electronic devices should be turned off until a certain altitude is
reached.
Most relevant to this module is the part when flight attendants remind passengers that if there
is a loss of cabin pressure, oxygen masks will descend. They then demonstrate to
passengers how to place them over their nose and mouth. They also remind passengers to
place their own masks on before assisting anyone else. In other words, a passenger has
to place his own mask on before he can help the 3-year-old next to him.
The moral of the above is that flight passengers are ineffective if they are passed out.
It is the same thing in life in that being out of balance can make a person ineffective.
As such, it is important for people to be mindful of when they are feeling out of
balance.
Thus far in our discussion of wellness, we’ve characterized wellness as having eight
dimensions: four of them associated with external aspects of our lives and the other
four rooted in our individual bodies, minds, and spirits. We’ve also emphasized that our
own sense of wellness is dynamic and, as such, something we each must actively engage in
if we want to be well. The introduction to this section also
reminds us that awareness of and openness to what is happening in our lives, as well as
how we are acting and reacting within each moment, determines the overall sense of
balance we experience.
Sounds simple, right? Maintaining balance among these various facets of our lives should be
easy! Yet, we all know, it’s not. Events occur that can demand our attention and consume
our energy. Negative emotions take hold that can cloud our outlook and judgment.
Physical symptoms can appear that can indicate our bodies are in distress. These things
are going to happen. We will become “out of balance” throughout the day...throughout our
lives. Only when we are mindful of any imbalances can we first consider options that
will effectively address our needs, and then choose to act on those that will move us
toward balance and well-being.
In this section, we continue to use our internal and external wellness wheels to explore the
concept of imbalance in each of the eight dimensions previously described.
learn by doing
In the previous section, we developed an external and an internal wellness wheel. The
external wheel consists of the four dimensions: social, environmental,
occupational, and family. The internal wheel represents the physical, emotional,
intellectual, and spiritual dimensions of wellness. As we begin to discuss the
characteristics of imbalance with respect to wellness, let’s use these wheels to
explore this concept in an interactive way.
Now that you’re aware of the dynamic and connected nature of these eight facets of wellness,
particularly when one or more of these dimensions is out of balance, try to
answer the following set of questions.
The consequences for being physically out of balance are numerous. On the positive side
of this, the world balance does not have to mean walking on a tightrope. Rather the
world balance is comprised of, for the most part, choices and lifestyle. Those choices
and lifestyles will be discussed in the next module, however, as this module discusses
the consequences of poor choices and unhealthy lifestyle.
The World Health Organization (WHO) is the world’s leading institution in reporting
health-related news and statistics. It is considered an online database that also
conducts research, establishes health related policies, and monitors trends in worldwide
health. According to the World Health Organization (WHO), the rates of worldwide obesity
have more than doubled since 1980. Specifically, 1.5 billion adults over the age of 20
were estimated to be overweight in 2008. Of this 1.5 billion, 500 million men and women
were classified in the obese range. The World Health Organization estimates that in
2010, 43 million children under the age of five were overweight. [1]
With obesity come health consequences. The WHO states a positive correlation between
degree of being overweight and health consequences. For instance, as a person becomes
more overweight, the risk rises for cardiovascular diseases such as heart disease and
stroke, type 2 diabetes, osteoarthritis, and certain types of cancers such as
endometrial, breast, and colon cancers. [2] As weight
increases, a person potentially decreases the number of years that he or she lives. In
the case of women, the chances of becoming pregnant decrease.
learn by doing
Watch the video and answer the following questions about obesity.
On the other side of the out of balance physical well-being continuum is the presence of
certain eating disorders. Although eating disorders are primarily associated with women
and girls, there has been more of a social awareness in boys and men. [3] Overall, there is a lag between the social awareness
of males with eating disorders and the medical model of diagnosis. Specifically, the Diagnostic and Statistical Manual of Mental Disorders, Fourth
Edition-Text Revision (DSM-IV-TR) is the book that mental health clinicians use
to diagnose psychological disorder. It lists four criteria for anorexia nervosa. Of the
four, one is focused on females (which is amenorrhea or the absence of at least three
consecutive menstrual cycles), which contributes to an underreporting of the prevalence
of anorexia in males.
That being said there are some available statistics for anorexia in males. For instance,
about 10-15% of people with anorexia or bulimia are male and, as noted above, this may
be an under representation of the population due to the diagnostic criteria and men
being less likely to seek treatment for a “woman’s disease.” [4] [5]
Despite the skewed statistics and the medical lag in diagnostic accuracy, what is known
about males with anorexia is that they have some similar psychological experiences with
females. For instance, females and males experience a distorted body image. Another
similarity is that recovery from anorexia is long for both genders, and there is a
significant vulnerability for relapse if the proper supports and services are not in
place. [6]
As noted above, there is a similarity between men and women in that both suffer from
distorted perceptions their bodies. However, there is a difference between how the
distorted body image is manifested. Specifically, males are more likely to suffer from
muscle dysmorphia, which is defined as being overly concerned with being more muscular.
This is in contrast to females who primarily are interested in losing weight. So, while
a female with anorexia has a desire to be thinner than she believes she is, a male might
have a desire to appear more muscular than he is.
There are both medical and psychological consequences of anorexia that can occur between
genders. The most severe outcome is death. In addition, abnormal heart rhythms
(arrhythmias) can occur as can anemia (where the body does not have enough healthy red
blood cells which can result in chest pain, fatigue, headaches, and difficulty
concentrating), gastrointestinal problems (such as constipation, bloating or nausea),
kidney problems, and irreversible organ damage. From a psychological perspective,
anorexia can contribute to, or magnify, symptoms of depression and anxiety
disorders.
It should be noted that there are still consequences for physical imbalance that lie in
between the continuum of anorexia and obesity. This will be addressed in the section on
the consequences of being emotionally out of balance.
References
- World Health Organization.
(2012).
Obesity and overweight. Retrieved from http://www.who.int/mediacentre/factsheets/fs311/en/.
- World Health Organization.
(2006).
What are the health consequences of being overweight?. Retrieved from http://www.who.int/features/qa/49/en/index.html.
- National Institute of Mental Health.
(2011).
Eating disorders: How are males affected?. Retrieved from http://www.nimh.nih.gov/health/publications/eating-disorders/how-are-males-affected.shtml.
- American Psychiatric Association
(2000).
Diagnostic and Statistical Manual of Mental Disorders. Author. Washington, DC. Edition 4, text rev.
- National Association of Anorexia Nervosa and Associated Disorders.
(2012).
Eating disorders statistics. Retrieved from http://www.anad.org/get-information/about-eating-disorders/eating-disorders-statistics/.
- Rich, M.
(2012).
Male anorexia. Retrieved from
http://www.life123.com/parenting/tweens-teens/anorexia/anorexia-in-men.shtml.
Dialectical behavior therapy (DBT) is a type of therapy developed by Marsha M.
Linehan [1]
at the University of Washington. DBT is based on three states of mind:
reasonable mind, wise mind, and emotional mind. People are in reasonable mind when they
take a more intellectual approach to life. Reasonable mind includes the ability to think
logically and focus solely on facts. While in reasonable mind, people are “cool" in
their approach. On the opposite end of the spectrum, people can be in emotional mind,
which is when thinking and behavior are emotionally based. Any attempts at logic can be
futile because thoughts can be nonfacts and further fuel emotions. While reasonable mind
takes a “cool” approach, thoughts and behaviors in emotional mind are "hot." Finally, a
person is in wise mind when there is an overlap of reasonable mind and emotional mind.
In other words, a people are aware of escalating emotions but have not lost touch with
logic. While some people can engage in unhealthy behaviors as a result of being in
emotional mind, those in wise mind are able to recognize potential long term
consequences of acting on pure emotions.
DBT also teaches methods of regulating emotions in an effort to decrease the likelihood
that one would act on them. To act on pure emotions may produce instant gratification
but then have long-term consequences. DBT stresses the importance of self-care in
regulating emotions. In other words, neglecting self-care makes one vulnerable to giving
into their emotions.
According to DBT, there are six levels of self-care that help establish a strong
psychological foundation. The more areas that are off balance, the more likely that one
would be emotionally off balance. The six areas of self-care are introduced via PLEASE
MASTER. The components of PLEASE MASTER are:
- TREAT PHYSICAL ILLNESS
In other
words, take care of your body. This includes having annual checkups and also
seeing your doctor when necessary. If a doctor writes a prescription, the
medications should be taken as prescribed.
- BALANCED EATING
This means not eating too much or too
little. Specifically, excessive calories can decrease alertness and
concentration, which creates a sense of “fogginess” and makes concentration
difficult. Conversely, too little food can also make concentration difficult and
cause irritability.
- AVOID MOOD-ALTERING DRUGS
In other words, do not use
medications that are not prescribed to you, and minimize the use of alcohol. In
the long run, prolonged exposure to illegal drugs and alcohol can result in
physical ailments and decreased optimal functioning of organs. In the short run,
coming down off of excessive use of drug or alcohol makes moods more difficult
to manage. In addition, suddenly stopping addictive drugs can
result in withdrawal—negative
experiences that accompany reducing or stopping drug use, including physical
pain and other symptoms. Mood-altering drugs include caffeine, which is
found in a wide variety of products, including coffee, tea, soft drinks, candy,
and desserts. Although the U.S. Food and Drug Administration lists caffeine as a
safe food substance, it has at least some characteristics of dependence, and
sudden reduction of excessive caffeine can result in being irritable, restless,
and drowsy, as well as experiencing strong headaches.
- BALANCED SLEEP
Off-balanced sleep has similar negative
effects as unhealthy eating. Too much sleep can create more drowsiness and too
little causes difficulty focusing and irritability. According to a recent
poll, [2]
about one-fourth of American adults say they get a good night’s sleep only a few
nights a month or less. Getting enough sleep is a luxury that many of us seem to
be unable or unwilling to afford, and yet sleeping is one of the most important
things we can do for ourselves. Continued over time, a nightly deficit of even
only 1 or 2 hours can have a substantial impact on mood and performance.
- GET EXERCISE
The word “exercise” is more flexible than can
be imagined. Daily exercise is important for overall physical and emotional
well-being. However, exercise does not have to be going to the gym every day. It
could be something as simple as fast-paced housework, brisk walks, and/or
parking in a spot that’s farther away from a destination. In other words,
exercise can be some concentrated time during a given day, or it can be
incorporated throughout a given day.
- BUILD MASTERY
Try to do one thing a day to make yourself
feel competent, build your self-confidence, and give you a sense of being in
control. In the course of a day, many people spend more time doing things for
others or things that “need to” get done. To incorporate some time during the
day or week to things that have been mastered such as or writing, cooking, or
learning a new language can raise self-esteem and create a sense of being
satisfied.
So taking PLEASE MASTER into account, how can lack of self-care create emotional
imbalance? Let’s say you are taking 17 credits in your third semester at college. When
you registered, it seemed reasonable that taking extra credits during the Spring and
Fall semesters could result in early graduation. As the semester progresses, you seem to
be managing the stress of 17 credits well. You have made an outline of a study schedule
that fits perfectly with your part time job. Then, 3 weeks before the end of the
semester, you get the final exam schedule. It looks as though most of your exams fall on
the same day. The 3 weeks' notice that you have sets the stage for anxiety and
worry.
Now, let’s take this a step further. Some anxiety and worry is good for you because it
helps create focus and motivation. However, your anxiety causes you to lose sleep. Then
you develop a cold because lack of sleep can affect your immune system. Now, because you
are anxious, not sleeping well, and not feeling well, the anxiety is amplified to the
point that your stomach is in knots, so you have start skipping meals. You realize your
level of anxiety, so to calm down, you start drinking a little “just to take the edge
off.” However, the alcohol has hit a little harder than usual because you have not been
eating. So now, you are not feeling well, not sleeping well, not eating well, and are
suffering from a hangover. Finally, since your energy is drained from lack of sleep,
poor eating, and some alcohol use, you have not had the energy to go to the gym, which
gives you a sense of mastery.
This example is exaggerated to highlight that neglecting your needs can create emotional
imbalance. Emotional vulnerability, or being in emotional mind as per DBT, creates the
potential to give into the emotions. Again, giving into emotions can provide short-term,
instant gratification but can also have long-term consequences. In our example, the
anxiety resulted in unhealthy responses (neglecting self-care). Although not highlighted
in the example, an unhealthy response to anxiety would be to avoid what is making you
anxious. If, given all the stressors in this example, you stopped studying, you would
jeopardize you GPA and your plan to graduate early.
Think of your own examples of when your emotions were put off balance due to lack of
self-care. Most people have experienced being called “grumpy” when they have not had
enough sleep. In more extreme cases, drug and alcohol use can create vulnerability for
violence, an extreme behavioral response to anger.
References
- Linehan, M.
(1993).
Skills Training Manual for Treating Borderline Personality Disorder. Guilford Press. New York.
- National Sleep Foundation.
(2008).
Sleep in America poll. Retrieved from http://www.sleepfoundation.org/sites/default/files/2008%20POLL%20SOF.PDF.
Socialization begins as early as 6 months through infant actions such as smiling,
gesturing, and making sounds. In most case, socializing begins in a very balanced, give
and take manner between infants and adults. That is until the child starts preschool
and/or starts interacting with other children. By the time a child is about 18 months
old, a child begins to show preference for certain toys and preference for interacting
with certain peers.
Once peer interactions tend to increase as the child starts his academic career. At the
beginning of elementary school, well balanced peer interactions tend to be based on
gender and this slowly becomes more gender integrated as children grow into
adolescence.
It is also about early adolescence where social imbalance is most likely to occur. It is
at this time where peer popularity is introduced. This is where certain personality
characteristics become prominent in being socially balanced. In order to establish and
maintain relationships with like age peers, common personality traits include being
extraverted, cooperative, and supportive. [1] In
addition, socially well balanced peers tend to do well academically.
At the time of late childhood and into early adolescence, signs that a child is socially
imbalanced may emerge. Overall, socially imbalanced children and adolescents tend to be
opposite of those who are socially balanced. In addition, they tend to be more
aggressive, both verbally and physically.
The consequences of being socially imbalanced can have long lasting impact. Initially,
those children who feel socially imbalanced will start withdraw socially. This tends to
be a defense and a way to “psychologically hide” from others. In other words, in the
mind of a socially imbalanced child, it is better to be neglected than rejected.
Aggressive acts in children have been well studied in the past, especially for those
rejected peers. At the present time, this topic has had a resurgence with newly coined
terms such as “cyber-bullying.” As a result of technology, rejected peers are no longer
only subjected to aggressive acts in the school yard and neighborhood streets. Rejected
peers are potentially subjected to ridicule 24 hours per day, seven days per week. The
consequences of such forms of aggression can go without consequences, often leaving the
rejected peer feeling powerless and revictimized. In this modern day and age, aggressive
acts are subject to occur in the safety of one’s home, at any hour of the day, and at
any day of the week.
The short and long term consequences of feeling socially rejected included difficulty
initiating romantic relationships and also more dire consequences. Specifically, recent
research has indicated a type of cynical shyness with males. In cynical shyness, males
had a strong desire for social involvement but lacked social skills and, consequently,
were repeatedly rejected by peers. As rejection re-occurred, the unexpressed emotional
pain intensified which resulted in anger and hatred. Males with cynical shyness, and who
lacked coping skills and/or resilience, were found more likely to commit acts of
violence. [2]
learn by doing
The video below demonstrates the consequences of social phobia. Match up the experiences
of this individual with some of the DSM-IV-TR criteria of Social Phobia.
Summary
The experience of being out of balance can be subjective to the person. As an example,
characteristics of an imbalanced state may include different degrees of deficiency in
the areas sleep, nutrition, and affiliation with others. With external demands often
taking precedence over internal needs, a state of being out of balance can be both slow
and gradual. Without being conscious of the process, the consequences for being out of
balance may emerge. Although the consequences are many and, again, subjective to the
person, the next two modules discuss two such consequences: stress and physical
pain.
References
- Rabiner, D. L., Keane, S. P., and MacKinnon-Lewis,
C.
(1993).
"Children’s beliefs about familiar and unfamiliar peers in relation
to their sociometric status." Developmental Psychology. Volume 29.
Number 2. 236–243 Pages.
- American Psychological Association.
(2007).
Cynical shyness can precipitate violence in males, say researchers, and may be a factor in school shootings. Retrieved from http://www.apa.org/news/press/releases/2007/08/shyness.aspx.
Emotions matter because they influence our behavior and there is no emotional
experience that has a more powerful influence on us than stress. In 1936, Hans Selye stated that stress is “the nonspecific
response of the body to any demand for change." [1] Stress
also refers to the physiological responses that occur when
an organism fails to respond appropriately to emotional or physical
threats. However, the word has since manifested away from science and
into popular culture, losing the essence of the original definition. Overall,
stress occurs when there is a threat of resource loss. In general, people seek
to collect, build, and then protect resources. Resources can be anything such
as money, personal characteristics, self-esteem, and seniority. From a
physiological perspective, most people have similar reactions to stress
(although to varying degrees), however, stress is subjective in that what may
be stressful to one person may not be stressful to another.
Extreme negative events, such as being the victim of a terrorist attack, a
natural disaster, or a violent crime, may produce an extreme form of stress
known as posttraumatic stress disorder (PTSD). PTSD is a
medical syndrome that includes symptoms of anxiety, sleeplessness,
nightmares, and social withdrawal. It can occur when a person has been
exposed to a traumatic event where the person experienced, witnessed, or was
confronted with something that involved actual or threatened death or serious
injury, followed by intense fear, helplessness, and/or horror. PTSD is
frequently experienced by soldiers who return home from wars, with those who
have experienced subjectively more extreme events during war potentially
experiencing more severe PTSD.
When extreme or prolonged, stress can create substantial health problems. For instance,
survivors of hurricane Katrina had three times the rate of heart attacks than the national
average in the years following the disaster, and this is probably due to the stress that
the hurricane created. [2] In another example, people in New York
City who lived nearer to the site of the 9/11 terrorist attacks reported experiencing more
stress in the year following it than those who lived farther away. [3]
learn by doing
Watch this video about posttraumatic stress disorder (PTSD) and answer
the following questions.
Stress is not unique, however, to the experience of extremely traumatic events.
It can occur in our everyday lives, having a variety of both negative—and
positive—outcomes. Think about an event that you would describe as
“annoying.” It is not dangerous or life-threatening, yet you may find it to be
somewhat stressful.
Not all stress is to be avoided and not all stress can be avoided. Positive
events, such as going on a trip, planning a party, or learning a new skill,
also may result in a person experiencing stress. In some cases, stress even can
be helpful. For example, stress can “keep you on your toes” so that you respond
to a situation with an appropriate level of attention and arousal. Studying for
a test is an example where you want to pass so, a healthy stress level will
help focus you to study.
Stimuli or external events that cause a person to experience stress of any kind
are called stressors.
Stressors in Our Everyday Lives
The stress that you experience in your everyday life can also be taxing.
Thomas Holmes and Richard Rahe [4] developed a measure of
some everyday life events that might lead to stress. The following tables
show The Holmes and Rahe Stress Scale and its interpretation of the
score. The Holmes and Rahe Stress Scale was developed when 2,500 members
of the military were asked to complete the rating scale and then the
health records of the soldiers over the following 6 month were
reviewed. [5] The results were clear:
The higher the scale score, the more likely the soldier was to end up in
the hospital.
| The Holmes and Rahe Stress Scale |
|---|
| Life Event |
Score |
| Death of spouse |
100 |
| Divorce |
73 |
| Marital separation from mate |
65 |
| Detention in jail, other institution |
63 |
| Death of a close family member |
63 |
| Major personal injury or illness |
53 |
| Marriage |
50 |
| Fired from work |
47 |
| Marital reconciliation |
45 |
| Retirement |
45 |
| Major change in the health or behavior of a family member |
44 |
| Pregnancy |
40 |
| Sexual difficulties |
39 |
| Gaining a new family member (e.g., through birth, adoption,
oldster moving, etc.) |
39 |
| Major business readjustment (e.g., merger, reorganization,
bankruptcy) |
39 |
| Major change in financial status |
38 |
| Death of close friend |
37 |
| Change to different line of work |
36 |
| Major change in the number of arguments with spouse |
35 |
| Taking out a mortgage or loan for a major purchase |
31 |
| Foreclosure on a mortgage or loan |
30 |
| Major change in responsibilities at work |
29 |
| Son or daughter leaving home (e.g., marriage, attending
college) |
29 |
| Trouble with in-laws |
29 |
| Outstanding personal achievement |
28 |
| Spouse beginning or ceasing to work outside the home |
26 |
| Beginning or ceasing formal schooling |
26 |
| Major change in living conditions |
25 |
| Revision of personal habits (dress, manners, associations,
etc.) |
24 |
| Trouble with boss |
23 |
| Major change in working hours or conditions |
20 |
| Change in residence |
20 |
| Change to a new school |
20 |
| Major change in usual type and/or amount of recreation |
19 |
| Major change in church activities (a lot more or less than
usual) |
19 |
| Major change in social activities (clubs, dancing, movies,
visiting) |
18 |
| Taking out a mortgage or loan for a lesser purchase (e.g., for a
car, television , freezer, etc.) |
17 |
| Major change in sleeping habits |
16 |
| Major change in the number of family get-togethers |
15 |
| Major change in eating habits |
15 |
| Vacation |
13 |
| Christmas season |
12 |
| Minor violations of the law (e.g., traffic tickets, etc.) |
11 |
| Total |
______ |
|
| Interpretation of Holmes and Rahe Stress Scale |
|---|
| Number of Life-Change Units |
Chance of Developing a Stress-Related Illness (%) |
| Less than 150 |
30 |
| 150–299 |
50 |
| More than 300 |
80 |
|
Although some of the items on the Holmes and Rahe scale are more major,
you can see that even minor stressors add to the total score. Our everyday interactions with the environment that are
essentially negative, known as daily hassles, can also create
stress as well as poorer health
outcomes. [6]
Events that may seem rather trivial altogether, such as misplacing our
keys, having to reboot our computer because it has frozen, being late for
an assignment, or getting cut off by another car in rush-hour traffic,
can produce
stress. [7] [8]
found that medical students who were tested during, rather than several
weeks before, their school examination periods showed lower immune system
functioning. Other research has found that even more minor stressors,
such as having to do math problems during an experimental session, can
compromise the immune
system. [9]
learn by doing
As you just learned, the Holmes and Rahe study showed that the higher the
score from their stress scale, the more likely a person was to develop a
stress-related illness.
In 1998, Renner and Mackin [10] published a similar scale they had developed
with items that typical college-aged individuals would relate to better.
This scale is called the College Undergraduate Stress Scale (CUSS) and is
presented below. Renner and Mackin gave the CUSS to approximately 12,000
college students.
| Event |
Stress Ratings |
| Being raped |
100 |
| Finding out that you are HIV-positive |
100 |
| Being accused of rape |
98 |
| Death of a close friend |
97 |
| Death of a close family member |
96 |
| Contracting a sexually transmitted disease (other than AIDS) |
94 |
| Concerns about being pregnant |
91 |
| Finals week |
90 |
| Concerns about your partner being pregnant |
90 |
| Oversleeping for an exam |
89 |
| Flunking a class |
89 |
| Having a boyfriend or girlfriend cheat on you |
85 |
| Ending a steady dating relationship |
85 |
| Serious illness in a close friend or family member |
85 |
| Financial difficulties |
84 |
| Writing a major term paper |
83 |
| Being caught cheating on a test |
83 |
| Drunk driving |
82 |
| Sense of overload in school or work |
82 |
| Two exams in one day |
80 |
| Cheating on your boyfriend or girlfriend |
77 |
| Getting married |
76 |
| Negative consequences of drinking or drug use |
75 |
| Depression or crisis in your best friend |
73 |
| Difficulties with parents |
73 |
| Talking in front of a class |
72 |
| Lack of sleep |
69 |
| Change in housing situation (hassles, moves) |
69 |
| Competing or performing in public |
69 |
| Getting a physical fight |
66 |
| Difficulties with a roommate |
66 |
| Job changes (applying, new job, work, hassles) |
65 |
| Declaring a major or concerns about future plans |
65 |
| A class you hate |
62 |
| Drinking or use of drugs |
61 |
| Confrontations with professors |
60 |
| Starting a new semester |
58 |
| Going on a first date |
57 |
| Registration |
55 |
| Maintaining a steady dating relationship |
55 |
| Commuting to campus or work, or both |
54 |
| Peer pressures |
53 |
| Being away from home for the first time |
53 |
| Getting sick |
52 |
| Concerns about your appearance |
52 |
| Getting straight A’s |
51 |
| A difficult class that you love |
48 |
| Making new friend; getting along with friends |
47 |
| Fraternity or sorority rush |
47 |
| Falling asleep in class |
40 |
| Attending an athletic event (e.g., football game) |
20 |
Regardless of the type or the level of stress a person experiences, the body’s
physiological response to stressors is basically the same. We’ll explore this aspect of
stress in the next section.
References
- Selye, H.
(1956).
The Stress of Life. McGraw-Hill. New York.
- American Medical Association.
(2009).
Three-fold heart attack increase in Hurricane Katrina survivors. Retrieved from http://www.ama-assn.org/ama/pub/news/news/heart-attack-katrina-survivors.shtml.
- Pulcino, T., Galea, S., Ahern, J., Resnick,
H., Foley, M., and Vlahov, D.
(2003).
"Posttraumatic stress in women after the September 11 terrorist
attacks in New York City." Journal of Women’s Health. Volume 12. Number
8. 809–820 Pages.
- Holmes, T. H., and Rahe, R. H.
(1967).
"The social readjustment rating scale." Journal of Psychosomatic Research. Volume 11. Number 2. 213–218 Pages.
- Rahe, R. H., Mahan, J., Arthur, R. J., and
Gunderson, E. K. E.
(1970).
"The epidemiology of illness in naval environments: I. Illness
types, distribution, severities and relationships to life change."
Military Medicine. Volume 135. Number 6. 443–452 Pages.
- Hutchinson, J. G., and Williams, P. G.
(2007).
"Neuroticism, daily hassles, and depressive symptoms: An
examination of moderating and mediating effects." Personality and
Individual Differences. Volume 42. Number 7. 1367–1378 Pages.
- Fiksenbaum, L. M., Greenglass, E. R., and
Eaton, J.
(2006).
"Perceived social support, hassles, and coping among the elderly."
Journal of Applied Gerontology. Volume 25. Number 1. 7–30 Pages.
- Glaser, R.
(1985).
"Stress-related impairments in cellular immunity." Psychiatry Research. Volume 16. Number 3. 233–239 Pages.
- Cacioppo, J. T., Berntson, G. G., Malarkey, W. B., Kiecolt-Glaser, J. K., Sheridan, J. F., Poehlmann, K. M., et al.
(2006).
Annals of the New York Academy of Sciences:
Neuroimmunomodulation: Molecular Aspects, Integrative Systems, and
Clinical Advances, Vol. 840. Chapter Autonomic, neuroendocrine, and
immune responses to psychological stress: The reactivity hypothesis.
New York Academy of Sciences. New York. 664–673 Pages. S. M. McCann et
al. (Eds.).
- Renner, M. J., and Mackin, R. S.
(1998).
"A life stress instrument for classroom use." Teaching of Psychology. Volume 25. Number 1. 46–48 Pages.
A subjective, triggering event will result in physiological changes in the body. Common
body characteristics of stress include cold extremities, tension headaches, neck pain,
rapid heartbeat, shallow breath, and/or digestive issues. Some of the physiological
consequences of prolonged stress include high blood pressure and heart disease.
From a historical context, the physiologist Hans Selye (1907–1982) studied stress by
examining how rats responded to being exposed to stressors such as extreme cold,
infection, shock, or excessive exercise. [1] [2] [3]
Selye found that regardless of the source of the stress, the rats experienced the same
series of physiological changes as they suffered the prolonged stress. Selye created the
term general adaptation syndrome (GAS) to refer to the three distinct phases of physiological change that occur in
response to long-term stress: alarm, resistance, and exhaustion. The figure
below describes each phase and depicts the changes in stress resistance over the three
phases.
The HPA Axis
The experience of stress creates both an increase in general arousal in the
sympathetic division of the autonomic nervous system (ANS), as well as another,
even more complex, system of physiological changes through the HPA axis. The HPA axis is a physiological response to stress involving interactions
among the hypothalamus, the pituitary, and the adrenal glands. The HPA
response begins when the hypothalamus secretes hormones that direct the
pituitary gland to release the hormone ACTH. ACTH then directs the adrenal
glands to secrete more hormones, including epinephrine, norepinephrine, and cortisol, a stress hormone that
releases sugars into the blood, helping preparing the body to respond to
threat. [4]
The initial arousal that accompanies stress is normally quite adaptive because it
helps us respond to potentially dangerous events. The experience of prolonged
stress, however, has a direct negative influence on our physical health.
Specifically, while stress increases activity in the sympathetic division of the
autonomic nervous system (ANS), it also suppresses activity in the
parasympathetic division of the ANS. When stress is long-term, the HPA axis
remains active and the adrenals continue to produce cortisol. This increased
cortisol production exhausts the stress mechanism, potentially leading to
fatigue and depression.
References
- Selye, H.
(1936).
"A syndrome produced by diverse nocuous agents." Nature. Volume 138. Number 3479. 32 Pages.
- Selye, H.
(1974).
"Forty years of stress research: Principal remaining problems and
misconceptions." Canadian Medical Association Journal. Volume 115.
Number 1. 53–56 Pages.
- Selye, H.
(1982).
The nature of stress. Retrieved from http://www.icnr.com/articles/thenatureofstress.html.
- Rodrigues, S. M., LeDoux, J. E., and Sapolsky, R. M.
(2009).
"The influence of stress hormones on fear circuitry." Annual Review of Neuroscience. Volume 32. Number 1. 289–313 Pages.
Not all people experience and respond to stress in the same way, and these differences
can be important. The cardiologists Meyer Friedman and R. H. Rosenman [1] were
among the first to study the link between stress and heart disease. In their research
they noticed that even though the partners in married couples often had similar
lifestyles, diet, and exercise patterns, the husbands nevertheless generally had more
heart disease than did the wives. As they tried to explain the difference, they focused
on the personality characteristics of the partners, finding that the husbands were more
likely than the wives to respond to stressors with negative emotions and hostility.
Recent research has shown that the strongest predictor of a physiological stress response
from daily hassles is the amount of negative emotion that they evoke. People who
experience strong negative emotions as a result of everyday hassles, and who respond to
stress with hostility, experience more negative health outcomes than do those who react
in a less negative way. [2] [3]
Williams and his colleagues [4] found that people who scored high on
measures of anger were three times more likely to suffer from heart attacks in
comparison to those who scored lower on anger.
On average, men are more likely than are women to respond to stress by activating the
fight-or-flight response, which is an emotional and behavioral
reaction to stress that increases the readiness for action. The arousal that
men experience when they are stressed leads them to either go on the attack, in an
aggressive or revenging way, or else retreat as quickly as they can to safety from the
stressor. The fight-or-flight response allows men to control the source of the stress if
they think they can do so, or if that is not possible, it allows them to save face by
leaving the situation. The fight-or-flight response is triggered in men by the
activation of the HPA axis.
Women, on the other hand, are less likely to take a fight-or-flight response to stress.
Rather, they are more likely to take a tend-and-befriend
response. [5] The tend-and-befriend response is a behavioral reaction to stress that involves activities designed to
create social networks that provide protection from threats. This approach is
also self-protective because it allows the individual to talk to others about her
concerns, as well as to exchange resources, such as child care. The tend-and-befriend
response is triggered in women by the release of the hormone ocytocin, which promotes affiliation. Overall, the tend-and-befriend response
is healthier than the flight-or-flight response because it does not produce the elevated
levels of arousal related to the HPA, including the negative results that accompany
increased levels of cortisol. This may help explain why women, on average, have less
heart disease and live longer than men.
In her fascinating research, Shelly Taylor showed that women and men have very different
ways of dealing with stress. Women are more likely to move toward interaction while men
are more likely to move toward action and inaction.
References
- Friedman, M., and Rosenman, R. H.
(1974).
Type A Behavior and Your Heart. Knopf. New York.
- McIntyre, K., Korn, J., and Matsuo, H.
(2008).
"Sweating the small stuff: How different types of hassles result in
the experience of stress." Stress and Health: Journal of the
International Society for the Investigation of Stress. Volume 24. Number
5. 383–392 Pages.
- Suls, J., and Bunde, J.
(2005).
"Anger, anxiety, and depression as risk factors for cardiovascular
disease: The problems and implications of overlapping affective
dispositions." Psychological Bulletin. Volume 131. Number 2. 260–300
Pages.
- Williams, R. B.
(2006).
Handbook of Health Psychology. Chapter
Hostility: Effects on health and the potential for successful behavioral
approaches to prevention and treatment. Lawrence Erlbaum Associates.
Mahwah, NJ. 661–668 Pages. A. Baum, T. A. Revenson, and J. E. Singer
(Eds.).
- Taylor, S. E., Klein, L. C., Lewis, B. P.,
Gruenewald, T. L., Gurung, R. A. R., and Updegraff, J. A.
(2000).
"Biobehavioral responses to stress in females: Tend-and-befriend,
not fight-or-flight." Psychological Review. Volume 107. Number 3.
411–429 Pages.
No matter how healthy and happy we are in our everyday lives, there are going to be times
when we experience stress. But we do not need to throw up our hands in despair when
things go wrong; rather, we can use our personal and social resources to help us.
Perhaps the most common approach to dealing with negative affect is to attempt to
suppress, avoid, or deny it. You probably know people who seem to be stressed,
depressed, or anxious, but they cannot or will not see it in themselves. Perhaps you
tried to talk to them about it, to get them to open up to you, but were rebuffed. They
seem to act as if there is no problem at all, simply moving on with life without
admitting or even trying to deal with the negative feelings. Or, perhaps you have even
taken a similar approach yourself. Have you ever had an important test to study for or
an important job interview coming up, and rather than planning and preparing for it, you
simply tried put it out of your mind entirely?
Research has found that ignoring stress and suppressing negative emotions can be an
unhealthy coping resources. For one, ignoring our problems does not make them go away.
If we experience so much stress that we get sick, we now have to manage both physical
illness and the ignored stressors. [1] For example, if we
know that we have that big exam coming up, we have to focus on the exam, despite the
initial urge to ignore it. To suppress or deny the fact that exam is coming up takes
emotional and physical effort, and we can become physically and emotionally tired
Despite ignoring stress and suppressing emotions not being healthy in the long run, there
are times when this might work out in the short run. Specifically, suppressing
emotionally based stress can be appropriate when a situation is uncontrollable or when
nothing can be done about the situation at the moment. For example, a person is wide
awake at 3:00 a.m. because he is worried about his day he has. He mentally reviews all
the events he has to do that include: making a doctor appointment, getting his oil
changed, and wondering if his study group will show up in the library. At this moment,
it would be appropriate to suppress the emotions and ignore the stress as there is
nothing he can do about any of the stressors at 3:00 a.m. To stay awake about things
that he cannot control will actually make him less effective for the busy day he has
later that morning.
Having said that, prolonged suppression of stress, especially when the stressors are
controllable, can result in decreased energy and this creates vulnerability for negative
emotions re emerging into consciousness. Consequently, a re-experience of the avoided
negative affect returns, and likely with much more intensity. For instance, to avoid
studying for a test will make testing day more stressful. To avoid the stress of waiting
for an oil change will create more stress in the long run as the car drives another mile
with old oil.
Although there are pharmacological interventions to help manage stress,
nonpharmacological interventions include increasing self-awareness of body cues of
stress, environmental control of the stressor such as changing jobs, and/or changing
thoughts about the stressor.
Daniel Wegner and his colleagues [2] directly tested whether
people would be able to effectively suppress a simple thought. He asked them to not think about a white bear for 5 minutes but to ring a bell if
they did. (Try it yourself. Can you do it?) However, participants were unable to
suppress the thought as instructed. The white bear kept popping into mind, even when the
participants were instructed to avoid thinking about it. You might have had this
experience when you were dieting or trying to study rather than party; the chocolate bar
in the kitchen cabinet and the fun time you were missing at the party kept popping into
mind, disrupting your work.
Suppressing our negative thoughts does not work and, as a matter of fact, the evidence
supports the opposite: When we are faced with troubles, it is healthy to let out the
negative thoughts and feelings by expressing them either to ourselves or to others.
James Pennebaker and his colleagues [3] [4]
have conducted many correlational and experimental studies that demonstrate the
advantages to our mental and physical health of opening up versus suppressing our
feelings. This research team has found that simply talking about or writing about our
emotions or our reactions to negative events provides substantial health benefits. For
instance, Pennebaker and Beall [5]
randomly assigned students to write about either the most traumatic and stressful event
of their lives or trivial topics. Although the students who wrote about the traumas had
higher blood pressure and more negative moods immediately after they wrote their essays,
they were also less likely to visit the student health center for illnesses during the
following six months. Other research studied individuals whose spouses had died in the
previous year, finding that the more they talked about the death with others, the less
likely they were to become ill during the subsequent year. Daily writing about one’s
emotional states has also been found to increase immune system functioning. [6]
Opening up probably helps in various ways. For one, expressing our problems to others
allows us to gain information, and possibly support, from them (remember the tend-and-befriend response that is so effectively used to reduce
stress by women). Writing or thinking about one’s experiences also seems to help people
make sense of these events and may give them a feeling of control over their lives. [7]
It is easier to respond to stress if we can interpret it in more positive ways. Kelsey
and colleagues [8] found that some people
interpret stress as a challenge (something that they feel that they can, with effort,
deal with), whereas others see the same stress as a threat (something that is negative
and fearful). People who viewed stress as a challenge had fewer physiological stress
responses than those who viewed it as a threat—they were able to frame and react to
stress in more positive ways.
When an external stressor is unavoidable, changing thoughts about the stressor can help
minimize the intensity. It also helps to gain coping resources in order to learn
tolerance of the stressor. For instance, a person starting her law career right out of
college may fully commit to her assigned tasks. However, 50-hour weeks and bringing home
files on the weekend begin to wear on her. She starts to worry that she is not doing an
adequate job and her sleep starts to suffer. However, at some point, she starts to
change her perception of the job. She starts to think, “If my boss has not said
anything, there is a good chance I’m doing a good job.” She also starts to see her
50-hour work weeks and weekend work as expedited ways to gain more experience. She
calculates her hours and thinks that she can condense five years of experience into
three. She starts to see her new job as an opportunity to gain a lot of experience in a
short amount of time. As her thoughts about the stressors change, she starts to feel
very excited about her opportunity, and the intensity of her stress is thereby
minimized.
References
- Gross, J. J., and Levenson, R. W.
(1997).
"Hiding feelings: The acute effects of inhibiting negative and
positive emotion." Journal of Abnormal Psychology. Volume 106. Number 1.
95–103 Pages.
- Wegner, D. M., Schneider, D. J., Carter, S.
R., and White, T. L.
(1987).
"Paradoxical effects of thought suppression." Journal of
Personality and Social Psychology. Volume 53. Number 1. 5–13 Pages.
- Pennebaker, J. W., Colder, M., and Sharp, L. K.
(1990).
"Accelerating the coping process." Journal of Personality and Social Psychology. Volume 58. Number 3. 528–537 Pages.
- Watson, D., and Pennebaker, J. W.
(1989).
"Health complaints, stress, and distress: Exploring the central
role of negative affectivity." Psychological Review. Volume 96. Number
2. 234–254 Pages.
- Pennebaker, J. W., and Beall, S. K.
(1986).
"Confronting a traumatic event: Toward an understanding of
inhibition and disease." Journal of Abnormal Psychology. Volume 95.
Number 3. 274–281 Pages.
- Petrie, K. J., Fontanilla, I., Thomas, M.
G., Booth, R. J., and Pennebaker, J. W.
(2004).
"Effect of written emotional expression on immune function in
patients with human immunodeficiency virus infection: A randomized
trial." Psychosomatic Medicine. Volume 66. Number 2. 272–275 Pages.
- Pennebaker, J. W., and Stone, L. D. (Eds.).
(2004).
Translating Traumatic Experiences into Language: Implications for Child Abuse and Long-Term Health. American Psychological Association. Washington, DC.
- Kelsey, R. M., Blascovich, J., Tomaka, J.,
Leitten, C. L., Schneider, T. R., and Wiens, S.
(1999).
"Cardiovascular reactivity and adaptation to recurrent
psychological stress: Effects of prior task exposure." Psychophysiology.
Volume 36. Number 6. 818–831 Pages.
There is also a “window of stress” in that too little stress can result in
inactivity while too much stress can have physical and emotional consequences.
However, just the right amount of stress can be adaptive and very motivating.
Stress, when in certain parameters, can be motivating and help with focus. For
example, a person is called for a job interview right after graduating with a
degree in accounting. If this person has already received an offer from another
company, there is likelihood that the intensity of stress will not be that
high. As such, that person may not bring his suit to the cleaners. He might run
five minutes late for the interview and forget to bring a copy of his resume.
If another person was called for the same job, but this has been his only call
thus far, the stress level will be higher. In this case, the person will
prepare by reviewing answers to different questions, make sure his suit is
pressed, and he will bring several copies of resume. If a third person was
called for the same interview, but was already passed over for different
positions in other companies, his stress may get to a point where it actually
works against him. He may very well do the things he is “supposed to do” in an
interview, but he also may magnify his stress level by being self conscious
about what he says. He may be so focused on what he wants to say, that he is
not listening to what the interviewer is saying. As such, he will not get the
job. Reflect on your own adaptive stress in the following
exercise.
Emotional responses such as the stress reaction are useful in warning us about potential
danger and in mobilizing our response to it, so it is a good thing that we have them.
However, we also need to learn how to control our emotions, to prevent them from letting
our behavior get out of control. The ability to successfully control
our emotions is known as emotion regulation.
Emotion regulation has some important positive outcomes. Consider, for
instance, research by Walter Mischel and his colleagues. In their studies, they
had 4- and 5-year-old children sit at a table in front of a yummy snack, such
as a chocolate chip cookie or a marshmallow. The children were told that they
could eat the snack right away if they wanted. However, they were also told
that if they could wait for just a couple of minutes, they’d be able to have
two snacks—both the one in front of them and another just like it. However, if
they ate the one that was in front of them before the time was up, they would
not get a second.
Mischel found that some children were able to override the impulse to seek
immediate gratification to obtain a greater reward at a later time. Other
children, of course, were not; they just ate the first snack right away.
Furthermore, the inability to delay gratification seemed to occur in a
spontaneous and emotional manner, without much thought. The children who could
not resist simply grabbed the cookie because it looked so yummy, without being
able to stop themselves. [1] [2]
The ability to regulate our emotions has important consequences later in life.
When Mischel followed up on the children in his original study, he found that
those who had been able to self-regulate grew up to have some highly positive
characteristics: They got better SAT scores, were rated by their friends as
more socially adept, and were found to cope with frustration and stress better
than those children who could not resist the tempting cookie at a young age.
Thus effective self-regulation can be recognized as an important key to success
in life. [3] [4] [5]
Watch this video to see how Stickman applies some self-regulatory techniques
when he’s angry.
This video was designed to help children learn about the basics of
healthy self-regulation.
Emotion regulation is influenced by body chemicals, particularly the
neurotransmitter serotonin. Preferences for small,
immediate rewards over large, but later, rewards have been linked to low levels
of serotonin in animals, [6] [7] and low levels of serotonin are tied
to violence and impulsiveness in human suicides. [8]
References
- Metcalfe, J., and Mischel, W.
(1999).
"A hot/cool-system analysis of delay of gratification: Dynamics of
willpower." Psychological Review. Volume 106. Number 1. 3–19 Pages.
- Strack, F., and Deutsch, R.
(2007).
Social Psychology: Handbook of Basic Principles, Vol. 2.
Chapter The role of impulse in social behavior. Guilford Press. New
York. 408–431 Pages. A. W. Kruglanski and E. T. Higgins (Eds.).
- Ayduk, O., Mendoza-Denton, R., Mischel, W.,
Downey, G., Peake, P. K., and Rodriguez, M.
(2000).
"Regulating the interpersonal self: Strategic self-regulation for
coping with rejection sensitivity." Journal of Personality and Social
Psychology. Volume 79. Number 5. 776–792 Pages.
- Eigsti, I.-M., Zayas, V., Mischel, W., Shoda, Y.,
Ayduk, O., Dadlani, M. B., et al.
(2006).
"Predicting cognitive control from preschool to late adolescence
and young adulthood." Psychological Science. Volume 17. Number 6.
478–484 Pages.
- Mischel, W., and Ayduk, O. (Eds.)
(2004).
Willpower in a Cognitive-Affective Processing System: The Dynamics of Delay of Gratification. Guilford Press. New York.
- Bizot, J.-C., Le Bihan, C., Peuch, A. J., Hamon, M., and Thiebot, M.-H.
(1999).
"Serotonin and tolerance to delay of reward in rats." Psychopharmacology. Volume 146. Number 4. 400–412 Pages.
- Liu, Y. P., Wilkinson, L. S., and Robbins, T. W.
(2004).
"Effects of acute and chronic buspirone on impulsive choice and
efflux of 5-HT and dopamine in hippocampus, nucleus accumbens and
prefrontal cortex." Psychopharmacology. Volume 173. Number 1–2. 175–185
Pages.
- Asberg, M., Traskman, L., and Thoren, P.
(1976).
"5-HIAA in the cerebrospinal fluid: A biochemical suicide
predictor?." Archives of General Psychiatry. Volume 33. Number 10.
1193–1197 Pages.
We do not enjoy it, but the experience of pain is how the body informs us that we are in
danger. The burn when we touch a hot radiator and the sharp stab when we step on a nail
leads us to change our behavior, preventing further damage to our bodies. People who
cannot experience pain are in serious danger of damage from wounds that others with pain
would quickly notice and attend to.
The experience of pain is a combination of body responses and subjective
experience. In other words, the level of pain can be positively or negatively impacted
by the amount of attention, level of motivation, and belief about the pain. This is
also referred to as psychogenic pain because, although there is a physical explanation for
it, pain can also be worsened by emotional states such as fear, depression, stress, or
anxiety. The above diagram will help bring some insight into the combination of
physiological and psychological aspects of pain. [1]
References
- WebMD.
(2012).
Pain types and classifications. Retrieved from http://www.webmd.com/pain-management/guide/pain-types-and-classifications.
The gate control theory of pain proposes that pain is determined by the
operation of two types of nerve fibers in the spinal cord. One set of smaller
nerve fibers carries pain from the body to the brain, whereas a second set of
larger fibers is designed to stop or start (as a gate would) the flow of
pain. [1] It is for this reason that
massaging an area where you feel pain may help alleviate it—the massage
activates the large nerve fibers that block the pain signals of the small nerve
fibers. [2]
Types of Pain
Since there are multiple causes of pain, there are also multiple types of
pain and multiple ways that people respond to it. Despite the discomfort
of pain, it is the way in which the body sends messages to the brain.
- Acute Pain and Chronic Pain
One of the many ways to classify pain
is to note it as either an acute or chronic type. The former, acute
pain, likely has a sudden onset and is of relatively short
duration. Acute pain has multiple sources but is usually the result
of tissue damage to the bones, muscles, and/or organs. Chronic
pain, on the other hand, is defined as pain lasting over three
months and medical interventions may have limited success. Chronic
pain can be the result of medical conditions such as osteoarthritis
or be the medical condition, such as in
fibromyalgia. While acute pain is usually associated with tissue
damage, chronic type is usually the result of nerve damage.
Sometimes, there is no clear origin for chronic pain, which can be
a source of frustration when it negatively impacts upon the quality
of life.
learn by doing
Watch the following video describing the physiology of pain and
answer the questions that follow.
- Breakthrough Pain
Associated more with chronic pain, especially if
the person is prescribed pain medication, is breakthrough pain.
Breakthrough pain is, in a sense, chronic pain that will
“breakthrough” the effects of pain medication. Breakthrough pain
can be experienced suddenly, as the result of seemingly
insignificant moving, or as the effects of pain medication begin to
wear off.
- Nociceptive and Neuropathic
In addition to acute and chronic pain,
there are many other ways that pain can be described. For instance,
pain can be classified as being either nociceptive or neuropathic.
The nociceptive type is caused by tissue damage while the
neuropathic type is caused by nerve damage. [3] [4]
- Miscellaneous Pain
Pain can also be classified by location (muscular pain,
joint pain, chest pain, back pain). It can also be described as an ache, a
sharp or stabbing, or throbbing. Finally, there are also pain syndromes that
include myofascial type pain syndromes such as Fibromyalgia where the pain is
located in certain muscles of the body. Overall, pain can be difficult to
describe because it is a very personal experience. As such, certain measures
have been developed to help describe and quantify pain level as it pertains to
a person. [3] [4]
| Pain Measure |
Description |
| Survey of Pain Attitudes (SOPA) |
Measures the belief about chronic pain so to measure how a person
may adjust to having pain. More specifically, it measures perceived
level of control over the pain, perceived level of disability, and
the belief that there is a cure for the pain. |
| Chronic Pain Coping Inventory (CPCI) |
Assesses use of coping in response to chronic pain in the past
week. Examples of coping include: restricting movement, resting,
need for assistance, exercise, task persistence. |
| Pain Beliefs and Perceptions Inventory (PBAPI) |
Similar to the SOPA in that it measures beliefs about pain and
belief about level of control over the pain. |
| Spouse Response Inventory (SRI) |
Assesses the spouses of those who experience pain. It measures a
spouse’s responses to pain and wellness behaviors from the partner
with pain issues. |
References
- Melzack, R., and Wall, P.
(1996).
The Challenge of Pain. Penguin. London.
- Wall, P.
(2000).
Pain: The Science of Suffering. Columbia University Press. New York.
- WebMD.
(2012).
Pain types and classifications. Retrieved from http://www.webmd.com/pain-management/guide/pain-types-and-classifications.
- National Institutes of Health, MedlinePlus.
(2012).
Chronic pain: Symptoms, diagnosis, and treatment. Retrieved from http://www.nlm.nih.gov/medlineplus/magazine/issues/spring11/articles/spring11pg5-6.html.
Experiencing pain is a lot more complicated than simply responding to neural messages. It
is also a matter of perception. We feel pain less when we are busy focusing on a
challenging activity, [1]
which can help explain why sports players may feel their injuries only after the game.
We also feel less pain when we are distracted by
humor. [2] And pain is soothed by
the brain’s release of endorphins, natural hormonal pain killers. The release of
endorphins can explain the euphoria experienced in the running of a
marathon. [3]
Mood Disorders
Much like pain level, the level of depression observed in people with mood
disorders varies widely. For some, a relationship exists between physical pain
and depression, however, it is difficult to determine if physical pain magnifies
depression or if depression magnifies physical pain. A phenomena known as the
“pain-prone” individual exists in that the physical pain one experiences is a
form of unexpressed or unacknowledged
depression. [4] The
pain-prone individual is more likely to be female, as major depressive disorder
occurs about twice as often in women as it does in
men. [5] [6]
As you will see in the next unit on psychological disorders, symptoms of
depression can include an all-encompassing low mood accompanied by low
self-esteem and by loss of interest or pleasure in normally enjoyable
activities. Furthermore, those negative feelings profoundly limit the
individual’s day-to-day functioning and ability to maintain and develop
interests in life. [7]
Somatoform Disorders
Somatoform disorders both occur in cases where psychological disorders are
related to the experience or expression of physical symptoms.
One case in which psychological problems create real physical impairments is in
the somatoform disorder known as somatization disorder (also called Briquet’s
syndrome or Brissaud-Marie syndrome). Somatization disorder is a psychological
disorder in which a person experiences numerous long-lasting but seemingly
unrelated physical ailments that have no identifiable physical cause. A person
with somatization disorder might complain of joint aches, vomiting, nausea,
muscle weakness, as well as sexual dysfunction. The symptoms that result from a
somatoform disorder are real and cause distress to the individual, but they are
due entirely to psychological factors. The somatoform disorder is more likely to
occur when the person is under stress, and it may disappear naturally over time.
Somatoform disorder is more common in women than in men, and usually first
appears in adolescents or those in their early 20s.
Another type of somatoform disorder is conversion disorder, which is a
psychological disorder where patients experience specific neurological symptoms
such as numbness, blindness, or paralysis, but where no neurological explanation
exists. [8] The difference between conversion and
somatoform disorders is in terms of the location of the physical complaint. In
somatoform disorder the malaise is general, whereas in conversion disorder there
are one or several specific neurological symptoms.
Conversion disorder gets its name from the idea that the existing psychological
disorder is “converted” into the physical symptoms. It was the observation of
conversion disorder (then known as “hysteria”) that first led Sigmund Freud to
become interested in the psychological aspects of illness in his work with
Jean-Martin Charcot. Conversion disorder is not common (a prevalence of less
than 1%), but it may in many cases be undiagnosed. Conversion disorder occurs
twice or more frequently in women than in men.
Hypochondriasis (hypochondria) is a psychological disorder accompanied by
excessive worry about having a serious illness. The patient often misinterprets
normal body symptoms such as coughing, perspiring, headaches, or a rapid
heartbeat as signs of serious illness, and the patient’s concerns remain even
after he or she has been medically evaluated and assured that the health
concerns are unfounded. Many people with hypochondriasis focus on a particular
symptom such as stomach problems or heart palpitations.
Somatoform disorders are problematic not only for the patient, but they also have
societal costs. People with these disorders frequently follow through with
potentially dangerous medical tests and are at risk for drug addiction from the
drugs they are given and for injury from the complications of the operations
they submit
to. [9] [10]
In addition, people with these disorders may take up hospital space that is
needed for people who are really ill. To help combat these costs, emergency
department and hospital workers use a variety of tests for detecting these
disorders.
Nonacceptance
According to Marsha Linehan, in her treatment model of dialectical behavior
therapy (DBT), both physical and emotional pain is to be accepted as an aspect
of life that all will endure. Nonacceptance is essentially combating the reality
of pain being a presence in life. Marsha Linehan states that the combination of
pain and the nonacceptance of the pain results in suffering. Suffering occurs
when a person resists the present reality and focuses on where he once was
and/or where he wishes he could be. [11]
Maladaptive Thoughts
In an earlier Wellness module, you were introduced to the role that maladaptive
thoughts play in psychological issues and to cognitive-behavioral
therapy (CBT). In a future unit, a more general explanation of CBT will be
given.
In relationship to this module, it is should be noted that the experience of pain
and be amplified by maladaptive thoughts. For instance, one can experience any
type of pain as listed in the physiological side of the Venn diagram. However,
if one has thoughts such as “I’ll never feel better,” or ignores the advice of
medical doctors and says, “I can work through the pain,” that person can
potentially make pain worse.
Despite the two examples of thoughts being seemingly opposite, a common theme
emerges in that both thoughts are not facts. The role of automatic thoughts in
CBT is instrumental. Automatic thoughts are just that—automatic. It can be
equated to the doctor tapping a knee that results in the person kicking. To
certain extent, one does not “think about thinking” as it can be reflexive.
However, a person can gain control over how he or she responds to automatic
thoughts.
One example of a maladaptive thought can exacerbate the physiological aspects of
pain is called a mental filter. A mental filter is when one focuses exclusively
on certain, usually negative or upsetting, aspects of something. So, let’s say
someone was experiencing a headache and has an automatic thought such as, “I
can’t believe I have another headache.” That type of thought can establish a
“filter” that only allows similar thoughts that may include: “I always get these
headaches,” “I’m going to have headaches for the rest of my life,” “These
headaches are making me miserable,” “No one else gets as many headaches as me.”
Although the initial, automatic thought is a fact, the mental filter usually
will invite thoughts that are untrue and, left unchallenged or unquestioned,
will be treated as fact. This, in turn, will amplify pain.
References
- Bantick, S. J., Wise, R. G., Ploghaus, A., Clare,
S., Smith, S. M., and Tracey, I.
(2002).
"Imaging how attention modulates pain in humans using functional
MRI." Brain: A Journal of Neurology. Volume 125. Number 2. 310–319
Pages.
- Zweyer, K., Velker, B., and Ruch, W.
(2004).
"Do cheerfulness, exhilaration, and humor production moderate pain
tolerance? A FACS study." Humor: International Journal of Humor
Research. Volume 17. Number 1–2. 85–119 Pages.
- Sternberg, W. F., Bailin, D., Grant, M.,
and Gracely, R. H.
(1998).
"Competition alters the perception of noxious stimuli in male and
female athletes." Pain. Volume 76. Number 1–2. 231–238 Pages.
- Blumer, D., and Heilbronn, M.
(1982).
"Chronic pain as a variant of depressive disease: the pain-prone
disorder." Journal of Nervous and Mental Disease. Volume 170. Number 7.
381-406 Pages.
- Kessler, R. C., Chiu, W. T., Demler, O.,
and Walters, E. E.
(2005).
"Prevalence, severity, and comorbidity of 12-month DSM-IV disorders
in the National Comorbidity Survey Replication." Archives of General
Psychiatry. Volume 62. Number 6. 617–627 Pages.
- Kessler, R. C., Berglund, P., Demler, O,
Jin, R., Koretz, D., Merikangas, K. R., et al.
(2003).
"The epidemiology of major depressive disorder: Results from the
National Comorbidity Survey Replication (NCS-R)." Journal of the
American Medical Association. Volume 289. Number 23. 3095–3105 Pages.
- Fairchild, K., and Scogin, F.
(2008).
Handbook of Emotional Disorders in Later Life: Assessment and Treatment. Chapter Assessment and treatment of depression. Oxford University Press. New York. K. Laidlow and B. Knight (Eds.).
- Akagi, H., and House, A. O.
(2001).
Hysterical Conversion: Clinical and Theoretical Perspectives.
Chapter The epidemiology of hysterical conversion. Oxford University
Press. Oxford, England. 73–87 Pages. P. Halligan, C. Bass, and J.
Marshall (Eds.).
- Bass, C., Peveler, R., and House, A.
(2001).
"Somatoform disorders: Severe psychiatric illnesses neglected by
psychiatrists." British Journal of Psychiatry. Volume 179. Number 1.
11–14 Pages.
- Looper, K. J., and Kirmayer, L. J.
(2002).
"Behavioral medicine approaches to somatoform disorders." Journal
of Consulting and Clinical Psychology. Volume 70. Number 3. 810–827
Pages.
- Linehan, M.
(1993).
Skills Training Manual for Treating Borderline Personality Disorder. Guilford Press. New York.
Narcotic Analgesics
Narcotic analgesics include opium, morphine, and heroin and are examples
of pain reducers that work on the physiological experience of pain. Such
narcotic analgesics are ingested and then connect to certain brain
receptors. Certain narcotic analgesics mimic the internal agents (such as
endorphins) that work on the central nervous system (brain and spinal
cord) and work toward decreasing pain.
Hypnotic Relief of Pain
Hypnotic relief of pain is employing the use of guided relaxation and
intense concentration. The goal is to have the attention of the subject
entirely focused on an image so that all external stimuli and potential
distractors are completely ignored. In other words, the goal is to have
the subject in a trance state. Hypnotherapy is a specialized area that
requires license, and is typically used as an adjunct to mental health
treatment. The use of hypnosis for pain is usually accomplished at pain
management centers. [1] [4]
A technique of a hypnotherapist is assisting a subject in visualizing
vivid, images in which the subject, for example, pictures himself
accomplishing goals. When the session is over, either the subject brings
himself out of hypnosis or the hypnotherapist helps end the trance-like
state. It is also possible to practice self-hypnosis and employ the skill
when necessary. Watch the video below which explains a specific, hypnotic
pain management technique:
Placebo Effect
A phenomenon is a general result that has been observed reliably in
systematic empirical research. In essence, it is an established answer to
a research question. Examples of phenomena include: the positive impact
that expressive writing improves health, women do not talk more than men,
and cell phone usage impairs driving ability. Some others are that
certain psychological disorders increased greatly in prevalence during
the late 20th century, people perform better on easy tasks when they are
being watched by others (and worse on difficult tasks), and people recall
items presented at the beginning and end of a list better than items
presented in the middle.
Phenomena are often given names by their discoverers or other
researchers, and these names can catch on and become widely known. Placebo effect is an example of a phenomenon.
Placebos, or fake psychological or medical treatments, often lead to
improvements in people’s symptoms and functioning.
As cited in a paper by Albert, [2] the American Medical
Association defines placebo as “a substance provided to a patient that
the physician believes has no specific pharmacological effect upon the
condition being treated.” Examples of a placebo include “a sham
treatment, injection, pill, procedure.”
Acceptance
As noted above, and according to Marsha Linehan in her treatment
model of dialectical behavioral therapy, both physical and emotional pain is to be accepted as
an aspect of life that all will endure. According to Linehan, the
acceptance of pain is to be free of suffering. Acceptance is the
ability to tolerate the moment that is being experienced. It should
be noted that true acceptance does not mean that it is OK to be in
pain. Rather, it means that the pain is being non judgmentally
acknowledged for what it is, as opposed to what one wants it to
be. [3]
Dialectical Behavioral Therapy (DBT)
As previously noted, dialectical behavioral therapy (DBT)
incorporates mindfulness as its’ foundation. DBT has been
well-researched in treating other issues than it was originally
developed for. One such issue that has been found to be highly
effective is the treatment of pain. Since DBT is primarily a coping
skills treatment, certain coping skills can help manage pain. The
skills or modules of DBT are core mindfulness, emotion regulation,
distress tolerance, and interpersonal effectiveness. Let’s look at
some examples of DBT skills that can help, at the very least,
minimize the intensity of pain. [3]
Acupuncture
learn by doing
The following video explains the basics of acupuncture and
its impact on pain management. After you have watched the
video, complete the following activity. The correct answers
will provide a summary about acupuncture.
Self-management
In self-management of pain treatment there is collaboration between
the person and the professionals that he or she interacts with.
This, in turn, provides a sense of control for the person in that
he or she is participating in intervention options, the pace of
treatment, and decision-making. Overall, it has been shown that
those who have participated in self management programs have
significantly increased their ability to manage the physiological
discomfort of pain. [5]
Other Types of Pain Treatments
In addition to the above treatments for chronic pain, certain
medications, electrical stimulation, nerve blocks, or surgery are
also interventions. Other forms, and preferably first line
interventions might include less invasive forms of pain management
such as psychotherapy, relaxation therapies, biofeedback, and
behavior modification. Much like acupuncture, pain may also be
minimized with the use of alternative treatments such as tai chi,
meditation, and/or massage therapies. [5]
| Pain Intervention |
Description |
| Electrical stimulation |
Transcutaneous electrical nerve stimulation (TENS) was
developed in the 1960s. It involves placing small electrodes
over the part of the body that is in pain. The electrodes are
attached to a machine that sends electricity to the pain
area. The electricity interrupts messages about the pain from
the nerves to the brain. |
| Nerve blocks |
Injections in the pain area contain a local anesthetic for
acute pain. If it is effective, then more permanent forms of
treatment can be employed. |
| Biofeedback |
Through biofeedback, one can learn relaxation techniques and
learn how to calm contracted muscles that can be a source of
pain. |
| Behavior modification |
Through a behavior modification program, evaluation of pain
behaviors are noted such as use of pain medications, overall
activity levels, and tolerance during specific exercises.
Once this baseline is established, pain behaviors and use of
pain medications are discouraged while levels of increased
activity level and well behaviors are reinforced. |
| Medications |
Pain medications may be
over-the-counter medications (such as Tylenol, aspirin, Cortizone,
Ben-Gay) or prescription pain relievers (such as Percocet,
Oxycodone, and antiseizure medications). Both prescribed and
nonprescribed pain relievers vary in their degree of
effectiveness, side effects, and level of addiction. |
| Psychotherapy |
As noted throughout the module, certain schools of therapy
(CBT, DBT) can help individuals cope with pain and/or change the way
he or she thinks about the pain. |
| Massage therapies |
Massage therapy can help relax muscle tissue. Relaxing muscle tissue may result in decreased nerve
compression and increased joint space; thus, reduced pain and
increased range of motion can result. |
| Tai chi |
The movements of tai chi have been described as both gentle
and graceful. Tai chi has been used as an intervention for
elderly people to relieve arthritis pain. Tai chi has been
called "moving meditation," due to its relaxing nature that
focuses on breathing and inner peace. In other words,
quieting the mind and relaxing the body while focusing on
breathing and tai chi moves creates less focus on pain. |
| Meditation |
Shamatha is a type of mediation that creates focused
attention on either breath or a mantra. Shamatha teaches
observation what's going on in the mind and body without
judgment. Research has shown that Shamatha creates changes in
how the somatosensory cortex of the brain responded to
pain. |
References
- WebMD.
(2012).
Mental health and hypnosis. Retrieved from http://www.webmd.com/anxiety-panic/guide/mental-health-hypnotherapy.
- Albert, E.
(2012).
Placebo: Don't Knock It Until You Try It:
Resolving The Bioethical Quadfecta While Recognizing The Placebo As a
Viable Option for Patients. Retrieved from http://www.slideshare.net/ea6603/bioethics-paper-on-placebos-power.
- Linehan, M.
(1993).
Skills Training Manual for Treating Borderline Personality Disorder. Guilford Press. New York.
- Mayo Clinic staff.
(2009).
Hypnosis. Retrieved from http://www.mayoclinic.com/health/hypnosis/MY01020/METHOD=print.
- National Institutes of Health, MedlinePlus.
(2012).
Chronic pain: Symptoms, diagnosis, and treatment. Retrieved from http://www.nlm.nih.gov/medlineplus/magazine/issues/spring11/articles/spring11pg5-6.html.
The experience of pain is not only the result of physiology and psychology, but cultural
implications also play a role. [1] The role of culture
and the experience of pain has been an ongoing area of research since the early
1950s. [2] Included in such research are the
role that one’s culture plays in the experience of pain, the influence that culture has
in the treatment of pain, and the resources available for pain
treatment. [1] As an example,
research has stated that certain racial and ethnic groups are more likely to delay care
for pain assessment and treatment. Hispanics were seen at greater risk for injury and
pain due to the nature of their employment and the willingness to engage in jobs that
put physical wellness at risk for the sake of their families. In addition,
other research has suggested that Hispanics, when compared with Caucasians, will report
a greater magnitude of pain for a given pain issue. [1]
It is not completely known why the above may be, however, it is suggested that the level
of pain may be related to biological predisposition for certain ethnic/minority groups
when compared to others. For instance, people of Asian and Hispanic origin will
often need different dosages of certain medications when compared to Caucasians. [1] It
has also been suggested that Hispanics may not immediately seek treatment for pain due
to something known as aguantar. This means physical pain, and
even emotional pain, is more self managed and pain should be faced with dignity. [2]
References
- International Association for the Study of Pain.
(2002).
Hypnosis. Pain: Clinical Updates X(5).
Retrieved from
http://www.iasp-pain.org/AM/AMTemplate.cfm?Section=HOME,HOME&CONTENTID=7578&TEMPLATE=/CM/ContentDisplay.cfm&SECTION=HOME,HOME.
- Hernandez, A., and Sachs-Ericsson, N.
(2006).
"Ethnic differences in pain reports and the moderating role of
depression in a community sample of Hispanic and Caucasian participants
with serious health problems." Psychosomatic Medicine. Volume 68. Number
1. 121–128 Pages.
Mindfulness is paying attention—without
judgement—to what is happening right now, moment by moment by moment.
Society appears to have become faster paced. In other words, what once was managing school
or work for college students, and many high school students, now becomes managing work and school. For the high school
students who are not working, they might be involved with managing school and
extracurricular activities. That same pattern of school and extracurricular activities is
also seen in middle and elementary school students. For those younger students who are not
driving, it is the responsibilities of parents and/or caregivers to transport them to such
activities. This becomes even more burdensome for caregivers who have more than one child
involved with activities as the parents now have to manage their work schedules with the
activities of more than one child.
The above can be characteristic of the life experiences for many people, but most people seem to have their
own unique experiences where they are attempting to spin one too many plates. It seems that
managing many responsibilities at one time has become the norm. The consequence of this
however, is that people run the risk of ignoring their own needs. Never giving an
opportunity to “check in” with themselves.
In modern day society, the opposing concepts of multitasking and
mindfulness have become more familiar. Although multitasking has
become more of the norm, mindful experiences can help “recharge batteries” and keep a
person feeling balanced in a society that can “drain batteries.”
The concept of mindfulness can be difficult to describe in that it can be more of an
experience. In earlier modules mindfulness was described as a form of multi-sensory
awareness that allows people to be present, focused, and recognize where they are at from
moment to moment. It was also described as the ability to do one thing at a time with all
energy and focus on that one thing.
A Mind-Body Connection
Recognition that a mind-body connection exists and affects our health and overall
sense of well-being has been unfolding since the 1960s. For the past 40+ years,
various fields of healthcare have blended aspects of holistic mind and spiritual
based practices with the more physical centric and detail oriented aspects of western
medicine to develop approaches and techniques to treatment which are often referred
to as complementary medicine or alternative therapies.
Western practitioners have drawn on ancient, as well as contemporary, healing
practices from China, India, and Tibet.
This timeline highlights some of the most important events and research studies that
have furthered both our understanding and practice of mind-body medicine over the
past five decades.
-
Herbert Benson (1960s and 1970s)
Considered the godfather of mind-body medicine because of his pioneering work
on the effects of meditation on stress that led to identifying the “relaxation
response” in the early 1970s.
-
Robert Ader (mid-1970s)
One of the founders of the field known as
psychoneuroimmunology. This area of study focuses on the connection between the
mind and the body’s immune system.
-
Jon Kabat-Zinn (early 1980s)
Developed Mindfulness-Based Stress
Reduction program. Founded Stress Reduction Program at University of
Massachusetts Medical School in 1979.
-
David Spiegel (late 1980s)
Studied the effects of intensive
supportive-expressive group therapy for women with breast cancer.
-
Candace Pert (1980s)
Developed the theory of mind-body functions as
information molecules in the body. Her research has contributed to the study of
psychneuroimmunology.
-
Marsh M. Linehan (late 1980s)
Developed a therapy model known as
dialectical behavior therapy in which mindfulness is a major
component.
-
Sara Lazar (2000s)
Researches the mind-body connection using
neuroimaging techniques to study the effects of meditation on emotion and
cognition.
The basic definition of psychology is “science of the mind.” However, more recently,
psychology has incorporated more than just the mind. Several treatment approaches to
therapy have combined Eastern approaches to wellness with Western, more traditional,
“mind” approaches to psychology.
learn by doing
Watch this short video about Mindfulness-Based Stress Reduction (MBSR) and related
mindfulness-based approaches to wellness and them fill in the blanks to complete the
passage that follows.
did I get this
Decide whether or not each of the following items describes an aspect or
characteristic of mindfulness.
Mindfulness is a relatively new concept in Western culture and, as such,
is something to be practiced. In other words, and as previously noted,
society has become faster paced with more demands and less time for those
demands. Consequently, the quantity and quality of time to incorporate
mindfulness has to be gradually built. In other words, to take one moment
of being truly mindful is a starting point that can built into two, five,
ten, and then to thirty mindful minutes to focus, accomplish, and engage
in self care. Mindfulness was discussed as being present and in full
recognition of a moment. It was also described as the ability to do one
thing at a time with all energy and focus on that one thing. The ability
to engage in this practice can reduce vulnerability to potential
consequences of mindlessness and excessive
multi-tasking that include the experience of stress and/or the experience
of physical pain. Most importantly, the concept of mindfulness allows for
a feeling of self control in a world that can feel out of control.
learn by doing
You’ve already tried guided meditation earlier in this unit. The
following exercise will take a somewhat different approach derived from Buddhist
meditative practices, but also common to many other eastern religious traditions.
Rather than a guided meditation you are given 5 simple instructions.
Allocate approximately 15-30 minutes to this exercise. Many people find that this
type of meditation is most effective in a quiet, dimly lit place. It can also help to
meditate in the morning or in the late evening, when the potential for being
disturbed is lessened.
Instructions:
-
Find a Comfortable Place and Position: Sit or lay down; to
the best of your ability try to have your back and neck are aligned, yet relaxed.
Lying down is easiest, but many like to sit cross legged or in a lotus position on
the floor or on a pillow (don’t slouch).
-
Relax and Breathe Slowly: Close your eyes and relax. Slow
your breathing down and begin to breathe in through your nose and out through your
mouth. Breathe in from your diaphragm (midsection), not just your upper chest,
allowing your entire chest cavity to fill. Try to slow your breathing down to the
point that if there were a candle 12 inches away from your mouth, you would not
disturb it. Visualize the air entering through your nose and filling your lungs
and then slowly exiting out of your mouth.
-
Be Mindful of Your Thoughts and Move On: As your meditation
proceeds, your mind will begin to wander and you will start to think about past
and future events, responsibilities, hopes, worries, and the like. Rather than
allow each of these thoughts to occupy your mind, make a note of them and then
move on and refocus your attention on your breathing. This may be difficult at
first since you are likely new to this, but you’ll get the hang of it with some
practice.
-
Do Not Judge: Do not pass judgment on what comes to mind.
If you get stuck on something specific or your mind races, rather than get
frustrated note this as a topic that is occupying your mind and refocus on your
attention on your breathing. Don’t be hard on yourself if this is difficult, your
mind will eventually move on to another thought, or better yet, to visualizing air
entering your chest through your nose and exiting out through your mouth.
-
Pause to Note Your Surroundings When Finished: When you
feel that you’ve spent enough time on this exercise, mentally count upwards from 1
to 10 and open your eyes. Remain seated for a few minutes and observe your
surroundings. Take some time reflect on your meditation.
After completing steps 1-5, please consider the following.
learn by doing
Here is an opportunity for you to try a mindfulness meditation called the
“raisin meditation.” The video will guide you through this short
activity.
Your mind has a tendency to patterns in everything, particularly when you take the time to
mindfully attend to the scene. An even more direct approach is to present people with a
pattern to look for, like a face. This principle is behind a technique used by some
painters called the hidden faces illusion. At first blush these paintings look like typical
landscapes, but when primed to look for faces, people instantly become aware of the fact
that the scenery has been posed in face-like arrangements. Rather than painting such
scenes, a novel approach is to photograph natural scenes that contain patterns resembling
hidden faces.
learn by doing
Take a look at the image below which was taken in Pictograph Cave State Park in
Montana. What do you see?
Now take a look at the photograph one more time. How many faces can you find? There
is no correct answer, but most people can find 3 or more.
Let’s see if a type of attention meditation exercise can help you find more of
them.
You will be using a technique that is similar to things you’ve already practiced in
this unit. Take a few deep breaths and try to forget about your daily concerns. Take
a few minutes to allow your eye to wander over the photo, paying close attention to
the qualities of the rock-face. Be mindful of the scene, the 3D structure of the
rock, the varied hue, etc. Take the time to appreciate the natural beauty of what you
see.
Distress Tolerance Skills
As noted in the previous modules, dialectical behavior therapy (DBT) is a type of
therapy developed by Marsha M. Linehan [1] at
the University of Washington. It was originally developed for the treatment of
borderline personality disorder. However, more research has concluded that it can be
an effective treatment for mood, anxiety, eating, and substance abuse disorders.
Reviewing the three states of mind, reasonable mind is when a more intellectual
approach to life is assumed. To be in reasonable mind is to have the ability to think
logically and focus solely on facts. In emotional mind, attempts at logic can be
futile because thoughts can become nonfacts and further fuel emotions. Emotional mind
culminates in behaviors that are emotionally based but may have a long-term
consequence. Finally, an overlap of reasonable mind and emotional mind results in
wise mind. People in wise mind are mindful of an internal experience of escalating
emotions but also aware of long-term consequences of emotionally based behavior.
To increase the chances that a person stays in wise mind, DBT divides its curriculum
into four modules: core mindfulness skills, interpersonal effectiveness, distress
tolerance skills, and emotional regulation skills. Core mindfulness the increased
ability to attend to and “check in” with the self. In other words, how am I feeling
at a given moment? This takes practice as mindfulness is to be practiced in
situations that are non urgent as they lay the foundation for employing skills when
in an urgent situation. Interpersonal effectiveness is the practice of relating and
communicating well with others and being mindful of how communication can become
maladaptive and incorporating a communication skill to minimize the emotional
intensity of the communication.
Distress tolerance skills are the ability to be
incorporated a particular type of coping skill in a given moment when experiencing a
crisis. Emotion regulation is the module that helps gain insight into how emotions
work, and the skills required for management of emotions, as opposed to having
emotions manage the person. [1]
As an example, picture the ideal way to purchase a car. In the beginning stages,
purchasing a car can be a very reasonably minded task. In other words, research is
completed in that a person may choose a safe car that is fairly priced and gets good
gas mileage. This reasonable approach may also include saving enough money to buy a
late model used car without having payments.
Let’s take that same reasonable approach and walk into the dealership. Picture a
person being approached by a salesperson. The salesperson asks, “How may I help you?”
and the person takes out the printout of the make and model of the car that he wishes
to purchase outright, with cash and no payments. The salesperson then reviews the
computer printouts and acknowledges that this car is still in stock. However, the
salesperson says, “Before I take you to see your car, why don’t you have a seat in
this brand new car that is featured in our showroom?” Because the salesperson was
being nice, the customer decides to sit in this brand new car for a minute. And then,
it happens …
The salesperson shuts the door of this brand new SUV. The SUV has ZERO miles on it,
and the new car smell starts to stimulate the olfactory sense. The smooth, shiny
steering wheel is cool to the touch and feels good in the customer's hands. From
there, his thoughts start to change: “My $5,000 would be a good down payment on this
car,” “The gas prices aren’t going to go up all that much more,” “The six years worth
of payments will go by quick and, besides, everyone has a car payment.” With each
thought, the excitement grows and, before he realizes what is happening, the customer
is signing up for 6 years worth of payments, with interest, and more money will be
spent fueling and insuring the new car than he had anticipated.
So, what happened in the above scenario? The customer started off from a very
reasonable place. Once he entered the car, he was not being mindful of his emotional
experience. Rather, he was focusing on his thoughts, maybe even fantasizing what it
would be like when he rolled into his driveway. In other words, he became unmindful
of two things: his goal (to have reliable transportation without a payment) and his
emotional experience (the escalation of excitement).
Although DBT is primarily used in clinical settings, it can also be employed in
everyday life. For instance, with core mindfulness skills, building awareness and
learning how to name the emotion that is experienced when the door to the new SUV
shuts. The person probably felt a level of excitement and/or pressure. It’s one thing
to be able to label the emotion, but learning to describe the emotions can be a bit
more challenging. In other words, how does a person know he is becoming more excited
or feeling more pressure?
Internal cues of excitement and/or pressure may include:
- Sweating/perspiring
- Feeling jittery
- Muscles tensing
- Heaviness in stomach
Once the emotion is recognized, the person then requires some emotional regulation
and/or distress tolerance skills in order to minimize the chance of an emotionally
based decision and increase the chances of a wise minded decision. An example of an
emotional regulation skill would be to be mindful of the escalating emotion and do
the opposite of what the emotion is telling him to do. In the
case, the excitement is telling him to stay in the car and continue to smell the new
car and fantasize about driving out the showroom with this SUV. So, the opposite
would to exit the SUV.
An example of a distress tolerance skill would be to take a timeout, walk outside,
and take deep breaths. Once his emotions begin to subside, he can then walk back into
the showroom and be interpersonally effective with his salesperson. In other words,
from a wise-minded place, the customer can communicate with the salesperson in a
manner such as the following:
“I came in with a specific make and model in mind and with the exact amount of money
to pay it in full. I am feeling positive in my choice of vehicle, and I would like to
process the paperwork for the car that I came in for. If we start the process now,
you can get back to your day, see more customers, and I can be home at a decent
time.”
To be interpersonally effective is to communicate with only facts and without using
nonfacts, assumptions, or attacking. To be interpersonally effective also means to
express feelings based on the facts and assert the goal. Once the goal is stated,
then interpersonal effectiveness is also communicating the “wins” of keeping to the
goal. If the salesperson makes another attempt to sell a car that is not easily
afforded, to be interpersonally effective would be to recommunicate the goal and
positive consequences of achieving the goal.
The following video is a rap about "ACCEPTS" distress tolerance skills. Listen to strategies offered.
did I get this
Match the given behaviors with the appropriate ACCEPTS
skills and strategies. Each behavior has three specific examples.
Remember that all suggestions should be practiced mindfully. In other words, all attention and focus on that one thing.
Mindfulness can also be described in the form of the acronym, R.A.I.N:
“R” is the recognition of an emotional experience. In other words, and this will be
addressed in a later activity, an emotional experience begins with a body sensation. The
more mindful a person is about an internal emotional experience, the more likely that
person to recognize that emotion. “A” is either to allow or acknowledge that the emotion is
present. In other words, it would not be helpful to fight the presence of an emotion
because that would, in a sense, make the emotion much stronger. “I” is to investigate or
inquire. Not only recognizing and acknowledging the emotion but inquire as to why the
emotion might be present. Finally, “N” is to not to identify with the emotion. In other
words, one can be depressed without identifying him or herself as a depressed person. It is more accepting that in the present moment, the person is a
person feeling depressed and the depressed state is fleeting. To
practice R.A.I.N. is to decrease the chance that one does not become enmeshed with an
emotional experience. It allows a person to take a step back and increase the chances that
the person gains a deeper understanding on the function of the emotional experience, be it
depression, anger, or sadness.
learn by doing
Watch this TED lecture video given by neuroscientist Sara Lazar summarizing her own
experiences with mindful practices and the research it led her to do.
did I get this
You have already created a MBSR program for yourself, now it’s time to create a
wide-reaching wellness plan. A wellness plan is intended to correct current
imbalances in one’s wellness by having a person evaluate their physical/medical,
intellectual, spiritual, mental/emotional, social, financial, occupational and
environmental wellness. The following five step sequence will help you assess your
current wellness and come up with a practical, holistic plan to improve areas that
are lacking.
This is a very personal exercise and involves a serious consideration of your current
wellness and how it could be improved. If you are struggling with answering this
question, recruit a close friend or family member to help you with Steps 1-3. While a
face-to-face conversation is optimal, this could be done over the phone or through
electronic means of communication (Skype, chat, text message, email, etc.)
-
Assess: Assess your wellness in the following areas:
physical/medical, intellectual, spiritual, mental/emotional, social, financial,
occupational and environmental.
-
Rank: Rank order the areas that need improvement from most
to least impactful to your overall wellness, note the order (no need to rank the
areas in which you are doing well). Then rerank the same areas in terms of how
easy it is to make the needed changes; note the order. Items that occur toward the
top of both lists typically impact several other aspects of wellness, so effective
changes along these dimensions brings about a holistic effect.
-
Select Goals and Make Plan: Select a specific subset of
impactful, achievable goals for improving the items from Step #2. Create a
practical and pragmatic plan of action to accomplish these goals.
-
Keep Track of Progress: Create a wellness plan roadmap,
note your progress and highlight milestone achievements. Set realistic deadlines
and try to stick to them. If you don’t meet them, reassess your progress and set
new deadlines.
-
Be Flexible: As time passes your needs and surroundings
will change, so a wellness plan strives to be a living document. Thus, you should
regularly reassess whether your current plan optimally contributes to your current
understanding of wellness, and revise the plan if needed.
References
- Linehan, M.
(1993).
Skills Training Manual for Treating Borderline Personality
Disorder. Guilford Press. New York.
When Minor Body Imperfections Lead to Suicide
“I think we probably noticed in his early teens that he became very
conscious about aspects of his appearance....He began to brood over it quite a
lot,” said Maria as she called in to the talk radio program to describe her
son Robert.
Maria described how Robert had begun to worry about his weight. A friend had
commented that he had a “fat” stomach, and Robert began to cut down on
eating. Then he began to worry that he wasn’t growing enough and devised an
elaborate series of stretching techniques to help him get taller.
Robert scrutinized his face and body in the mirror for hours, finding a
variety of imagined defects. He believed that his nose was crooked, and he
was particularly concerned about a lump that he saw on it: “A small lump,”
said his mother. “I should say it wasn’t very significant, but it was
significant to him.”
Robert insisted that all his misery stemmed from this lump on his nose, that
everybody noticed it. In his sophomore year of high school, he had cosmetic
surgery to remove it.
Around this time, Robert had his first panic attack and began to worry that
everybody could notice him sweating and blushing in public. He asked his
parents for a $10,000 loan, which he said was for overseas study. He used
the money for a procedure designed to reduce sweating and blushing. Then,
dissatisfied with the results, he had the procedure reversed.
Robert was diagnosed with body dysmorphic disorder. His mother told the
radio host,
"At the time we were really happy because we thought that finally we
actually knew what we were trying to fight and to be quite honest, I must
admit I thought well it sounds pretty trivial....
"Things seemed to go quite well and he got a new girlfriend and he was
getting excellent marks in his clinical work in hospital and he promised us
that he wasn't going to have any more surgery."
However, a lighthearted comment from a friend about a noticeable vein in his
forehead prompted a relapse. Robert had surgery to tie off the vein. When
that didn’t solve all his problems as he had hoped, he attempted to have the
procedure reversed but learned that it would require complicated
microsurgery. He then used injections on himself to try opening the vein
again, but he could never completely reverse the first surgery.
Robert committed suicide shortly afterward, in
2001. [1]
Stop for a minute and consider what it means to be “normal” or “abnormal?” Is
it normal to wash your hands before you eat dinner? How hot should the water
be? How long should you wash your hands? When does this act of hand washing
move from what society views as “normal” to what others would deem “abnormal?”
You will learn that the types of behavior considered “normal” or “abnormal”
falls on a spectrum and is often less easily definable than you may have
thought. In this unit, we will explore these concepts and consider how
abnormality depends on both the consequences that result from a given behavior
and the culture in which someone lives.
Let’s begin with looking at the definition of a psychological disorder. A
psychological disorder is an ongoing dysfunctional pattern of thought, emotion,
and behavior that causes significant distress, impairs a person’s normal
functioning, and is considered deviant in that person’s culture or
society. [2]
Psychological disorders have much in common with other medical disorders. They
are out of the patient’s control, they may in some cases be treated by drugs,
and their treatment is often covered by medical insurance. Like medical
problems, psychological disorders have both biological (nature) as well as
environmental (nurture) influences. These causal influences are reflected in
the bio-psycho-social model of illness, a model that you will be learning about
later on in this module. [3]
Applying psychological science to our understanding and treatment of
psychological disorders is termed abnormal psychology. About
1 in every 4 Americans (or over 78 million people) are affected by a psychological disorder
during any one year, [4] and at least a half billion
people are affected worldwide. The impact of mental illness is particularly strong on
people who are poorer, of lower socioeconomic class, and from disadvantaged ethnic
groups.
People with psychological disorders are also stigmatized by the people around
them, resulting in shame and embarrassment, as well as prejudice and
discrimination against them. Thus the understanding and treatment of
psychological disorders has broad implications for the everyday life of many
people. The table below shows the prevalence (i.e., the frequency of occurrence of a given condition in a
population at a given time) of some of the major psychological
disorders in the United States.
| One-Year Prevalence Rates for Psychological Disorders in the United States |
|---|
| From Flat World Knowledge, Introduction to Psychology,
CC-BY-NC-SA.
Sources: Kessler, R. C., Chiu, W. T., Demler, O., and Walters, E. E. (2005).Prevalence,
severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity
Survey Replication. Archives of General Psychiatry,
62(6):617–627; Narrow, W. E., Rae, D. S., Robins, L. N., and Regier, D. A. (2002).
Revised prevalence based estimates of mental disorders in the United States: Using a
clinical significance criterion to reconcile 2 surveys’ estimates. Archives of General Psychiatry, 59(2):115–123. |
| Disease |
Percentage affected |
Number affected |
| Any mental disorder |
26.2 |
81,744,000 |
| Any anxiety disorder |
18.1 |
56,472,000 |
| Specific phobia |
8.7 |
27,144,000 |
| Social phobia |
6.8 |
21,216,000 |
| Agoraphobia |
0.8 |
2,496,000 |
| Generalized anxiety disorder |
3.1 |
9,672,000 |
| Panic disorder |
2.7 |
8,424,000 |
| Obsessive-compulsive disorder |
1.0 |
3,120,000 |
| Posttraumatic stress disorder |
3.5 |
10,920,000 |
| Any mood disorder |
9.5 |
29,640,000 |
| Major depressive disorder |
6.7 |
20,904,000 |
| Bipolar disorder |
2.6 |
8,112,000 |
| Schizophrenia |
1.0 |
3,120,000 |
| Personality disorders |
|
|
| Antisocial personality disorder |
1.5 |
4,680,000 |
| Borderline personality disorder |
1.5 |
4,680,000 |
| Anorexia nervosa |
0.1 |
312,000 |
| Any substance abuse disorder |
3.8 |
11,856,000 |
| Alcohol use disorder |
4.4 |
13,728,000 |
| Drug use disorder |
1.8 |
5,616,000 |
| All cancers* |
5.4 |
16,848,000 |
| Diabetes* |
10.7 |
33,348,000 |
| *These nonpsychological conditions are included for
comparison. |
|
|
|
In this unit our focus is on the disorders themselves. We review the major
psychological disorders and consider their causes and their impact on the
people who suffer from them.
References
- Mitchell, N. (Producer).
(2002).
Body Dysmorphic Disorder and Cosmetic “Surgery of the Psyche.” All in the mind. ABC Radio National. Retrieved from http://www.abc.net.au/rn/allinthemind/stories/2003/746058.htm.
- Butcher, J., Mineka, S., and Hooley, J.
(2007).
Abnormal Psychology and Modern Life. Allyn and Bacon. Boston. Edition 13.
- Engel, G.
(1977).
"The need for a new medical model: A challenge for biomedicine." Science. Volume 196. Number 4286. 129 Pages.
- Kessler, R. C., Chiu, W. T., Demler, O., and
Walters, E. E.
(2005).
"Prevalence, severity, and comorbidity of 12-month DSM-IV disorders
in the National Comorbidity Survey Replication." Archives of General
Psychiatry. Volume 62. Number 6. 617–627 Pages.
A psychological disorder is an ongoing
dysfunctional pattern of thought, emotion, and behavior that causes
significant distress, and that is considered deviant in that person’s
culture or society. [1]
Psychological disorders have much in common with other medical disorders. They
are out of the patient’s control, they may in some cases be treated by drugs,
and their treatment is often covered by medical insurance. Like medical
problems, psychological disorders have both biological (nature) as well as
environmental (nurture) influences. These causal influences are reflected in
the bio-psycho-social model of illness. [2]
The bio-psycho-social model of illness is a way of understanding disorder that assumes that disorders are
caused by biological, psychological, and social factors. The biological component of the bio-psycho-social model
refers to the influences on disorder that come from the functioning of the
individual’s body. Particularly important are genetic characteristics that make
some people more vulnerable to a disorder than others and the influence of
neurotransmitters. The psychological component of the
bio-psycho-social model refers to the influences that come from the individual,
such as patterns of negative thinking and stress responses. The social component of the bio-psycho-social model refers
to the influences on disorder due to social and cultural factors such as
socioeconomic status, homelessness, abuse, and discrimination.
To consider one example, the psychological disorder of schizophrenia has a
biological cause because it is known that there are patterns of genes that make
a person vulnerable to the
disorder. [3] But whether or not the
person with a biological vulnerability experiences the disorder depends in
large part on psychological factors such as how the individual responds to the
stress he experiences, as well as social factors such as whether or not he is
exposed to stressful environments in adolescence and whether or not he has
support from people who care about
him. [4] [5]
Similarly, mood and anxiety disorders are caused in part by genetic factors
such as hormones and neurotransmitters, in part by the individual’s particular
thought patterns, and in part by the ways that other people in the social
environment treat the person with the disorder. We will use the
bio-psycho-social model as a framework for considering the causes and
treatments of disorder.
Although they share many characteristics with them, psychological disorders are
nevertheless different from medical conditions in important ways. For one,
diagnosis of psychological disorders can be more difficult. Although a medical
doctor can see cancer in the lungs using an MRI scan or see blocked arteries in
the heart using cardiac catheterization, there is no corresponding test for
psychological disorder. Current research is beginning to provide more evidence
about the role of brain structures in psychological disorder, but for now the
brains of people with severe mental disturbances often look identical to those
of people without such disturbances.
Because there are no clear biological diagnoses, psychological disorders are
instead diagnosed on the basis of clinical observations of the behaviors that
the individual engages in. These observations find that emotional states and
behaviors operate on a continuum, ranging from more “normal” and “accepted” to
more “deviant,” “abnormal,” and “unaccepted.” The behaviors that are associated
with disorder are in many cases the same behaviors we that engage in our
“normal” everyday life. Washing one’s hands is a normal healthy activity, but
it can be overdone by those with an obsessive-compulsive
disorder (OCD). It is not unusual to worry about and try to improve
one’s body image, but Robert’s struggle with his personal appearance, as
discussed at the beginning of this module, was clearly unusual, unhealthy, and
distressing to him.
Whether a given behavior is considered a psychological disorder is determined
not only by whether a behavior is unusual (e.g.,
whether it is “mild” anxiety versus “extreme” anxiety) but also by whether a
behavior is maladaptive—that is, the extent to which it causes distress (e.g., pain and suffering) and dysfunction (impairment in one or more important areas
of functioning) to the
individual. [6] An intense fear
of spiders, for example, would not be considered a psychological disorder
unless it has a significant negative impact on the sufferer’s life, for
instance by causing him or her to be unable to step outside the house. The
focus on distress and dysfunction means that behaviors that are simply unusual
(such as some political, religious, or sexual practices) are not classified as
disorders.
Another difficulty in diagnosing psychological disorders is that they
frequently occur together. For instance, people diagnosed with anxiety
disorders also often have mood
disorders, [7] and people diagnosed
with one personality disorder frequently suffer from other personality
disorders as well. Comorbidity occurs
when people who suffer from one disorder also suffer at the same time from
other disorders. Because many psychological disorders are comorbid,
most severe mental disorders are concentrated in a small group of people (about
6% of the population) who have more than three of
them. [8]
Psychology in Everyday Life: Combating the Stigma of Abnormal
Behavior
Every culture and society has its own views on what constitutes abnormal
behavior and what causes it. [9] The Old
Testament Book of Samuel tells us that as a consequence of his sins, God
sent King Saul an evil spirit to torment him (1 Samuel 16:14). Ancient
Hindu tradition attributed psychological disorders to sorcery and
witchcraft. During the Middle Ages it was believed that mental illness
occurred when the body was infected by evil spirits, particularly the
devil. Remedies included whipping, bloodletting, purges, and trepanation
(cutting a hole in the skull) to release the demons.
Until the 18th century, the most common treatment for the mentally ill
was to incarcerate them in asylums or “madhouses.” During the 18th
century, however, some reformers began to oppose this brutal treatment of
the mentally ill, arguing that mental illness was a medical problem that
had nothing to do with evil spirits or demons. In France, one of the key
reformers was Philippe Pinel (1745–1826), who believed that mental
illness was caused by a combination of physical and psychological
stressors, exacerbated by inhumane conditions. Pinel advocated the
introduction of exercise, fresh air, and daylight for the inmates, as
well as treating them gently and talking with them. In America, the
reformers Benjamin Rush (1745–1813) and Dorothea Dix (1802–1887)
were instrumental in creating mental hospitals that
treated patients humanely and attempted to cure them if possible. These
reformers saw mental illness as an underlying psychological disorder,
which was diagnosed according to its symptoms and which could be cured
through treatment.
The reformers Philippe Pinel, Benjamin Rush, and Dorothea Dix fought the
often brutal treatment of the mentally ill and were instrumental in
changing perceptions and treatment of them.
Despite the progress made since the 1800s in public attitudes about those
who suffer from psychological disorders, people, including police,
coworkers, and even friends and family members, still stigmatize people
with psychological disorders. A stigma refers to
a disgrace or defect that indicates that person
belongs to a culturally devalued social group. In some cases the
stigma of mental illness is accompanied by the use of disrespectful and
dehumanizing labels, including names such as “crazy,” “nuts,” “mental,”
“schizo,” and “retard.” The stigma of mental disorder affects people
while they are ill, while they are healing, and even after they have
healed. [10] On a community level, stigma can
affect the kinds of services social service agencies give to people with
mental illness, and the treatment provided to them and their families by
schools, workplaces, places of worship, and health-care providers. Stigma
about mental illness also leads to employment discrimination, despite the
fact that with appropriate support, even people with severe psychological
disorders are able to hold a
job. [11] [12] [13] [14]
The mass media has a significant influence on society’s attitude toward mental
illness. [15] While media portrayal of
mental illness is often sympathetic, negative stereotypes still remain in newspapers,
magazines, film, and television. (See the following video for an example.) Television
advertisements may perpetuate negative stereotypes about the mentally ill. Burger
King recently ran an ad called “The King’s Gone Crazy” in which the company’s mascot
runs around an office complex carrying out acts of violence and wreaking havoc.
The most significant problem of the stigmatization of those with
psychological disorder is that it slows their recovery. People with
mental problems internalize societal attitudes about mental illness,
often becoming so embarrassed or ashamed that they conceal their
difficulties and fail to seek treatment. Stigma leads to lowered
self-esteem, increased isolation, and hopelessness, and it may negatively
influence the individual’s family and professional
life. [16]
Despite all of these challenges, however, many people overcome
psychological disorders and go on to lead productive lives. It is up to
all of us who are informed about the causes of psychological disorder and
the impact of these conditions on people to understand, first, that
mental illness is not a “fault” any more than is cancer. People do not
choose to have a mental illness. Second, we must all work to help
overcome the stigma associated with disorder. Organizations such as the
National Alliance on Mental Illness, [17] for
example, work to reduce the negative imp3act of stigma through education,
community action, individual support, and other techniques.
References
- Butcher, J., Mineka, S., and Hooley, J.
(2007).
Abnormal Psychology and Modern Life. Allyn and Bacon. Boston. Edition 13.
- Engel, G.
(1977).
"The need for a new medical model: A challenge for biomedicine." Science. Volume 196. Number 4286. 129 Pages.
- Gejman, P., Sanders, A., and Duan, J.
(2010).
"The role of genetics in the etiology of schizophrenia."
Psychiatric Clinics of North America. Volume 33. Number 1. 35–66 Pages.
- Sawa, A., and Snyder, S.
(2002).
"Schizophrenia: Diverse approaches to a complex disease." Science. Volume 296. Number 5568. 692–695 Pages.
- Walker, E., Kestler, L., Bollini, A., and Hochman, K.
(2004).
"Schizophrenia: Etiology and course." Annual Review of Psychology. Volume 55. Number 1. 401–430 Pages.
- American Psychiatric Association
(2000).
Diagnostic and Statistical Manual of Mental Disorders. Author. Washington, DC. Edition 4, text rev.
- Hunt, C., Slade, T., and Andrews, G.
(2004).
"Generalized anxiety disorder and major depressive disorder
comorbidity in the National Survey of Mental Health and Well Being."
Depression and Anxiety. Volume 20. Number 1. 23–31 Pages.
- Kessler, R. C., Chiu, W. T., Demler, O., and
Walters, E. E.
(2005).
"Prevalence, severity, and comorbidity of 12-month DSM-IV disorders
in the National Comorbidity Survey Replication." Archives of General
Psychiatry. Volume 62. Number 6. 617–627 Pages.
- Brothwell, D.
(1981).
Digging Up Bones: The Excavation, Treatment, and Study of Human Skeletal Remains. Cornell University Press. Ithaca, NY.
- Schefer, R.
(2003, May 28).
Addressing Stigma: Increasing Public Understanding of Mental Illness.
Presented to the Standing Senate Committee on Social Affairs, Science
and Technology. Retrieved from
http://www.camh.net/education/Resources_communities_organizations/addressing_stigma_senatepres03.pdf.
- Boardman, J., Grove, B., Perkins, R., and
Shepherd, G.
(2003).
"Work and employment for people with psychiatric disabilities."
British Journal of Psychiatry. Volume 182. Number 6. 467–468 Pages.
- Leff, J., and Warner, R.
(2006).
Social Inclusion of People with Mental Illness. Cambridge University Press. New York.
- Ozawa, A., and Yaeda, J.
(2007).
"Employer attitudes toward employing persons with psychiatric
disability in Japan." Journal of Vocational Rehabilitation. Volume 26.
Number 2. 105–113 Pages.
- Pulido, F., Diaz, M., and Ramírez, M.
(2004).
"Work integration of people with severe mental disorder: A pending
question." Revista Psiquis. Volume 25. Number 6. 26–43 Pages.
- Francis, C., Pirkis, J., Dunt, D., and Blood, R.
(2001).
Mental Health and Illness in the Media: A Review of the Literature. Commonwealth Department of Health and Aged Care. Canberra, Australia.
- Hayward, P., and Bright, J.
(1997).
"Stigma and mental illness: A review and critique." Journal of Mental Health. Volume 6. Number 4. 345–354 Pages.
- National Alliance on Mental Illness.
(n.d.).
Fight stigma. Retrieved from http://www.nami.org/template.cfm?section=fight_stigma.
Psychologists have developed criteria that help them determine whether behavior
should be considered a psychological disorder and which of the many disorders
particular behaviors indicate. These criteria are laid out in a 1,000-page
manual known as the Diagnostic and Statistical Manual of
Mental Disorders (DSM), a document that provides a
common language and standard criteria for the classification of mental
disorders. [1]
The DSM is used by therapists, researchers, drug
companies, health insurance companies, and policymakers in the United States to
determine what services are appropriately provided for treating patients with
given symptoms.
The first edition of the DSM was published in 1952 on
the basis of census data and psychiatric hospital statistics. Since then, the
DSM has been revised five times. The last major
revision was the fourth edition (DSM-IV), published in
1994, and an update of that document was produced in 2000 (DSM-IV-TR). The fifth edition (DSM-V) is
currently undergoing review, planning, and preparation and is scheduled to be
published in 2013. The DSM-IV-TR was designed in
conjunction with the World Health Organization’s 10th version of the International Classification of Diseases (ICD-10), which is used as a guide for mental disorders
in Europe and other parts of the world.
As you can see in the table below, the DSM organizes
the diagnosis of disorder according to five dimensions (or axes) relating to different aspects of disorder or disability. The
axes are important to remember when we think about psychological disorder,
because they make it clear not only that there are different types of disorder,
but that those disorders have a variety of different causes. Axis I includes the most usual clinical disorders, including mood disorders and anxiety
disorders; Axis II includes the less severe but
long-lasting personality disorders as well as mental
retardation; Axis III and Axis IV
relate to physical symptoms and social-cultural factors, respectively. The
axes remind us that when making a diagnosis we must look at the complete
picture, including biological, personal, and social-cultural factors.
| DSM Axes |
|---|
| The DSM organizes psychological disorders into
five dimensions (known as axes) that concern the different aspects of
disorder. From Flat World Knowledge, Introduction to Psychology, v1.0. Adapted from American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.). Washington, DC: Author |
| Axis I: Is a clinical syndrome, such as mood, anxiety, or learning
disorder, present? |
| Axis II: Is a personality disorder or mental retardation present? |
| Axis III: Is a general medical condition, such as heart disease,
diabetes, or cancer, present? |
| Axis IV: Are social or environmental problems, such as homelessness,
divorce, school problems, or other stressors, present? |
| Axis V: What is the global assessment of this person's functioning
(ranging from "persistent danger of hurting oneself or others" to
"superior functioning in a wide range of activities")? |
|
The DSM does not attempt to specify the exact symptoms
that are required for a diagnosis. Rather, the DSM uses
categories, and patients whose symptoms are similar to the description of the
category are said to have that disorder. The DSM
frequently uses qualifiers to indicate different levels of severity within
a category. For instance, the disorder of mental retardation can be classified
as mild, moderate, or severe.
Each revision of the DSM takes into consideration new
knowledge as well as changes in cultural norms about disorder. Homosexuality,
for example, was listed as a mental disorder in the DSM
until 1973, when it was removed in response to advocacy by politically
active gay rights groups and changing social norms. The current version of the
DSM lists about 400 disorders. Some of the major
categories are shown below, and you may go here
and browse the complete list.
 Categories of psychological disorders based on the DSM. From Flat World Knowledge, Introduction to Psychology, CC-BY-NC-SA.
Categories of psychological disorders based on the DSM. From Flat World Knowledge, Introduction to Psychology, CC-BY-NC-SA.
Although the DSM has been criticized regarding the
nature of its categorization system (and it is frequently revised to attempt to
address these criticisms), for the fact that it tends to classify more
behaviors as disorders with every revision (even “academic problems” are now
listed as a potential psychological disorder), and for the fact that it is
primarily focused on Western illness, it is nevertheless a comprehensive,
practical, and necessary tool that provides a common language to describe
disorder. Most U.S. insurance companies will not pay for therapy unless the
patient has a DSM diagnosis. The DSM
approach allows a systematic assessment of the patient, taking into
account the mental disorder in question, the patient’s medical condition,
psychological and cultural factors, and the way the patient functions in
everyday life.
References
- American Psychiatric Association
(2000).
Diagnostic and Statistical Manual of Mental Disorders. Author. Washington, DC. Edition 4, text rev.
Anxiety, the nervousness or agitation that we
sometimes experience, often about something that is going to happen, is a natural
part of life. We all feel anxious at times, maybe when we think about our upcoming visit to
the dentist or the presentation we have to give to our class next week. Anxiety is an
important and useful human emotion; it is associated with the activation of the sympathetic
nervous system and the physiological and behavioral responses that help protect us from
danger. But too much anxiety can be debilitating, and every year millions of people suffer
from anxiety disorders, which are psychological
disturbances marked by irrational fears, often of everyday objects and
situations. [1]
Consider the following, in which “Chase” describes her feelings of a persistent and
exaggerated sense of anxiety, even when there is little or nothing in her life to provoke
it:
For the past six months now I’ve had a really bad feeling inside
of me. The best way to describe it is like a really bad feeling of negative
inevitability, like something really bad is impending, but I don’t know what. It’s like
I’m on trial for murder or I’m just waiting to be sent down for something. I have it all
of the time but it gets worse in waves that come from nowhere with no apparent triggers.
I used to get it before going out for nights out with friends, and it kinda stopped me
from doing it as I’d rather not go out and stress about the feeling, but now I have it
for more days than not so it doesn’t really make a difference
anymore. [2]
Chase is probably suffering from a generalized anxiety disorder
(GAD), a psychological disorder diagnosed in situations in which a
person has been excessively worrying about money, health, work, family life, or
relationships for at least 6months, even though he or she knows that the concerns are
exaggerated, and when the anxiety causes significant distress and dysfunction.
In addition to their feelings of anxiety, people who suffer from GAD may also experience a
variety of physical symptoms, including irritability, sleep troubles, difficulty
concentrating, muscle aches, trembling, perspiration, and hot flashes. The sufferer cannot
deal with what is causing the anxiety, nor avoid it, because there is no clear cause for
anxiety. In fact, the sufferer frequently knows, at least cognitively, that there is really
nothing to worry about.
About 10 million Americans suffer from GAD, and about two thirds are women. [1] [3]
Generalized anxiety disorder is most likely to develop between the ages of 7 and 40 years,
but its influence may in some cases lessen with age. [4]
DSM IV-TR Criteria for Generalized Anxiety Disorder
Excessive anxiety about a number of events or activities, occurring more days than
not, for at least 6 months.
The person finds it difficult to control the worry.
The anxiety and worry are associated with at least three of the following six
symptoms (with at least some symptoms present for more days than not, for the past 6
months):
- Restlessness or feeling keyed up or on edge
- Being easily fatigued
- Difficulty concentrating or mind going blank
- Irritability
- Muscle tension
- Sleep disturbance
The focus of the anxiety and worry is not confined to features of an Axis I disorder,
being embarrassed in public (as in social phobia), being contaminated (as in
obsessive-compulsive disorder), being away from home or close relatives (as in
separation anxiety disorder), gaining weight (as in anorexia nervosa), having
multiple physical complaints (as in somatization disorder), or having a serious
illness (as in hypochondriasis), and the anxiety and worry do not occur exclusively
during posttraumatic stress disorder.
The anxiety, worry, or physical symptoms cause clinically significant distress or
impairment in social or occupational functioning.
The disturbance does not occur exclusively during a mood disorder, a psychotic
disorder, pervasive developmental disorder, substance use, or general medical
condition. [5]
References
- Kessler, R. C., Chiu, W. T., Demler, O., and Walters, E. E.
(2005).
"Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the
National Comorbidity Survey Replication." Archives of General Psychiatry. Volume 62. Number 6. 617–627 Pages.
- Chase (forum member).
(2010, February 28).
Re: “anxiety?” [Online forum comment]. Mental Health Forum. Retrieved from
http://www.mentalhealthforum.net/forum/showthread.php?t=9359.
- Robins, L., and Regier, D. A.
(1991).
Psychiatric Disorders in America: The Epidemiologic Catchment Area
Study. Free Press. New York.
- Rubio, G., and Lopez-Ibor, J.
(2007).
"Generalized anxiety disorder: A 40-year follow up study." Acta
Psychiatric Scandinavica. Volume 115. Number 4. 345–354 Pages.
- American Psychiatric Association
(2000).
Diagnostic and Statistical Manual of Mental Disorders. Author. Washington, DC. Edition 4, text rev.
When I was about 30 I had my first panic attack. I was driving home, my three little
girls were in their car seats in the back, and all of a sudden I couldn’t breathe, I
broke out into a sweat, and my heart began racing and literally beating against my ribs!
I thought I was going to die. I pulled off the road and put my head on the wheel. I
remember songs playing on the CD for about 15 minutes and my kids’ voices singing along.
I was sure I’d never see them again. And then, it passed. I slowly got back on the road
and drove home. I had no idea what it was. [1]
Ceejay is experiencing panic disorder, a
psychological disorder characterized by sudden attacks of anxiety and terror that have
led to significant behavioral changes in the person’s life. Symptoms of a panic
attack include shortness of breath, heart palpitations, trembling, dizziness, choking
sensations, nausea, and an intense feeling of dread or impending doom. Panic attacks can
often be mistaken for heart attacks or other serious physical illnesses, and they may lead
the person experiencing them to go to a hospital emergency room. Panic attacks may last as
little as one or as much as 20 minutes, but they often peak and subside within about 10
minutes.
Sufferers are often anxious because they fear that they will have another attack. They
focus their attention on the thoughts and images of their fears, becoming excessively
sensitive to cues that signal the possibility of threat. [2]
They may also become unsure of the source of their arousal, misattributing it to situations
that are not actually the cause. As a result, they may begin to avoid places where attacks
have occurred in the past, such as driving, using an elevator, or being in public places.
Panic disorder affects about 3% of the American population in a given year.
DSM IV-TR Criteria for Panic Disorder
Recurrent unexpected panic attacks
At least one of the attacks has been followed by at least 1 month of one or more of
the following:
- Persistent concern about having additional panic attacks
- Worry about the implications of the attack or its consequences
- A significant change in behavior related to the attacks
Presence or absence of agoraphobia
The panic attacks are not due to the direct physiologic effects of a substance (e.g.,
a drug of abuse, a medication) or a general medical condition (e.g.,
hyperthyroidism).
The panic attacks are not better accounted for by another mental disorder. [3]
References
- Ceejay (forum blogger).
(2006, September).
My dance with panic [Web log post]. Panic Survivor. Retrieved from
http://www.panicsurvivor.com/index.php/2007102366/Survivor-Stories/My-Dance-With-Panic.html.
- MacLeod, C., Rutherford, E., Campbell, L., Ebsworthy, G., and Holker,
L.
(2002).
"Selective attention and emotional vulnerability: Assessing the causal basis
of their association through the experimental manipulation of attentional
bias." Journal of Abnormal Psychology. Volume 111. Number 1. 107–123 Pages.
- American Psychiatric Association
(2000).
Diagnostic and Statistical Manual of Mental Disorders. Author. Washington, DC. Edition 4, text rev.
A phobia (from the Greek word phobos, which
means “fear”) is a specific fear of a certain object, situation, or
activity. The fear experience can range from a sense of unease to a full-blown
panic attack. Most people learn to live with their phobias, but for others the fear can be
so debilitating that they go to extremes to avoid the fearful situation. A sufferer of
arachnophobia (fear of spiders), for example, may refuse to enter a room until it has been
checked thoroughly for spiders, or may refuse to vacation in the countryside because
spiders may be there. Phobias are characterized by their specificity and their
irrationality. A person with acrophobia (a fear of height) could fearlessly sail around the
world on a sailboat with no concerns yet refuse to go out onto the balcony on the fifth
floor of a building.
A common phobia is social phobia, extreme shyness
around people or discomfort in social situations. Social phobia may be specific to
a certain event, such as speaking in public or using a public restroom, or it can be a more
generalized anxiety toward almost all people outside of close family and friends. People
with social phobia will often experience physical symptoms in public, such as sweating
profusely, blushing, stuttering, nausea, and dizziness. They are convinced that everybody
around them notices these symptoms as they are occurring. Women are somewhat more likely
than men to suffer from social phobia.
The most incapacitating phobia is agoraphobia, defined as anxiety about being in places or situations from which escape might be
difficult or embarrassing, or in which help may not be available. [1] Often,
agoraphobia occurs together with panic disorder, or the individual may be concerned about
having a panic attack in the feared situations or places. Typical places that provoke the
panic attacks are parking lots; crowded streets or shops; and bridges, tunnels, or
expressways. People (mostly women) who suffer from agoraphobia may have great difficulty
leaving their homes and interacting with other people.
Phobias affect about 9% of American adults, and they are about twice as prevalent in women
as in men. [2] [3]
In most cases phobias first appear in childhood and adolescence and usually persist into
adulthood.
DSM IV-TR Criteria for Specific Phobia
Persistent fear that is excessive or unreasonable, cued by the presence or
anticipation of a specific object or situation.
Exposure provokes immediate anxiety, which can take the form of a situationally
predisposed panic attack.
Patients recognize that the fear is excessive or unreasonable.
Patients avoid the phobic situation or else endure it with intense anxiety or
distress.
The distress in the feared situation interferes significantly with the person's
normal routine, occupational functioning, or social activities or relationships.
In persons younger than 18 years, the duration is at least 6 months.
The fear is not better accounted for by another mental disorder. [1]
DSM IV-TR Criteria for Social Phobia
A fear of one or more social or performance situations in which the person is exposed
to unfamiliar people or to possible scrutiny by others and feels he or she will act
in an embarrassing manner.
Exposure to the feared social situation provokes anxiety, which can take the form of
a panic attack.
The person recognizes that the fear is excessive or unreasonable.
The feared social or performance situations are avoided or are endured with
distress.
The avoidance, anxious anticipation, or distress in the feared situation interferes
significantly with the person's normal routine, occupational functioning, or social
activities or relationships.
The condition is not better accounted for by another mental disorder, substance use,
or general medical condition.
If a general medical condition or another mental disorder is present, the fear is
unrelated to it.
The phobia may be considered generalized if fears include most social situations. [1]
DSM IV-TR Criteria for Agoraphobia
Fear of being in places or situations from which escape might be difficult (or
embarrassing) or in which help might not be available in the event of having
unexpected panic-like symptoms.
The situations are typically avoided or require the presence of a companion.
The condition is not better accounted for by another mental disorder. [1]
References
- American Psychiatric Association
(2000).
Diagnostic and Statistical Manual of Mental Disorders. Author. Washington, DC. Edition 4, text rev.
- Fredrikson, M., Annas, P., Fischer, H., and Wik, G.
(1996).
"Gender and age differences in the prevalence of specific fears and
phobias." Behaviour Research and Therapy. Volume 34. Number 1. 33–39 Pages.
- Kessler, R., Meron-Ruscio, A., Shear, K., and Wittchen, H.
(2009).
Oxford Handbook of Anxiety and Related Disorders. Chapter Epidemiology of anxiety disorders. Oxford University Press. New York. M. Anthony, and M. Stein (Eds.).
Although he is best known for his perfect shots on the field, soccer star David Beckham
also suffers from obsessive-compulsive disorder (OCD). As he describes it, David Beckham’s
experience with obsessive behavior is not unusual. We all get a little obsessive at times.
We may continuously replay a favorite song in our heads, worry about getting the right
outfit for an upcoming party, or find ourselves analyzing a series of numbers that seem to
have a certain pattern. And our everyday compulsions can be useful. Going back inside the
house once more to be sure that we really did turn off the sink faucet or checking the
mirror a couple of times to be sure that our hair is combed are not necessarily bad
ideas.
Obsessive-compulsive disorder (OCD) is a
psychological disorder that is diagnosed when an individual continuously experiences
obsessions (distressing, intrusive, or frightening thoughts), and engages in
compulsions (repetitive behaviors or mental acts) in an attempt to
calm these obsessions. OCD is diagnosed when the obsessive thoughts are so
disturbing and the compulsive behaviors are so time consuming that they cause distress and
significant dysfunction in a person’s everyday life. Washing your hands once or even twice
to make sure that they are clean is normal; washing them 20 times is not. Keeping your
fridge neat is a good idea; spending hours a day on it is not. The sufferers know that
these rituals are senseless, but they cannot bring themselves to stop them, in part because
the relief they feel after they perform them acts as a reinforcer, making the behavior more
likely to occur again.
Sufferers of OCD may avoid certain places that trigger the obsessive thoughts or may use
alcohol or drugs to try to calm themselves down. OCD has a low prevalence rate (about 1% of
the population in a given year) in relation to other anxiety disorders and usually develops
in adolescence or early adulthood. [1] [2] The
course of OCD varies from person to person. Symptoms can come and go, decrease, or worsen
over time.
DSM IV-TR Criteria for Obsessive-Compulsive Disorder
Obsessions
- Recurrent and persistent thoughts, impulses, or images that are
experienced as intrusive and inappropriate, causing anxiety or distress.
- The thoughts, impulses, or images are not simply excessive worries about real-life problems.
- The person attempts to ignore or suppress such thoughts, impulses,
or images or to neutralize them with some other thought or action.
- The person recognizes that the obsessional thoughts, impulses, or images are a product of his or her own mind.
Compulsions
- Repetitive behaviors or mental acts that the person feels driven to
perform in response to an obsession or according to rules that must be
applied rigidly.
- The behaviors or mental acts are aimed at preventing or reducing distress or preventing some dreaded event or situation.
- These behaviors or mental acts either are not connected in a
realistic way with what they are designed to neutralize or prevent, or
they are clearly excessive.
Obsessive-Compulsive Disorder
- At some point during the course of the disorder, the person has
recognized that the obsessions or compulsions are excessive or
unreasonable.
- The obsessions or compulsions cause marked distress, take up more
than 1 hour a day, or significantly interfere with the person's normal
routine, occupation, or usual social activities.
- If another Axis I disorder, substance use, or general medical
condition is present, the content of the obsessions or compulsions is
not restricted to it. [3]
References
- Horwath, E., and Weissman, M.
(2000).
"The epidemiology and cross-national presentation of
obsessive-compulsive disorder." Psychiatric Clinics of North America.
Volume 23. Number 3. 493–507 Pages.
- Samuels, J., and Nestadt, G.
(1997).
"Epidemiology and genetics of obsessive-compulsive disorder."
International Review of Psychiatry. Volume 9. Number 1. 61–71 Pages.
- American Psychiatric Association
(2000).
Diagnostic and Statistical Manual of Mental Disorders. Author. Washington, DC. Edition 4, text rev.
"If you imagine burnt pork and plastic, I can still taste it," says Chris Duggan, on his
experiences as a soldier in the Falklands War in 1982. "These helicopters were coming in
and we were asked to help get the boys off...when they opened the doors the stench was
horrendous."
When he left the army in 1986, he suffered from PTSD. "I was a bit psycho," he says. "I
was verbally aggressive, very uncooperative. I was arguing with my wife, and eventually
we divorced. I decided to change the kitchen around one day, get all new stuff, so I
threw everything out of the window. I was 10 stories up in a flat. I poured brandy all
over the video and it melted. I flooded the bathroom." [1]
People who have survived a terrible ordeal, such as combat, torture, sexual assault,
imprisonment, abuse, natural disasters, or the death of someone close to them may develop
posttraumatic stress disorder (PTSD). The anxiety may begin
months or even years after the event. People with PTSD experience high
levels of anxiety along with reexperiencing the trauma
(flashbacks), and a strong desire to avoid any reminders of the
event. They may lose interest in things they used to enjoy; startle easily; have
difficulty feeling affection; and may experience terror, rage, depression, or insomnia. The
symptoms may be felt especially when approaching the area where the event took place or
when the anniversary of that event is near.
PTSD affects about 5 million Americans, including victims of the 9/11 terrorist attacks,
the wars in Afghanistan and Iraq, and Hurricane Katrina. Sixteen percent of Iraq war
veterans, for example, reported experiencing symptoms of PTSD. [2] PTSD is a frequent outcome of childhood or adult
sexual abuse, a disorder that has its own Diagnostic and Statistical Manual of Mental Disorders (DSM) diagnosis. Women are more likely to develop PTSD than men. [3]
Not everyone who experiences a trauma will develop PTSD. Risk factors for PTSD include the
degree of the trauma’s severity, the lack of family and community support, and additional
life stressors. [4] Many people with PTSD also suffer
from another mental disorder, particularly depression, other anxiety disorders, and
substance abuse. [5]
DSM IV-TR Criteria for Posttraumatic Stress Disorder
The person has been exposed to a traumatic event in which both of the following were
present:
- The person experienced, witnessed, or was confronted with an event that involved
actual or threatened death or serious injury or a threat to the physical integrity
of others.
- The person's response involved intense fear, helplessness, or horror.
The traumatic event is persistently re-experienced in at least one of the following
ways:
- Recurrent and intrusive distressing recollections of the event, including images,
thoughts, or perceptions.
- Recurrent distressing dreams of the event.
- Acting or feeling as if the traumatic event were recurring, including a sense of
reliving the experience, illusions, hallucinations, and flashback episodes.
- Intense psychological distress at exposure to cues that symbolize an aspect of
the traumatic event.
- Physiologic reactivity on exposure to cues that symbolize or resemble an aspect
of the traumatic event.
The person persistently avoids stimuli associated with the trauma and has numbing of
general responsiveness including at least three of the following:
- Efforts to avoid thoughts, feelings, or conversations associated with the
trauma
- Efforts to avoid activities, places, or people that arouse recollections of the
trauma
- Inability to recall an important aspect of the trauma
- Markedly diminished interest or participation in significant activities
- Feeling of detachment or estrangement from others
- Restricted range of affect
Persistent symptoms of increased arousal are indicated by at least two of the
following:
- Difficulty falling or staying asleep
- Irritability or outbursts of anger
- Difficulty concentrating
- Hypervigilance
- Exaggerated startle response
Duration of the disturbance is more than 1 month.
The disturbance causes clinically significant distress or impairment in social,
occupational, or other important areas of functioning. [6]
learn by doing
For each person, select the diagnosis that best describes his or her symptoms.
References
- Gould, M.
(2007, October 10).
You can teach a man to kill but not to see dying. The Guardian. Retrieved from
http://www.guardian.co.uk/society/2007/oct/10/guardiansocietysupplement.socialcare2.
- Hoge, C., and Castro, C.
(2006).
"Post-traumatic stress disorder in UK and U.S. forces deployed to
Iraq." Lancet. Volume 368. Number 9538. 867 Pages.
- Davidson, J.
(2000).
"Trauma: The impact of post-traumatic stress disorder." Journal of
Psychopharmacology. Volume 14. Number 2 Suppl 1. S5–S12 Pages.
- Brewin, C., Andrews, B., and Valentine, J.
(2000).
"Meta-analysis of risk factors for posttraumatic stress disorder in
trauma-exposed adults." Journal of Consulting and Clinical Psychology. Volume 68. Number 5. 748–766 Pages.
- Brady, K. T., Back, S. E., and Coffey, S. F.
(2004).
"Substance abuse and posttraumatic stress disorder." Current
Directions in Psychological Science. Volume 13. Number 5. 206–209 Pages.
- American Psychiatric Association
(2000).
Diagnostic and Statistical Manual of Mental Disorders. Author. Washington, DC. Edition 4, text rev.
Both nature and nurture contribute to the development of anxiety disorders. In terms of
our evolutionary experiences, humans have evolved to fear dangerous situations. Those of
us who had a healthy fear of the dark, of storms, of high places, of closed spaces, and
of spiders and snakes were more likely to survive and have descendants. Our evolutionary
experience can account for some modern fears as well. A fear of elevators may be a
modern version of our fear of closed spaces, while a fear of flying may be related to a
fear of heights.
Also supporting the role of biology, anxiety disorders, including PTSD, are heritable, [1]
and molecular genetics studies have found a
variety of genes that are important in the expression of such disorders. [2] [3] Neuroimaging studies have found that anxiety
disorders are linked to areas of the brain that are associated with emotion, blood
pressure and heart rate, decision making, and action monitoring. [4] [5] People who experience PTSD also have a
somewhat smaller hippocampus in comparison with those who do not, and this difference
leads them to have a very strong sensitivity to traumatic events. [6]
Whether the genetic predisposition to anxiety becomes expressed as a disorder depends on
environmental factors. People who were abused in childhood are more likely to be anxious
than those who had normal childhoods, even with the same genetic disposition to anxiety
sensitivity. [7] And the most severe anxiety and
dissociative disorders, such as PTSD, are usually triggered by the experience of a major
stressful event. One problem is that modern life creates a lot of anxiety. Although our
life expectancy and quality of life have improved over the past 50 years, the same
period has also created a sharp increase in anxiety levels. [8] These
changes suggest that most anxiety disorders stem from perceived, rather than actual,
threats to our well-being.
Anxieties are also learned through classical and operant conditioning. Just as rats that
are shocked in their cages develop a chronic anxiety toward their laboratory environment
(which has become a conditioned stimulus for fear), rape victims may feel anxiety when
passing by the scene of the crime, and victims of PTSD may react to memories or
reminders of the stressful event. Classical conditioning may also be accompanied by stimulus generalization. A single dog bite can lead to
generalized fear of all dogs; a panic attack that follows an embarrassing moment in one
place may be generalized to a fear of all public places. People’s responses to their
anxieties are often reinforced. Behaviors become compulsive because they provide relief
from the torment of anxious thoughts. Similarly, leaving or avoiding fear-inducing
stimuli leads to feelings of calmness or relief, which reinforces phobic behavior.
References
- Hettema, J. M., Neale, M. C., and Kendler, K. S.
(2001).
"A review and meta-analysis of the genetic epidemiology of anxiety
disorders." American Journal of Psychiatry. Volume 158. Number 10.
1568–1578 Pages.
- Smoller, J., Paulus, M., Fagerness, J.,
Purcell, S., Yamaki, L., Hirshfeld-Becker, D., et al.
(2008).
"Influence of RGS2 on anxiety-related temperament, personality, and
brain function." Archives of General Psychiatry. Volume 65. Number 3.
298–308 Pages.
- Thoeringer, C., Ripke, S., Unschuld,
P., Lucae, S., Ising, M., Bettecken, T., et al.
(2009).
"The GABA transporter 1 (SLC6A1): A novel candidate gene for
anxiety disorders." Journal of Neural Transmission. Volume 116. Number
6. 649–957 Pages.
- Brown, T., and McNiff, J.
(2009).
"Specificity of autonomic arousal to DSM-IV panic disorder and
posttraumatic stress disorder." Behaviour Research and Therapy. Volume
47. Number 6. 487–493 Pages.
- Damsa, C., Kosel, M., and Moussally, J.
(2009).
"Current status of brain imaging in anxiety disorders." Current
Opinion in Psychiatry. Volume 22. Number 1. 96–110 Pages.
- Gilbertson, M. W., Shenton, M. E.,
Ciszewski, A., Kasai, K., Lasko, N. B., Orr, S. P., et al.
(2002).
"Smaller hippocampal volume predicts pathologic vulnerability to
psychological trauma." Nature Neuroscience. Volume 5. Number 11. 1242
Pages.
- Stein, M., Schork, N., and Gelernter, J.
(2008).
"Gene-by-environment (serotonin transporter and childhood maltreatment)
interaction for anxiety sensitivity, an intermediate phenotype for anxiety
disorders." Neuropsychopharmacology. Volume 33. Number 2. 312–319 Pages.
- Twenge, J. M.
(2006).
Generation Me: Why Today’s Young Americans Are More Confident, Assertive, Entitled—And More Miserable Than Ever Before. Free Press. New York.
The everyday variations in our feelings of happiness and sadness reflect our
mood, which can be defined as the
positive or negative feelings that are in the background of our everyday
experiences. In most cases we are in a relatively good mood, and this
positive mood has some positive consequences— it encourages us to do what needs
to be done and to make the most of the situations we are
in. [1] When we are in a good mood our thought processes
open up, and we are more likely to approach others. We are more friendly and
helpful to others when we are in a good mood than we are when we are in a bad
mood, and we may think more
creatively. [2]
On the other hand, when we are in a bad mood we are more likely to prefer to be
alone rather than interact with others, we focus on the negative things around
us, and our creativity suffers.
It is not unusual to feel “down” or “low” at times, particularly after a
painful event such as the death of someone close to us, a disappointment at
work, or an argument with a partner. We often get depressed when we are tired,
and many people report being particularly sad during the winter when the days
are shorter. Mood (or affective) disorders are psychological disorders in which the person’s mood negatively
influences his or her physical, perceptual, social, and cognitive
processes. People who suffer from mood disorders
tend to experience more intense—and particularly more intense negative—
moods. About 10% of the U.S. population suffers from a mood disorder in a given
year.
The most common symptom of mood disorders is negative mood, also known as
sadness or depression. Consider the feelings of this
person, who was struggling with depression and was diagnosed with major depressive disorder:
I didn’t want to face anyone; I didn’t want to talk to anyone. I didn’t really want to
do anything for myself....I couldn’t sit down for a minute really to do anything that
took deep concentration....It was like I had big huge weights on my legs and I was
trying to swim and just kept sinking. And I’d get a little bit of air, just enough to
survive and then I’d go back down again. It was just constantly, constantly just
fighting, fighting, fighting, fighting,
fighting. [3]
Recurrence of depressive episodes is fairly common and is greatest
for those who first experience depression before the age of 15 years. About
twice as many women suffer from depression than do
men. [4] This gender difference is consistent across
many countries and cannot be explained entirely by the fact that women are more
likely to seek treatment for their depression. Rates of depression have been
increasing over the past years, although the reasons for this increase are not
known. [5]
As you can see below, the experience of depression has a variety of negative
effects on our behaviors. In addition to the loss of interest, productivity,
and social contact that accompanies depression, the person’s sense of
hopelessness and sadness may become so severe that he or she considers or even
succeeds in committing suicide. Suicide is the 11th leading cause of death in
the United States, and a suicide occurs approximately every 16 minutes. Almost
all the people who commit suicide have a diagnosable psychiatric disorder at
the time of their
death. [6] [7] [8]
Behaviors Associated with Depression
- Changes in appetite; weight loss or gain
- Difficulty concentrating, remembering details, and making decisions
- Fatigue and decreased energy
- Feelings of hopelessness, helplessness, and pessimism
- Increased use of alcohol or drugs
- Irritability, restlessness
- Loss of interest in activities or hobbies once pleasurable, including
sex
- Loss of interest in personal appearance
- Persistent aches or pains, headaches, cramps, or digestive problems that do
not improve with treatment
- Sleep disorders, either trouble sleeping or excessive sleeping
- Thoughts of suicide or attempts at suicide
References
- Isen, A. M.
(2003).
A Psychology of Human Strengths: Fundamental Questions and Future Directions for a Positive Psychology.
Chapter Positive affect as a source of human strength. American
Psychological Association. Washington, DC. 179–195 Pages. J. Aspinall
(Ed.).
- De Dreu, C. K. W., Baas, M., and Nijstad, B.
A.
(2008).
"Hedonic tone and activation level in the mood-creativity link:
Toward a dual pathway to creativity model." Journal of Personality and
Social Psychology. Volume 94. Number 5. 739–756 Pages.
- National Institute of Mental Health.
(2010, April 8).
People with depression discuss their illness. Retrieved from http://www.nimh.nih.gov/media/video/health/depression.shtml.
- Culbertson, F. M.
(1997).
"Depression and gender: An international review." American Psychologist. Volume 52. Number 6. 25–31 Pages.
- Kessler, R. C., Berglund, P., Demler, O,
Jin, R., Koretz, D., Merikangas, K. R., et al.
(2003).
"The epidemiology of major depressive disorder: Results from the
National Comorbidity Survey Replication (NCS-R)." Journal of the
American Medical Association. Volume 289. Number 23. 3095–3105 Pages.
- American Association of Suicidology.
(2010, June 29).
Some facts about suicide and depression. Retrieved from http://www.suicidology.org/c/document_library/get_file?folderId=232&name=DLFE-246.pdf.
- American Foundation for Suicide Prevention.
(2007).
About suicide: Facts and figures. National statistics. Retrieved from http://www.afsp.org/index.cfm?fuseaction=home.viewpage&page_id= 050FEA9F-B064-4092-B1135C3A70DE1FDA.
- Sudak, H. S.
(2003).
Kaplan and Sadock’s Comprehensive Textbook of Psychiatry. Chapter Suicide. Lippincott Williams and Wilkins. Philadelphia. B. J. Sadock and V. A. Sadock (Eds.).
The level of depression observed in people with mood disorders varies widely. People who
experience depression for many years, such that it becomes to seem normal and part of
their everyday life, and who feel that they are rarely or never happy, will likely be
diagnosed with a mood disorder. If the depression is mild but long-lasting, they will be
diagnosed with dysthymia, a condition
characterized by mild, but chronic, depressive symptoms that last for at least 2
years.
If the depression continues and becomes even more severe, the diagnosis may
become that of major depressive disorder. Major depressive disorder (clinical depression) is a mental disorder characterized by an all-encompassing low
mood accompanied by low self-esteem and by loss of interest or pleasure in
normally enjoyable activities. Those who suffer from major depressive
disorder feel an intense sadness, despair, and loss of interest in pursuits
that once gave them pleasure. These negative feelings profoundly limit the
individual’s day-to-day functioning and ability to maintain and develop
interests in life. [1]
About 21 million American adults suffer from a major depressive disorder in any
given year; this is approximately 7% of the American population. Major
depressive disorder occurs about twice as often in women as it does in
men. [2] [3]
In some cases clinically depressed people lose contact with reality and may
receive a diagnosis of major depressive episode with
psychotic features. In these cases the depression includes delusions
and hallucinations.
References
- Fairchild, K., and Scogin, F.
(2008).
Handbook of Emotional Disorders in Later Life: Assessment and Treatment. Chapter Assessment and treatment of depression. Oxford University Press. New York. K. Laidlow and B. Knight (Eds.).
- Kessler, R. C., Berglund, P., Demler, O,
Jin, R., Koretz, D., Merikangas, K. R., et al.
(2003).
"The epidemiology of major depressive disorder: Results from the
National Comorbidity Survey Replication (NCS-R)." Journal of the
American Medical Association. Volume 289. Number 23. 3095–3105 Pages.
- Kessler, R. C., Chiu, W. T., Demler, O.,
and Walters, E. E.
(2005).
"Prevalence, severity, and comorbidity of 12-month DSM-IV disorders
in the National Comorbidity Survey Replication." Archives of General
Psychiatry. Volume 62. Number 6. 617–627 Pages.
Juliana is a 21-year-old single woman. Over the past several years she had
been treated by a psychologist for depression, but for the past few months
she had been feeling a lot better. Juliana had landed a good job in a law
office and found a steady boyfriend. She told her friends and parents that
she had been feeling particularly good—her energy level was high and she was
confident in herself and her life.
One day Juliana was feeling so good that she impulsively quit her new job
and left town with her boyfriend on a road trip. But the trip didn’t turn
out well because Juliana became impulsive, impatient, and easily angered.
Her euphoria continued, and in one of the towns that they visited she left
her boyfriend and went to a party with some strangers that she had met. She
danced into the early morning and ended up having sex with several of the
men.
Eventually Juliana returned home to ask for money, but when her parents
found out about her recent behavior, and when she acted aggressively and
abusively to them when they confronted her about it, they referred her to a
social worker. Juliana was hospitalized, where she was diagnosed with
bipolar disorder.
Whereas dysthymia and major depressive disorder are characterized by
overwhelming negative moods, bipolar disorder is a psychological disorder characterized by swings in mood from
overly “high” to sad and hopeless, and back again, with periods of
near-normal mood in between. Bipolar disorder is diagnosed in cases
such as Juliana’s, where experiences with depression are followed by a more
normal period and then a period of mania or euphoria in which the person feels
particularly awake, alive, excited, and involved in everyday activities but is
also impulsive, agitated, and distracted. Without treatment, it is likely that
Juliana would cycle back into depression and then eventually into mania again,
with the likelihood that she would harm herself or others in the process.
Bipolar disorder is an often chronic and lifelong condition that may begin in
childhood. Although the normal pattern involves swings from high to low, in
some cases the person may experience both highs and lows at the same time.
Determining whether a person has bipolar disorder is difficult due to the
frequent presence of comorbidity with both depression and anxiety disorders.
Bipolar disorder is more likely to be diagnosed when it is initially observed
at an early age, when the frequency of depressive episodes is high, and when
there is a sudden onset of the symptoms. [2]
References
- Thomas, P., and Bracken, P.
(2001).
"Vincent’s bandage: The art of selling a drug for bipolar
disorder." British Medical Journal. Volume 323. Number 7326. 1434 Pages.
- Bowden, C. L.
(2001).
"Strategies to reduce misdiagnosis of bipolar depression." Psychiatric Services. Volume 52. Number 1. 51–55 Pages.
Mood disorders are known to be at least in part genetic, because they are
heritable. [1] [2]
Neurotransmitters also play an important role in mood disorders. Serotonin,
dopamine, and norepinephrine are all known to influence
mood, [3] and drugs that influence the actions
of these chemicals are often used to treat mood disorders. The brains of those
with mood disorders may in some cases show structural differences from those
without them. Videbech and Ravnkilde [4] found that the
hippocampus was smaller in depressed subjects than in normal subjects, and this
may be the result of reduced neurogenesis (the process
of generating new neurons) in depressed
people. [5] Antidepressant drugs may
alleviate depression in part by increasing
neurogenesis. [6]
Research Focus: Using Molecular Genetics to Unravel the Causes of
Depression
Avshalom Caspi and his colleagues [7] used a
longitudinal study to test whether genetic predispositions might lead
some people, but not others, to suffer from depression as a result of
environmental stress. Their research focused on a particular gene, the
5-HTT gene, which is known to be important in the production and use of
the neurotransmitter serotonin. The researchers
focused on this gene because serotonin is known to be important in
depression, and because selective serotonin reuptake inhibitors (SSRIs)
have been shown to be effective in treating depression.
People who experience stressful life events, for instance involving
threat, loss, humiliation, or defeat, are likely to experience
depression. But biological-situational models suggest that a person’s
sensitivity to stressful events depends on his or her genetic makeup. The
researchers therefore expected that people with one type of genetic
pattern would show depression following stress to a greater extent than
people with a different type of genetic pattern.
The research included a sample of 1,037 adults from Dunedin, New Zealand.
Genetic analysis on the basis of DNA samples allowed the researchers to
divide the sample into two groups on the basis of the characteristics of
their 5-HTT gene. One group had a short version (or allele) of the gene, whereas the other group did not have the
short allele of the gene.
The participants also completed a measure where they indicated the number
and severity of stressful life events that they had experienced over the
past 5 years. The events included employment, financial, housing, health,
and relationship stressors. The dependent measure in the study was the
level of depression reported by the participant, as assessed using a
structured interview
test. [8]
As you can see in the figure below, as the number of stressful
experiences the participants reported increased from 0 to 4, depression
also significantly increased for the participants with the short version
of the gene (top panel). But for the participants who did not have a
short allele, increasing stress did not increase depression (bottom
panel). Furthermore, for the participants who experienced 4 stressors
over the past 5 years, 33% of the participants who carried the short
version of the gene became depressed, whereas only 17% of participants
who did not have the short version did.
This important study provides an excellent example of how genes and
environment work together: An individual’s response to environmental
stress was influenced by his or her genetic makeup.
But psychological and social determinants are also important in creating mood
disorders and depression. In terms of psychological characteristics, mood
states are influenced in large part by our cognitions. Negative thoughts about
ourselves and our relationships to others create negative moods, and a goal of
cognitive therapy for mood disorders is to attempt to change people’s
cognitions to be more positive. Negative moods also create negative behaviors
toward others, such as acting sad, slouching, and avoiding others, which may
lead those others to respond negatively to the person, for instance by
isolating that person, which then creates even more depression. You can see how
it might become difficult for people to break out of this “cycle of
depression.”
Weissman and colleagues [9] found that rates of depression varied greatly
among countries, with the highest rates in European and American countries and
the lowest rates in Asian countries. These differences seem to be due to
discrepancies between individual feelings and cultural expectations about what
one should feel. People from European and American
cultures report that it is important to experience emotions such as happiness
and excitement, whereas the Chinese report that it is more important to be
stable and calm. Because Americans may feel that they are not happy or excited
but that they are supposed to be, this may increase their
depression. [10]
References
- Berrettini, W.
(2008).
Textbook of Mood Disorders. Chapter
Genetics of bipolar and unipolar disorders. American Psychiatric
Publishing. Washington, DC. D. J. Stein, D. J. Kupfer, and A. F.
Schatzberg (Eds.).
- Merikangas, K., Chakravarti, A., Moldin, S., Araj, H., Blangero, J., Burmeister, M, et al.
(2002).
"Future of genetics of mood disorders research." Biological Psychiatry. Volume 52. Number 6. 457–477 Pages.
- Sher, L., and Mann, J. J.
(2003).
Psychiatry. Chapter Psychiatric pathophysiology: Mood disorders. Wiley. New York. A. Tasman, J. Kay, and J. A. Lieberma (Eds.).
- Videbech, P., and Ravnkilde, B.
(2004).
"Hippocampal volume and depression: A meta-analysis of MRI
studies." American Journal of Psychiatry. Volume 161. Number 11.
1957–1966 Pages.
- Warner-Schmidt, J. L., and Duman, R.
S.
(2006).
"Hippocampal neurogenesis: Opposing effects of stress and
antidepressant treatment." Hippocampus. Volume 16. Number 3. 239–249
Pages.
- Duman, R. S., and Monteggia, L. M.
(2006).
"A neurotrophic model for stress-related mood disorders." Biological Psychiatry. Volume 59. Number 12. 1116–1127 Pages.
- Caspi, A., Sugden, K., Moffitt, T. E., Taylor,
A., Craig, I. W., Harrington, H., et al.
(2003).
"Influence of life stress on depression: Moderation by a
polymorphism in the 5-HTT gene." Science. Volume 301. Number 5631.
386–389 Pages.
- Robins, L. N., Cottler, L., Bucholtz, K., and Compton, W.
(1995).
Diagnostic Interview Schedule for DSM-IV. Washington University. St. Louis, MO.
- Weissman, M. M., Bland, R. C., Canino, G.
J., Greenwald, S., Hwu, H-G., Joyce, P. R., et al.
(1996).
"Cross-national epidemiology of major depression and bipolar
disorder." Journal of the American Medical Association. Volume 276.
Number 4. 293–299 Pages.
- Tsai, J. L., Knutson, B., and Fung, H. H.
(2006).
"Cultural variation in affect valuation." Journal of Personality
and Social Psychology. Volume 90. Number 2. 288–307 Pages.
The term schizophrenia, which in Greek means “split mind,” was
first used to describe a psychological disorder by Eugen Bleuler (1857–1939), a Swiss
psychiatrist who was studying patients who had very severe thought disorders. Schizophrenia is a serious psychological disorder
marked by delusions, hallucinations, loss of contact with reality, inappropriate affect,
disorganized speech, social withdrawal, and deterioration of adaptive behavior.
Schizophrenia is the most chronic and debilitating of all psychological disorders. It
affects men and women equally, occurs in similar rates across ethnicities and across
cultures, and affects at any one time approximately 3 million people in the United
States. [1] Onset of schizophrenia is
usually between the ages of 16 and 30 and rarely after the age of 45 or in
children. [2] [3]
Schizophrenia is accompanied by a variety of symptoms, but not all patients
have all of them. [4] Symptoms are
divided into positive symptoms, negative symptoms, and cognitive
symptoms. [5] [1]
Positive symptoms refer to the presence of abnormal behaviors or experiences
(such as hallucinations) that are not observed in normal people, whereas
negative symptoms (such as lack of affect and an inability to socialize with
others) refer to the loss or deterioration of thoughts and behaviors that are
typical of normal functioning. Finally, cognitive symptoms are the changes in
cognitive processes that accompany schizophrenia. [6]
Because the person has lost contact with reality, we say that he or she is
experiencing psychosis, which is a
psychological condition characterized by a loss of contact with
reality.
People with schizophrenia often experience hallucinations—false sensations that occur in the
absence of a real stimulus or which are gross distortions of a real
stimulus. Auditory hallucinations are the most common and are reported
by approximately three quarters of
patients. [7]
Schizophrenic patients frequently report hearing voices that curse them,
comment on their behavior, order them to do things, or warn them of
danger. [8] Visual
hallucinations are less common and frequently involve seeing God or the
devil. [9]
People with schizophrenia also commonly experience delusions, which are false beliefs not commonly
shared by others within one’s culture, and maintained even though they are
obviously out of touch with reality. People with delusions of grandeur believe that they are important, famous, or
powerful. They often become convinced that they are someone else, such as the
president or God, or that they have some special talent or ability. Some claim
to have been assigned to a special covert
mission. [10] People with delusions of persecution believe that a person or group
seeks to harm them. They may think that people are able to read their minds and
control their thoughts. [11]
People with schizophrenia also often experience the positive symptom of derailment—the shifting from one subject to another, without following any one
line of thought to conclusion—and may exhibit grossly disorganized
behavior including inappropriate sexual behavior, peculiar appearance and dress,
unusual agitation (e.g., shouting and swearing), strange body movements, and awkward facial
expressions. It is also common for people with schizophrenia to experience inappropriate affect. For example, the person may laugh
uncontrollably when hearing sad news. Movement disorders typically appear as agitated
movements, such as repeating a certain motion again and again, but can in some cases
include catatonia, a state in which a person does not move and is
unresponsive to others. [12] [13]
Negative symptoms of schizophrenia include social withdrawal, poor
hygiene and grooming, poor problem-solving abilities, and a distorted sense of time. [6] Persons with schizophrenia often
suffer from flat affect, which means that they express almost no emotional response (e.g.,
they speak in a monotone and have a blank facial expression) even though they may report
feeling emotions. [14] Another negative
symptom is the tendency toward incoherent language, for instance, to repeat the speech of
others (“echo speech”). Some people with schizophrenia experience motor disturbances,
ranging from complete catatonia and apparent obliviousness to their environment to random
and frenzied motor activity during which they become hyperactive and incoherent. [15]
Not all people with schizophrenia exhibit negative symptoms, but those who do
also tend to have the poorest outcomes. [16]
Negative symptoms are predictors of deteriorated functioning in everyday life
and often make it impossible for people to work or to care for themselves.
Cognitive symptoms of schizophrenia are typically
difficult for outsiders to recognize but make it extremely difficult for the
individual to lead a normal life. These symptoms include difficulty
comprehending information and using it to make decisions (the lack of executive control), difficulty maintaining focus and
attention, and problems with working memory (the ability to use information
immediately after it is learned).
References
- National Institute of Mental Health.
(2010, April 26).
What is schizophrenia?. Retrieved from http://www.nimh.nih.gov/health/topics/schizophrenia/index.shtml.
- Mueser, K. T., and McGurk, S. R.
(2004).
"Schizophrenia." Lancet. Volume 363. Number 9426. 2063–2072 Pages.
- Nicolson, R., Lenane, M., Hamburger, S. D., Fernandez, T., Bedwell, J., and Rapoport, J. L.
(2000).
"Lessons from childhood-onset schizophrenia." Brain Research Review. Volume 31. Number 2–3. 147–156 Pages.
- Lindenmayer, J. P., and Khan, A.
(2006).
Textbook of Schizophrenia. Chapter
Psychological disorder. American Psychiatric Publishing. Washington, DC.
187–222 Pages. J. A. Lieberman, T. S. Stroup, and D. O. Perkins (Eds.).
- American Psychiatric Association
(2000).
Diagnostic and Statistical Manual of Mental Disorders. Author. Washington, DC. Edition 4, text rev.
- Skrabalo, A.
(2000).
"Negative symptoms in schizophrenia(s): The conceptual basis." Harvard Brain. Volume 7. Number 1. 7–10 Pages.
- Nicolson, S. E., Mayberg, H. S., Pennell,
P. B., and Nemeroff, C. B.
(2006).
"Persistent auditory hallucinations that are unresponsive to
antipsychotic drugs." American Journal of Psychiatry. Volume 163. Number
7. 1153–1159 Pages.
- National Institute of Mental Health.
(2009, September 8).
What are the symptoms of schizophrenia?. Retrieved from http://www.nimh.nih.gov/health/publications/schizophrenia/what-are-the-symptoms-of-schizophrenia.shtml.
- De Sousa, A.
(2007).
"Types and contents of hallucinations in schizophrenia." Journal of
Pakistan Psychiatric Society. Volume 4. Number 1. 9 Pages.
- Buchanan, R. W., and Carpenter, W. T.
(2005).
Kaplan and Sadock’s Comprehensive Textbook of Psychiatry. Chapter Concept of schizophrenia. Lippincott Williams and Wilkins. Philadelphia. B. J. Sadock and V. A. Sadock (Eds.).
- Maher, B. A.
(2001).
Comprehensive Handbook of Psychological Disorder. Chapter Delusions. Kluwer Academic/Plenum. New York. Edition 3. 309–370 Pages. P. B. Sutker and H. E. Adams (Eds.).
- Janno, S., Holi, M., Tuisku, K., and Wahlbeck,
K.
(2004).
"Prevalence of neuroleptic-induced movement disorders in chronic
schizophrenia patients." American Journal of Psychiatry. Volume 161.
Number 1. 160–163 Pages.
- Rosebush, P. I., and Mazurek, M. F.
(2010).
"Catatonia and its treatment." Schizophrenia Bulletin. Volume 36. Number 2. 239–242 Pages.
- Kring, A. M.
(1999).
"Emotion in schizophrenia: Old mystery, new understanding." Current
Directions in Psychological Science. Volume 8. Number 5. 160–163 Pages.
- Kirkpatrick, B., and Tek, C.
(2005).
Kaplan and Sadock’s Comprehensive Textbook of Psychiatry.
Chapter Schizophrenia: Clinical features and psychological disorder
concepts. Lippincott Williams and Wilkins. Philadelphia. 1416–1435
Pages. B. J. Sadock and S. V. Sadock (Eds.).
- Fenton, W. S., and McGlashan, T. H.
(1994).
"Antecedents, symptom progression, and long-term outcome of the
deficit syndrome in schizophrenia." American Journal of Psychiatry.
Volume 151. Number 3. 351–356 Pages.
There is no single cause of schizophrenia. Rather, a variety of biological and
environmental risk factors interact in a complex way to increase the likelihood
that someone might develop
schizophrenia. [1]
Studies in molecular genetics have not yet identified the particular genes
responsible for schizophrenia, but it is evident from research using family,
twin, and adoption studies that genetics are
important. [2] As you can see in
the figure below, the likelihood of developing schizophrenia increases
dramatically if a close relative also has the disease.
Neuroimaging studies have found some differences in brain structure between
schizophrenic and normal patients. In some people with schizophrenia, the
cerebral ventricles (fluid-filled spaces in the brain) are
enlarged. [3]
People with schizophrenia also frequently show an overall loss of neurons in
the cerebral cortex, and some show less activity in the frontal and temporal
lobes, which are the areas of the brain involved in language, attention, and
memory. This would explain the deterioration of functioning in language and
thought processing that is commonly experienced by schizophrenic
patients. [4]
Many researchers believe that schizophrenia is caused in part by excess
dopamine, and this theory is supported by the fact that most of the drugs
useful in treating schizophrenia inhibit dopamine activity in the
brain. [5] Levels of serotonin
may also play a part. [6] But recent evidence
suggests that the role of neurotransmitters in schizophrenia is more
complicated than was once believed. It also remains unclear whether observed
differences in the neurotransmitter systems of people with schizophrenia cause
the disease, or if they are the result of the disease itself or its
treatment. [7]
A genetic predisposition to developing schizophrenia does not always develop
into the actual disorder. Even if a person has an identical twin with
schizophrenia, he still has less than a 50% chance of getting it himself, and
over 60% of all people with schizophrenia have no first- or second-degree
relatives with the disorder. [8] [9] This suggests that there are important environmental
causes as well.
One hypothesis is that schizophrenia is caused in part by disruptions to normal
brain development in infancy that may be caused by poverty, malnutrition, and
disease. [10] [11] [12] [13] Stress also increases the
likelihood that a person will develop schizophrenic symptoms; onset and relapse
of schizophrenia typically occur during periods of increased stress. However, it may be that people who develop
schizophrenia are more vulnerable to stress than others and not necessarily
that they experience more stress than others. [14]
References
- Walker, E., Kestler, L., Bollini, A., and Hochman, K.
(2004).
"Schizophrenia: Etiology and course." Annual Review of Psychology. Volume 55. Number 1. 401–430 Pages.
- Walker, E., and Tessner, K.
(2008).
"Schizophrenia." Perspectives on Psychological Science. Volume 3. Number 1. 30–37 Pages.
- Suddath, R. L., Christison, G. W., Torrey,
E. F., Casanova, M. F., and Weinberger, D. R.
(1990).
"Anatomical abnormalities in the brains of monozygotic twins
discordant for schizophrenia." New England Journal of Medicine. Volume
322. Number 12. 789–794 Pages.
- Galderisi, S., Quarantelli, M., Volper,
U., Mucci, A., Cassano, G. B., Invernizzi, G., et al.
(2008).
"Patterns of structural MRI abnormalities in deficit and nondeficit
schizophrenia." Schizophrenia Bulletin. Volume 34. Number 2. 393–401
Pages.
- Javitt, D. C., and Laruelle, M.
(2006).
Textbook of Schizophrenia. Chapter
Neurochemical theories. American Psychiatric Publishing. Washington, DC.
85–116 Pages. J. A. Lieberman, T. S. Stroup, and D. O. Perkins (Eds.).
- Inayama, Y., Yoneda, H., Sakai, T., Ishida,
T., Nonomura, Y., Kono, Y., et al.
(1996).
"Positive association between a DNA sequence variant in the
serotonin 2A receptor gene and schizophrenia." American Journal of
Medical Genetics. Volume 67. Number 1. 103–105 Pages.
- Csernansky, J. G., and Grace, A. A.
(1998).
"New models of the pathophysiology of schizophrenia: Editors’
introduction." Schizophrenia Bulletin. Volume 24. Number 2. 185–187
Pages.
- Gottesman, I. I., and Erlenmeyer-Kimling,
L.
(2001).
"Family and twin studies as a head start in defining prodomes and
endophenotypes for hypothetical early interventions in schizophrenia."
Schizophrenia Research. Volume 5. Number 1. 93–102 Pages.
- Riley, B. P., and Kendler, K. S.
(2005).
Kaplan and Sadock’s Comprehensive Textbook of Psychiatry.
Chapter Schizophrenia: Genetics. Lippincott Williams and Wilkins.
Philadelphia. 1354–1370 Pages. B. J. Sadock and V. A. Sadock(Eds.).
- Brown, A. S., Begg, M. D., Gravenstein, S.,
Schaefer, C. S., Wyatt, R. J., Bresnahan, M., et al.
(2004).
"Serologic evidence of prenatal influenza in the etiology of
schizophrenia." Archives of General Psychiatry. Volume 61. Number 8.
774–780 Pages.
- Murray, R. M., and Bramon, E.
(2005).
Kaplan and Sadock’s Comprehensive Textbook of Psychiatry.
Chapter Developmental model of schizophrenia. Lippincott Williams and
Wilkins. Philadelphia. 1381–1395 Pages. B. J. Sadock and V. A.
Sadock(Eds.).
- Susser, E. B., Neugebauer, R., Hock, H.W.,
Brown, A. S., Lin, S., Labowitz, D., and Gorman, J. M.
(1996).
"Schizophrenia after prenatal famine: Further evidence." Archives
of General Psychiatry. Volume 53. Number 1. 25–31 Pages.
- Waddington J. L., Lane, A., Larkin, C.,
and O’Callaghan, E.
(1999).
"The neurodevelopmental basis of schizophrenia: Clinical clues from
cerebro-craniofacial dysmorphogenesis, and the roots of a lifetime
trajectory of disease." Biological Psychiatry. Volume 46. Number 1. 1–9
Pages.
- Walker, E., Mittal, V., and Tessner, K.
(2008).
"Stress and the hypothalamic pituitary adrenal axis in the
developmental course of schizophrenia." Annual Review of Clinical
Psychology. Volume 4. Number 1. 189–216 Pages.
To this point in the unit we have considered the psychological disorders
that fall on Axis I of the Diagnostic and Statistical Manual
of Mental Disorders (DSM) categorization
system. In comparison to the Axis I disorders, which may frequently be severe
and dysfunctional and are often brought on by stress, the disorders that fall
on Axis II are longer-term disorders that are less likely to be severely
incapacitating.
Axis II consists primarily of personality disorders. A personality disorder is a disorder characterized by
inflexible patterns of thinking, feeling, or relating to others that cause problems in
personal, social, and work situations. Personality disorders tend to emerge during
late childhood or adolescence and usually continue throughout adulthood. [1] The disorders can be problematic for
the people who have them, but they are less likely to bring people to a therapist for
treatment than are Axis I disorders.
The personality disorders are summarized in the table below. They are
categorized into three types: those characterized by odd or
eccentric behavior, those characterized by dramatic
or erratic behavior, and those characterized by anxious or inhibited behavior. As you consider the personality types
described in the table, I’m sure you’ll think of people that you know who have
each of these traits, at least to some degree. Probably you know someone who
seems a bit suspicious and paranoid, who feels that other people are always
“ganging up on him,” and who really doesn’t trust other people very much.
Perhaps you know someone who fits the bill of being overly dramatic—the “drama
queen” who is always raising a stir and whose emotions seem to turn everything
into a big deal. Or you might have a friend who is overly dependent on others
and can’t seem to get a life of her own.
Descriptions of the Personality Disorders (Axis II)
") From Flat World Knowledge, Introduction to Psychology, v1.0. Source: American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.). Washington, DC: Author.
From Flat World Knowledge, Introduction to Psychology, v1.0. Source: American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.). Washington, DC: Author.
The personality traits that make up the personality disorders are common—we see
them in the people whom we interact with every day—yet they may become
problematic when they are rigid, overused, or interfere with everyday
behavior. [2] What is perhaps
common to all the disorders is the person’s inability to accurately understand
and be sensitive to the motives and needs of the people around them.
The personality disorders create a bit of a problem for diagnosis. For one, it
is frequently difficult for the clinician to accurately diagnose which of the
many personality disorders a person has, although the friends and colleagues of
the person can generally do a good job of
it. [3] And the personality
disorders are highly comorbid; if a person has one, it’s likely that he or she
has others as well. Also, the number of people with personality disorders is
estimated to be as high as 15% of the
population, [4] which might make us
wonder if these are really “disorders” in any real sense of the word.
Although they are considered as separate disorders, the personality disorders
are seem like milder versions of more severe Axis I
disorders. [5] For example, obsessive-compulsive personality disorder has similar
symptoms to obsessive-compulsive disorder (OCD), and schizoid and schizotypal personality disorders are characterized by
symptoms similar to those of schizophrenia. This overlap in classification
causes some confusion, and some theorists have argued that the personality
disorders should be eliminated from the DSM. But
clinicians normally differentiate Axis I and Axis II disorders, and thus the
distinction is useful for
them. [6] [7] [8]
focus primarily on harm to others.
learn by doing
Assume that the people you are about to read about have received full diagnostic
assessments by a psychologist and have a personality disorder. For each individual,
determine which type of personality disorder he or she most likely has.
Although it is not possible to consider the characteristics of each of the personality
disorders in this book, let’s focus on two that have important implications for behavior.
The first, borderline personality disorder (BPD), is important
because it is so often associated with suicide, and the second, antisocial personality disorder (APD), because it is the foundation of criminal
behavior. Borderline and antisocial personality disorders are also good examples to
consider because they are so clearly differentiated in terms of their focus. BPD (more
frequently found in women than men) is known as an internalizing
disorder because the behaviors that it entails (e.g., suicide and self-mutilation)
are mostly directed toward the self. APD (mostly found in men), on the other hand, is a
type of externalizing disorder in which the problem behaviors
(e.g., lying, fighting, vandalism, and other criminal activity)
References
- Widiger, T. A.
(2006).
Rorschach Assessment to the Personality Disorders. The LEA Series in Personality and Clinical Psychology. Chapter Understanding personality disorders. Lawrence Erlbaum Associates. Mahwah, NJ. 3–25 Pages. S. K. Huprich (Ed.).
- Lynam, D., and Widiger, T.
(2001).
"Using the five-factor model to represent the DSM-IV personality
disorders: An expert consensus approach." Journal of Abnormal
Psychology. Volume 110. Number 3. 401–412 Pages.
- Oltmanns, T. F., and Turkheimer, E.
(2006).
Personality and Psychopathology. Chapter
Perceptions of self and others regarding pathological personality
traits. Guilford Press. New York. 71–111 Pages. R. F. Krueger and J. L.
Tackett (Eds.).
- Grant, B., Hasin, D., Stinson, F., Dawson, D.,
Chou, S., Ruan, W., and Pickering, R. P.
(2004).
"Prevalence, correlates, and disability of personality disorders in
the United States: Results from the national epidemiologic survey on
alcohol and related conditions." Journal of Clinical Psychiatry. Volume
65. Number 7. 948–958 Pages.
- Huang, Y., Kotov, R., de Girolamo, G., Preti,
A., Angermeyer, M., Benjet, C., et al.
(2009).
"SM-IV personality disorders in the WHO World Mental Health
Surveys." British Journal of Psychiatry. Volume 195. Number 1. 46–53
Pages.
- Krueger, R. F.
(2005).
"Continuity of Axes I and II: Toward a unified model of
personality, personality disorders, and clinical disorders." Journal of
Personality Disorders. Volume 19. Number 3. 233–261 Pages.
- Phillips, K. A., Yen, S., and Gunderson, J. G.
(2003).
Textbook of Clinical Psychiatry. Chapter Personality disorders. American Psychiatric Publishing. Washington, DC. R. E. Hales and S. C. Yudofsky (Eds.).
- Verheul, R.
(2005).
"Clinical utility for dimensional models of personality pathology."
Journal of Personality Disorders. Volume 19. Number 3. 283–302 Pages.
Borderline personality disorder (BPD) is a
psychological disorder characterized by a prolonged disturbance of personality
accompanied by mood swings, unstable personal relationships, identity problems, threats
of self-destructive behavior, fears of abandonment, and impulsivity. BPD is widely
diagnosed—up to 20% of psychiatric patients are given the diagnosis, and it may occur in up
to 2% of the general population. [1] About
three-quarters of diagnosed cases of BPD are women.
People with BPD fear being abandoned by others. They often show a clinging
dependency on the other person and engage in manipulation to try to maintain
the relationship. They become angry if the other person limits the
relationship, but also deny that they care about the person. As a defense
against fear of abandonment, borderline people are compulsively social. But
their behaviors, including their intense anger, demands, and suspiciousness,
repel people.
People with BPD often deal with stress by engaging in self-destructive
behaviors, for instance by being sexually promiscuous, getting into fights,
binge eating and purging, engaging in self-mutilation or drug abuse, and
threatening suicide. These behaviors are designed to call forth a “saving”
response from the other person. People with BPD are a continuing burden for
police, hospitals, and therapists. Borderline individuals also show disturbance
in their concepts of identity: They are uncertain about self-image, gender
identity, values, loyalties, and goals. They may have chronic feelings of
emptiness or boredom and be unable to tolerate being alone.
BPD has both genetic as well as environmental roots. In terms of genetics,
research has found that those with BPD frequently have neurotransmitter
imbalances, [2] and the
disorder is
heritable. [3]
In terms of environment, many theories about the causes of BPD focus on a
disturbed early relationship between the child and his or her parents. Some
theories focus on the development of attachment in early childhood, while
others point to parents who fail to provide adequate attention to the child’s
feelings. Others focus on parental abuse (both sexual and physical) in
adolescence, as well as on divorce, alcoholism, and other
stressors. [4] The dangers of BPD are
greater when they are associated with childhood sexual abuse, early age of
onset, substance abuse, and aggressive behaviors. The problems are amplified
when the diagnosis is comorbid (as it often is) with other disorders, such as
substance abuse disorder, major depressive disorder, and posttraumatic stress
disorder (PTSD). [5]
Research Focus: Affective and Cognitive Deficits in BPD
Posner and colleagues [6] hypothesized that the difficulty that
individuals with BPD have in regulating their lives (e.g., in developing
meaningful relationships with other people) may be due to imbalances in
the fast and slow emotional pathways in the brain. Specifically, they
hypothesized that the fast emotional pathway through the amygdala is too
active, and the slow cognitive-emotional pathway through the prefrontal
cortex is not active enough in those with BPD.
The participants in their research were 16 patients with BPD and 14
healthy comparison participants. All participants were tested in a
functional magnetic resonance imaging (fMRI) machine while they performed
a task that required them to read emotional and nonemotional words, and
then press a button as quickly as possible whenever a word appeared in a
normal font and not press the button whenever the word appeared in an
italicized font. The researchers found that while all participants
performed the task well, the patients with BPD had more errors than the
controls (both in terms of pressing the button when they should not have
and not pressing it when they should have). These errors primarily
occurred on the negative emotional words.
The figure below shows the comparison of the level of brain activity in
the emotional centers in the amygdala (left panel) and the prefrontal
cortex (right panel). In comparison to the controls, the borderline
patients showed relatively larger affective responses when they were
attempting to quickly respond to the negative emotions, and showed less
cognitive activity in the prefrontal cortex in the same conditions. This
research suggests that excessive affective reactions and lessened
cognitive reactions to emotional stimuli may contribute to the emotional
and behavioral volatility of borderline patients.
References
- Hyman, S. E.
(2002).
"A new beginning for research on borderline personality disorder."
Biological Psychiatry. Volume 51. Number 12. 933–935 Pages.
- Zweig-Frank, H., Paris, J., Kin, N. M.
N. Y., Schwartz, G., Steiger, H., and Nair, N. P. V.
(2006).
"Childhood sexual abuse in relation to neurobiological challenge
tests in patients with borderline personality disorder and normal
controls." Psychiatry Research. Volume 141. Number 3. 337–341 Pages.
- Minzenberg, M. J., Poole, J. H., and
Vinogradov, S.
(2008).
"A neurocognitive model of borderline personality disorder: Effects
of childhood sexual abuse and relationship to adult social attachment
disturbance." Development and Psychological Disorder. Volume 20. Number
1. 341–368 Pages.
- Lobbestael, J., and Arntz, A.
(2009).
"Emotional, cognitive and physiological correlates of abuse-related
stress in borderline and antisocial personality disorder." Behaviour
Research and Therapy. Volume 48. Number 2. 116–124 Pages.
- Skodol, A. E., Gunderson, J. G., Pfohl, B.,
Widiger, T. A., Livesley, W. J., and Siever, L. J.
(2002).
"The borderline diagnosis I: Psychopathology, comorbidity, and
personality structure." Biological Psychiatry. Volume 51. Number 12.
936–950 Pages.
- Posner, M., Rothbart, M., Vizueta, N.,
Thomas, K., Levy, K., Fossella, J., et al.
(2003).
"An approach to the psychobiology of personality disorders."
Development and Psychopathology. Volume 15. Number 4. 1093–1106 Pages.
In contrast to borderline personality disorder, which involves primarily feelings of
inadequacy and a fear of abandonment, antisocial personality disorder
(APD) is characterized by a disregard of the rights of others, and a tendency
to violate those rights without being concerned about doing so.
APD is a pervasive pattern of violation of the rights of others that
begins in childhood or early adolescence and continues into adulthood. APD is
about three times more likely to be diagnosed in men than in women. To be diagnosed with
APD the person must be 18 years of age or older and have a documented history of conduct
disorder before the age of 15. Many years ago, people having antisocial personality
disorder were referred to as “sociopaths” or “psychopaths,” but these terms are no
longer interchangeable. The disorder “psychopathy” is not in the DSM, but is a distinct
personality disorder characterized by lack of remorse and deficits in empathy.
People with APD feel little distress for the pain they cause others. They lie, engage in
violence against animals and people, and frequently have drug and alcohol abuse
problems. They are egocentric and frequently impulsive, for instance suddenly changing
jobs or relationships. People with APD soon end up with a criminal record and often
spend time incarcerated. The intensity of antisocial symptoms tends to peak during the
20s and then may decrease over time.
Biological and environmental factors are both implicated in the development of antisocial
personality disorder. Twin and adoption studies suggest
a genetic predisposition, [1] and biological abnormalities
include low autonomic activity during stress, biochemical imbalances, right hemisphere
abnormalities, and reduced gray matter in the frontal lobes. [2] [3] Environmental factors include
neglectful and abusive parenting styles, such as the use of harsh and inconsistent
discipline and inappropriate modeling. [4]
References
- Rhee, S. H., and Waldman, I. D.
(2002).
"Genetic and environmental influences on anti-social behavior: A
meta-analysis of twin and adoptions studies." Psychological Bulletin.
Volume 128. Number 3. 490–529 Pages.
- Lyons-Ruth, K., Holmes, B. M.,
Sasvari-Szekely, M., Ronai, Z., Nemoda, Z., and Pauls, D.
(2007).
"Serotonin transporter polymorphism and borderline or antisocial
traits among low-income young adults." Psychiatric Genetics. Volume 17.
Number 6. 339–343 Pages.
- Raine, A., Lencz, T., Bihrle, S., LaCasse,
L., and Colletti, P.
(2000).
"Reduced prefrontal gray matter volume and reduced autonomic
activity in antisocial personality disorder." Archive of General
Psychiatry. Volume 57. Number 2. 119–127 Pages.
- Huesmann, L. R., and Kirwil, L.
(2007).
The Cambridge Handbook of Violent Behavior and Aggression.
Chapter Why observing violence increases the risk of violent behavior
by the observer. Cambridge University Press. New York. 545–570 Pages. D.
J. Flannery, A. T. Vazsonyi, and I. D. Waldman (Eds.).
The disorders presented next are categorized in the DSM-IV as “Disorders Usually First
Diagnosed in Infancy, Childhood, or Adolescence.” The key word here is usually—adults can be diagnosed with these disorders, but most often, they are
diagnosed for the first time when the individual is a child. These disorders, such as ADHD
and Autistic Disorder, are categorized together because of the timing of first diagnosis
rather than similarity of their symptoms. [1] Although these disorders are often
thought of as being the primary mental illnesses faced by children, it is important to note
that children can—and do—also experience the other disorders you have read about, including
anxiety and mood disorders.
Zack, age 7 years, has always had trouble settling down. He is easily bored and
distracted. In school, he cannot stay in his seat for very long, and he frequently does
not follow instructions. He is constantly fidgeting or staring into space. Zack has poor
social skills and may overreact when someone accidentally bumps into him or uses one of
his toys. At home, he chatters constantly and rarely settles down to do a quiet
activity, such as reading a book.
Symptoms such as Zack’s are common among 7-year-olds, and particularly among
boys. But what do the symptoms mean? Does Zack simply have a lot of energy and
a short attention span? Boys mature more slowly than girls at this age, and
perhaps Zack will catch up in the next few years. One possibility is for the
parents and teachers to work with Zack to help him be more attentive, to put up
with the behavior, and to wait it out.
But many parents, often on the advice of the child’s teacher, take their children to a
psychologist for diagnosis. If Zack were taken for testing today, it is likely that he
would be diagnosed with a psychological disorder known as attention-deficit hyperactivity disorder (ADHD). ADHD is a
developmental behavior disorder characterized by problems with focus, difficulty
maintaining attention, and inability to concentrate, in which symptoms start before 7
years of age. [1] [2]
Although it is usually first diagnosed in childhood, ADHD can remain problematic in adults,
and up to 7% of college students are diagnosed with it. [3] In adults, the symptoms of ADHD include
forgetfulness, difficulty paying attention to details, procrastination, disorganized work
habits, and not listening to others.
ADHD is about 70% more likely to occur in males than in females [4] and is often comorbid with
other behavioral and conduct disorders. The diagnosis of ADHD has quadrupled over the past
20 years such that it is now diagnosed in about 1 out of every 20 American children and is
the most common psychological disorder among children in the world. [5] ADHD is
also being diagnosed much more frequently in adolescents and adults. [6] You might wonder what this all means.
Are the increases in the diagnosis of ADHD due to the fact that today’s children and
adolescents are actually more distracted and hyperactive than their parents were, due to a
greater awareness of ADHD among teachers and parents, or are psychologists and
psychiatrists overdiagnosing the problem? Some believe that drug companies contribute to
the rate of diagnosis of the disorder, because ADHD is often treated with prescription
medications, including stimulants such as Ritalin.
Despite these arguments by skeptics, research suggests that ADHD is a real disorder that is
caused by a combination of genetic and environmental factors. Twin studies have found that
ADHD is heritable, [2] and neuroimaging studies have
found that people with ADHD may have structural differences in areas of the brain that
influence self-control and attention. [7] Other studies have pointed to
environmental factors, such as mothers’ smoking and drinking alcohol during pregnancy and
the consumption of lead and food additives by those who are affected. [8] [9] [10]
Social factors, such as family stress and poverty, also contribute to ADHD. [11]
References
- American Psychiatric Association
(2000).
Diagnostic and Statistical Manual of Mental Disorders. Author. Washington, DC. Edition 4, text rev.
- National Institute of Mental Health.
(2010).
Attention-deficit hyperactivity disorder (ADHD). Retrieved from http://www.nimh.nih.gov/health/topics/attention-deficit-hyperactivity-disorder-adhd/index.shtml.
- Weyandt, L. L., and DuPaul, G.
(2006).
"ADHD in college students." Journal of Attention Disorders. Volume 10. Number 1. 9–19 Pages.
- Kessler, R. C., Chiu, W. T., Demler, O., and
Walters, E. E.
(2005).
"Prevalence, severity, and comorbidity of 12-month DSM-IV disorders
in the National Comorbidity Survey Replication." Archives of General
Psychiatry. Volume 62. Number 6. 617–627 Pages.
- Olfson, M., Gameroff, M., Marcus, S., and
Jensen, P.
(2003).
"National trends in the treatment of attention deficit
hyperactivity disorder." American Journal of Psychiatry. Volume 160.
Number 6. 1071–1077 Pages.
- Barkley, R. A.
(1998).
Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and
Treatment. Guilford Press. New York.
- Seidman, L., Valera, E., and Makris, N.
(2005).
"Structural brain imaging of attention deficit/hyperactivity
disorder." Biological Psychiatry. Volume 57. Number 11. 1263–1272 Pages.
- Braun, J., Kahn, R., Froehlich, T., Auinger,
P., and Lanphear, B.
(2006).
"Exposures to environmental toxicants and
attention-deficit/hyperactivity disorder in U.S. children."
Environmental Health Perspectives. Volume 114. Number 12. 1904–1909
Pages.
- Linnet, K., Dalsgaard, S., Obel, C., Wisborg,
K., Henriksen T., Rodriguez, A et al.
(2003).
"Maternal lifestyle factors in pregnancy risk of
attention-deficit/hyperactivity disorder and associated behaviors:
Review of the current evidence." American Journal of Psychiatry. Volume
160. Number 6. 1028–1040 Pages.
- McCann, D., Barrett, A., Cooper, A.,
Crumpler, D., Dalen, L., Grimshaw, K., et al.
(2007).
"Food additives and hyperactive behaviour in 3-year-old and
8/9-year-old children in the community: A randomised, double-blinded,
placebo-controlled trial." Lancet. Volume 370. Number 9598. 1560–1567
Pages.
- Burt, S. A., Krueger, R. F., McGue, M., and
Iacono, W. G.
(2001).
"Sources of covariation among attention-deficit/hyperactivity
disorder, oppositional defiant disorder, and conduct disorder: The
importance of shared environment." Journal of Abnormal Psychology.
Volume 110. Number 4. 516–525 Pages.
Jared’s kindergarten teacher has voiced her concern to Jared’s parents about
his difficulties with interacting with other children and his delay in
developing normal language. Jared is able to maintain eye contact and enjoys
mixing with other children, but he cannot communicate with them very well.
He often responds to questions or comments with long-winded speeches about
trucks or some other topic that interests him, and he seems to lack
awareness of other children’s wishes and needs.
Jared’s concerned parents took him to a multidisciplinary child development
center for consultation. Here he was tested by a pediatric neurologist, a
psychologist, and a child psychiatrist. The pediatric neurologist found that
Jared’s hearing was normal, and there were no signs of any neurological
disorder. He diagnosed Jared with a pervasive developmental
disorder, because while his comprehension and expressive language was
poor, he was still able to carry out nonverbal tasks, such as drawing a picture
or doing a puzzle.
Based on her observation of Jared’s difficulty interacting with his peers, and the fact
that he did not respond warmly to his parents, the psychologist diagnosed Jared with autistic disorder (autism), a disorder of neural
development characterized by impaired social interaction and communication and by
restricted and repetitive behavior, and in which symptoms begin before 7 years of
age. The psychologist believed that the autism diagnosis was correct because, like
other children with autism, Jared has a poorly developed ability to see the world from the
perspective of others; engages in unusual behaviors such as talking about trucks for hours;
and responds to stimuli, such as the sound of a car or an airplane, in unusual ways.
The child psychiatrist believed that Jared’s language problems and social skills were not
severe enough to warrant a diagnosis of autistic disorder and instead proposed a diagnosis
of Asperger’s disorder, a developmental disorder
that affects a child’s ability to socialize and communicate effectively with others and
in which symptoms begin before 7 years of age. The symptoms of Asperger’s are
almost identical to those of autism (with the exception of a delay in language
development), and the child psychiatrist simply saw these problems as less extreme.
Imagine how Jared’s parents must have felt at this point. Clearly there is
something wrong with their child, but even the experts cannot agree on exactly
what the problem is. Diagnosing problems such as Jared’s is difficult, yet the
number of children like him is increasing dramatically. Disorders related to
autism and Asperger’s disorder now affect almost 1% of American
children. [1] The milder forms of autism, and
particularly Asperger’s, have accounted for most of this increase in
diagnosis.
Although for many years autism was thought to be primarily a socially determined disorder,
in which parents who were cold, distant, and rejecting created the problem, current
research suggests that biological factors are most important. The heritability of autism
has been estimated to be as high as 90%. [2] Scientists speculate that autism is caused by an unknown,
genetically determined brain abnormality that occurs early in development. It is likely
that several different brain sites are affected, [3] and the search for these areas is being conducted in many
scientific laboratories.
But does Jared have autism or Asperger’s? The problem is that diagnosis is not exact
(remember the idea of “categories”), and the experts themselves are often unsure how to
classify behavior. Furthermore, the appropriate classifications change with time and new
knowledge. The American Psychiatric Association has recently posted on its website a
proposal to eliminate the term Asperger’s syndrome from the
upcoming DSM-V. Whether or not Asperger’s will remain a separate
disorder will be made known when the next DSM-V is published in
2013.
learn by doing
For each of the following children, specify which disorder he or she most
likely has.
References
- Kogan, M., Blumberg, S., Schieve, L., Boyle, C.,
Perrin, J., Ghandour, R., et al.
(2009).
"Prevalence of parent-reported diagnosis of autism spectrum
disorder among children in the US, 2007." Pediatrics. Volume 124. Number
5. 1395–1403 Pages.
- Freitag C. M.
(2007).
"The genetics of autistic disorders and its clinical relevance: A
review of the literature." PediaMolecular Psychiatrytrics. Volume 12.
Number 1. 2–22 Pages.
- Moldin, S. O.
(2003).
"Editorial: Neurobiology of autism: The new frontier." Genes, Brain and Behavior. Volume 2. Number 5. 253–254 Pages.
In the last module on childhood disorders, we discussed that identifying and clearly
describing psychological disorders is not simple task. The same kind of challenge exists in
the medical world for clearly identifying and describing diseases and disorders of other
parts of the body.
In this module, you learn about a dramatic and controversial disorder called dissociative
identity disorder. It is a rare condition that has captured the imagination of writers,
movie makers, and the general public. The clinical community has engaged in fierce debates
for decades about the causes and characteristics of dissociative identity disorder, with
many psychologists arguing that the disorder is not real.
First, we describe the disorder using terminology from the DSM.
Then we explain some of the concerns that people have raised that have led to doubts about
the validity of the diagnosis and interpretation of the patients' behaviors. Finally, we
review some of the research that has been conducted to answer the questions using the tools
of science.
You may remember the story of Sybil (a pseudonym for Shirley Ardell
Mason, who was born in 1923), a person who, over a period of 40 years, claimed to possess
16 distinct personalities. Mason was in therapy for many years trying to integrate these
personalities into one complete self. A TV movie about Mason’s life, starring Sally Field
as Sybil, appeared in 1976.
Sybil suffered from the most severe of the dissociative disorders, dissociative identity disorder. Dissociative identity
disorder is a psychological disorder in which two or more
distinct and individual personalities exist in the same person, and there is an extreme
memory disruption regarding personal information about the other
personalities. [1] Dissociative identity disorder was once
known as multiple personality disorder, and this label is still sometimes used. This
disorder is sometimes mistakenly referred to as schizophrenia.
Reports of cases of dissociative identity disorder suggest that there can be more than 10
different personalities in one individual. Switches from one personality to another tend to
occur suddenly, often triggered by a stressful situation. [2] The host personality is the
personality in control of the body most of the time, and the alter
personalities tend to differ from each other in terms of age, race, gender,
language, manners, and even sexual orientation. [3] A shy, introverted individual may develop a boisterous,
extroverted alter personality. Each personality has unique memories and social
relationships. [4] Women are more frequently diagnosed with
dissociative identity disorder than are men, and when they are diagnosed also tend to have
more “personalities.” [5]
Although this disorder has received a lot of attention by the media and general public, it
is arguably the most controversial disorder in the DSM. In fact,
clinicians and researchers disagree about the legitimacy of dissociative identity disorder.
Some clinicians argue that the descriptions in the DSM accurately
reflect the symptoms of these patients, whereas others believe that patients are faking,
role-playing, or using the disorder as a way to justify behavior. [6] [7] [8] [9]
Some have hypothesized that patients who are distressed and highly suggestible
can be influenced by therapists to exhibit symptoms of the
disorder. [8] Even the diagnosis of
Shirley Ardell Mason (Sybil) is disputed. Some experts claim that Mason was
highly hypnotizable and that her therapist unintentionally “suggested” the
existence of her multiple personalities. [10]
Using Science to Resolve Controversies
How can we determine the legitimacy of dissociative identity disorder? Because psychology
is a science, careful research is the best method to resolve such controversies. Lilienfeld
and Lynn [8] review some studies that have done
just this. For example, Modestin [11]
conducted a survey in Switzerland that that revealed that two-thirds of cases
of dissociative identity disorder were diagnosed by just .09% of clinicians. Ninety percent
of clinicians reported never having seen a patient with dissociative identity disorder.
This suggests that some clinicians diagnose many people with dissociative identity
disorder, and other clinicians never diagnose anyone with the disorder. Future research is
needed to determine whether the clinicians who are diagnosing many cases of dissociative
identity disorder are simply better at identifying the disorder or if they are giving the
diagnosis too frequently.
Laboratory experiments provide a different kind of evidence regarding dissociative identity
disorder. For example, Spanos, Weekes, and Bertrand [12] (see also Lilienfeld and Lynn,
2003 [8] ) conducted an experiment in which participants were
asked to role-play the part of a murderer and be interviewed by a psychiatrist. Some
participants were randomly assigned to receive an interview involving hypnosis during which
it was suggested they had elements of dissociative identity disorder. For example, they
were told by the interviewer, “I've talked a bit to [name], but I think perhaps there might
be another part of [name] that I haven't talked to, another part that maybe feels somewhat
differently from the part that I've talked to. And I would like to communicate with that
other part.” The control group of participants received no suggestion of this kind. Many of
the participants who received the suggestion that they may have another personality adopted
a different name for this “alter” personality and even referred to him or her in the third
person. None of the control participants did this. By no means does this “prove” that
dissociative identity disorder can be created in the laboratory, but it does provide
evidence that people can show signs consistent with this disorder under the right
conditions (e.g., a suggestive interview). Studies like this and other types of research
can advance knowledge on how disorders develop so that diagnostic controversies can be
cleared up.
References
- van der Hart, O., and Nijenhuis, E. R. S.
(2009).
Oxford Textbook of Psychological Disorder.
Chapter Dissociative disorders. Oxford University Press. New York.
Edition 2. 452–481 Pages. P. H. Blaney, and T. M. Millon (Eds.).
- Gillig, P. M.
(2009).
"Dissociative identity disorder: A controversial diagnosis." Psychiatry. Volume 6. Number 3. 24–29 Pages.
- Kluft, R. P.
(2009).
The Hatherleigh Guide to Psychiatric Disorders, Vol. 1. Chapter The diagnosis and treatment of dissociative identity disorder. Hatherleigh Press. New York. Edition 2. 49–96 Pages.
- Dawson, P. L.
(1990).
"Understanding and cooperation among alter and host personalities."
American Journal of Occupational Therapy. Volume 44. Number 11. 994–997
Pages.
- American Psychiatric Association
(2000).
Diagnostic and Statistical Manual of Mental Disorders. Author. Washington, DC. Edition 4, text rev.
- Barry-Walsh, J.
(2005).
"Dissociative identity disorder." Australian and New Zealand
Journal of Psychiatry. Volume 39. Number 1–2. 109–110 Pages.
- Kihlstrom, J. F.
(2004).
"An unbalanced balancing act: Blocked, recovered, and false
memories in the laboratory and clinic." Clinical Psychology: Science and
Practice. Volume 11. Number 1. 34–41 Pages.
- Lilienfeld, S. O., and Lynn, S. J.
(2003).
Science and Pseudoscience in Clinical Psychology.
Chapter Dissociative identity disorder: Multiple personalities,
multiple controversies. Guilford Press. New York. 109–142 Pages. S. O.
Lilienfeld, S. J. Lynn, and J. M. Lohr (Eds.).
- Lipsanen, T., Korkeila, J., Peltola, P.,
Jarvinen, J., Langen, K., and Lauerma, H.
(2004).
"Dissociative disorders among psychiatric patients: Comparison with
a nonclinical sample." European Psychiatry. Volume 19. Number 1. 53–55
Pages.
- Miller, M., and Kantrowitz, B.
(1999, January 25).
"Unmasking Sybil: A reexamination of the most famous psychiatric patient in history." Newsweek. 11–16 Pages.
- Modestin, J.
(1992).
"Multiple personality disorder in Switzerland." American Journal of Psychiatry. Volume 149. Number 1. 88–92 Pages.
- Spanos, N. P., Weekes, J. R., and Bertrand,
L. D.
(1985).
"Multiple personality: A social psychological perspective." Journal
of Abnormal Psychology. Volume 94. Number 3. 362–376 Pages.
Therapy on Four Legs?
Lucien Masson, a 60-year-old Vietnam veteran from Arizona, put it simply: “Sascha is
the best medicine I’ve ever had.”
Lucien is speaking about his friend, companion, and perhaps even his therapist, a
Russian wolfhound named Sascha. Lucien suffers from posttraumatic stress disorder
(PTSD), a disorder that has had a profoundly negative impact on his life for many
years. His symptoms include panic attacks, nightmares, and road rage. Lucien has
tried many solutions, consulting with doctors, psychiatrists, and psychologists and
using a combination of drugs, group therapy, and anger-management classes.
But Sascha seems to be the best therapist of all. He helps out in many ways. If a
stranger gets too close to Lucien in public, Sascha will block the stranger with his
body. Sascha is trained to sense when Lucien is about to have a nightmare, waking
him before it starts. Before road rage can set in, Sascha gently whimpers, reminding
his owner that it doesn’t pay to get upset about nutty drivers.
In the same way, former Army medic Jo Hanna Schaffer speaks of her Chihuahua, Cody:
“I never took a pill for PTSD that did as much for me as Cody has done.”
Persian Gulf War veteran Karen Alexander feels the same way about her Bernese
mountain dog, Cindy: “She’ll come up and touch me, and that is enough of a stimulus
to break the loop, bring me back to reality. Sometimes I’ll scratch my hand until
it’s raw and won’t realize until she comes up to me and brings me out. She’s such a
grounding influence for me.”
 Can psychiatric therapy dogs help people who suffer from PTSD? From Flat
World Knowledge, Introduction to Psychology, v1.0. ©
Thinkstock.
Can psychiatric therapy dogs help people who suffer from PTSD? From Flat
World Knowledge, Introduction to Psychology, v1.0. ©
Thinkstock.
These dramatic stories of improvement from debilitating disorders can be attributed to an
alternative psychological therapy, based on established behavioral principles, provided
by “psychiatric service dogs.” The dogs are trained to help people with a variety of
mental disorders, including panic attacks, anxiety disorder, obsessive-compulsive
disorder, and bipolar disorder. They help veterans of Iraq and Afghanistan cope with
their traumatic brain injuries as well as with PTSD.
The dogs are trained to perform specific behaviors that are helpful to their owners. If
the dog’s owner is depressed, the dog will snuggle up and offer physical comfort; if the
owner is having a panic attack, the owner can calm himself by massaging the dog’s body.
The serenity shown by the dogs in all situations seems to reassure the PTSD sufferer
that all must be well. Service dogs are constant, loving companions who provide
emotional support and companionship to their embattled, often isolated owners. [1] [2] [3] [4]
Despite the reports of success from many users, it is important to keep in mind that the
utility of psychiatric service dogs has not yet been tested empirically to review
long-term benefits. Organizations such as Pet for Vets, however, help pair shelter dogs
with vets who are emotionally wounded. Watch this video for more inspiring stories about how dogs help veterans
cope with PTSD.
Psychological disorders create a tremendous individual, social, and economic drain on
society. Disorders make it difficult for people to engage in productive lives and
effectively contribute to their family and to society. Disorders lead to disability and
absenteeism in the workplace as well as to physical problems, premature death, and
suicide. At a societal level, the costs are staggering. It has been estimated that the
annual financial burden of each case of anxiety disorder is over $3,000 per year,
meaning that the annual cost of anxiety disorders alone in the United States runs into
the trillions of dollars. [5] [6]
The goal of this unit is to review the techniques that are used to treat psychological
disorder. Just as psychologists consider the causes of disorder in terms of the
bio-psycho-social model of illness, treatment is also based on psychological,
biological, and social approaches.
- The psychological approach to reducing disorder involves
providing help to individuals or families through psychological therapy, including
psychoanalysis, humanistic-oriented
therapy, cognitive-behavioral therapy (CBT), and
other approaches.
- The biomedical approach to reducing disorder is based on the
use of medications to treat mental disorders such as schizophrenia, depression, and
anxiety, as well as the employment of brain intervention techniques, including electroconvulsive therapy (ECT), transcranial magnetic stimulation (TMS), and psychosurgery.
- The social approach to reducing disorder focuses on changing
the social environment in which individuals live to reduce the underlying causes of
disorder. These approaches include group, couples, and family
therapy, as well as community outreach programs.
The community approach is likely to be the most effective of the three approaches
for reaching large groups of people because it focuses not only on treatment, but on
education about disorders and prevention of their occurrence in the first
place. [7]
learn by doing
Janice has been seriously depressed lately. A close friend finally persuaded her
to get professional help. She discovers that there are many different approaches
to treating psychological problems, but she isn’t sure what is best for her
condition. She decides to interview several potential therapists to see what
each one of them can tell her about the approach she might expect from that
psychologist.
In this exercise, you will listen in on just a few seconds of each of Janice’s
interviews. Based entirely on the information you hear, decide if the therapist
is suggesting a psychological approach to treatment, a biological approach to
treatment, or a social approach to treatment.
A clinician may focus on any or all of the three approaches to treatment, but in making a
decision about which to use, he or she will always rely on his or her knowledge about
existing empirical tests of the effectiveness of different treatments. These tests,
known as outcome studies, carefully compare people who receive a
given treatment with people who do not receive a treatment, or with people who receive a
different type of treatment. Taken together, these studies have confirmed that many
types of therapies are effective in treating disorder.
Psychotherapy
Treatment for psychological disorder begins when the individual who is
experiencing distress visits a counselor or therapist, perhaps in a church, a
community center, a hospital, or a private practice. The therapist will begin by
systematically learning about the patient’s needs through a formal psychological assessment, which is an
evaluation of the patient’s psychological and mental health. During the
assessment the psychologist may give personality tests such as the Minnesota
Multiphasic Personal Inventory (MMPI-2) or projective tests, and will conduct a
thorough interview with the patient. The therapist may get more information from
family members or school personnel.
In addition to the psychological assessment, the patient is usually seen by a
physician to gain information about potential Axis III (physical) problems. In
some cases of psychological disorder—and particularly for sexual
problems—medical treatment is the preferred course of action. For instance, men
who are experiencing erectile dysfunction disorder may need surgery to increase
blood flow or local injections of muscle relaxants. Or they may be prescribed
medications (Viagra, Cialis, or Levitra) that provide an increased blood supply
to the penis, which are successful in increasing performance in about 70% of men
who take them.
After the medical and psychological assessments are completed, the therapist will
make a formal diagnosis using the detailed descriptions of the disorder provided
in the Diagnostic and Statistical Manual of Mental
Disorders (DSM; see below). The therapist will
summarize the information about the patient on each of the five DSM axes, and the diagnosis will likely be sent to an
insurance company to justify payment for the treatment.
learn by doing
Imagine that you are a school psychologist. You are trying to decide if you
should recommend to a middle school that Mark Wilshire, a 6th grade student,
should receive special consideration in school activities. Mark’s parents have
been interested in his progress and cooperative with school officials, but they
are concerned about him and wonder if he has a learning disability. You suspect
that he may have normal learning abilities, but that he might have a “behavior
disorder” called Attention Deficit Hyperactivity Disorder, usually called by its
initials: ADHD. Here is a report compile about Mark. By law in your state, Mark
has a right to receive specific accommodations, such as a quiet place to take
tests, if he qualifies for an ADHD diagnosis. If he does not, then he will not
receive any special treatment.
Look over the report you have from a psychologist who interviewed Mark. Based on
this information, do you feel that Mark should be given further testing for ADHD
or that there is insufficient evidence of ADHD and other possible reasons for
his problems, such as a learning disability, should be pursued?
Your school requires that a recommendation for ADHD assessment must indicate if
the student qualifies under (A) Inattention type ADHD or (B)
Hyperactivity-Impulsivity type ADHD. Use the symptom charts to decide.
Case Report on Mark Wilshire
Mark is 12-years-old and is of average height and weight for his age. He has come
to the clinic because his parents are concerned about his poor performance at
school. Mark’s teachers report that they like Mark and he is friendly and
respectful, but he is consistently late with assignments, often forgets
regularly scheduled meetings, and frequently fails to follow directions even
when these directions are repeated several times. His work is often incomplete,
sloppy, and poorly edited. He constantly loses things, like books and pens, and
he often “daydreams” during class activities. When other children are being
disruptive, Mark is unable to continue with his work, so he becomes part of the
disruptive group, requiring attention from the teacher.
During the interview, Mark was well behaved. He would frequently squirm in his
chair and fidget, but he was able to control himself enough to remain engaged in
the conversation. He listened carefully to questions and answered appropriately
and with insight. He was distracted several times by noises in the waiting room,
but when his attention was reestablished, he understood questions and answered
them with well thought out explanations. His language was typical of a
12-year-old boy.
Instructions: Please complete the following assessment of
this student by identifying (checking the appropriate boxes) all symptoms that
apply to Mark Wilshire. When you are done, click the Submit button so you can
compare your checklist with the correct one. You many also review feedback
referring to excerpts of the report by clicking on the yellow bubbles.
When you have finished, please assess the other set of symptoms.
Symptom List A: Inactivity Type ADHD
Symptom List B: Hyperactivity-Impulsivity Type ADHD
If a diagnosis is made, the therapist will select a course of therapy that he or she
feels will be most effective. One approach to treatment is psychotherapy, the professional treatment for psychological
disorder through techniques designed to encourage communication of conflicts and
insight. The fundamental aspect of psychotherapy is that the patient directly
confronts the disorder and works with the therapist to help reduce it. Therapy includes
assessing the patient’s issues and problems, planning a course of treatment, setting
goals for change, the treatment itself, and an evaluation of the patient’s progress.
Therapy is practiced by thousands of psychologists and other trained practitioners in
the United States and around the world, and is responsible for billions of dollars of
the health budget.
To many people, therapy involves a patient lying on a couch with a therapist sitting
behind and nodding sagely as the patient speaks. Though this approach to therapy (known
as psychoanalysis) is still practiced, it is in the minority. It
is estimated that there are over 400 different kinds of therapy practiced by people in
many fields, and the most important of these are shown in the figure below. The
therapists who provide these treatments include psychiatrists
and clinical
psychologists, as well as social workers, psychiatric nurses, and couples, marriage, and
family therapists.
References
- Shim, J.
(2008, January 29).
Dogs chase nightmares of war away. CNN. Retrieved from
http://edition.cnn.com/2008/LIVING/personal/01/29/dogs.veterans.
- Lorber, J.
(2010, April 3).
For the battle-scarred, comfort at leash’s end. New York Times. Retrieved from http://www.nytimes.com/2010/04/04/us/04dogs.html.
- Alaimo, C.
(2010, April 11).
Psychiatric service dogs use senses to aid owners. Arizona Daily Star. Retrieved from
http://azstarnet.com/news/local/article_d24b5799-9b31-548c-afec-c0160e45f49c.html.
- Schwartz, A. N.
(2008, March 16).
Psychiatric service dogs, very special dogs, indeed. Dr. Schwartz’s Weblog. Retrieved from
http://www.mentalhelp.net/poc/view_doc.php?type=doc&id=14844.
- Konnopka, A., Leichsenring, F., Leibing, E., and König,
H.-H.
(2009).
"Cost-of-illness studies and cost-effectiveness analyses in anxiety
disorders: A systematic review." Journal of Affective Disorders. Volume 114. Number 1–3. 14–31 Pages.
- Smit, F., Cuijpers, P., Oostenbrink, J., Batelaan, N., de Graaf, R., and
Beekman, A.
(2006).
"Costs of nine common mental disorders: Implications for curative and
preventive psychiatry." Journal of Mental Health Policy and Economics. Volume 9. Number 4. 193–200 Pages.
- World Health Organization.
(2004).
Prevention of mental disorders: Effective interventions and policy
options: Summary report. Retrieved from
http://www.who.int/mental_health/evidence/en/Prevention_of_Mental_Disorders.pdf.
- American Psychiatric Association
(2000).
Diagnostic and Statistical Manual of Mental Disorders. Author. Washington, DC. Edition 4, text rev.
Many people who would benefit from psychotherapy do not get it, either because they do
not know how to find it or because they feel that they will be stigmatized and
embarrassed if they seek help. The decision to not seek help is a very poor choice
because the effectiveness of mental health treatments is well documented and, no matter
where a person lives, there are treatments available. [1]
The first step in seeking help for psychological problems is to accept the stigma. It is
possible that some of your colleagues, friends, and family members will know that you
are seeking help and some may at first think more negatively of you for it. But you must
get past these unfair and close-minded responses. Feeling good about yourself is the
most important thing you can do, and seeking help may be the first step in doing so.
One question is how to determine if someone needs help. This question is not always easy
to answer because there is no clear demarcation between “normal” and “abnormal”
behavior. Most generally, you will know that you or others need help when the person’s
psychological state is negatively influencing his or her everyday behavior, when the
behavior is adversely affecting those around the person, and when the problems continue
over a period of time. Often people seek therapy as a result of a life-changing event
such as diagnosis of a fatal illness, an upcoming marriage or divorce, or the death of a
loved one. But therapy is also effective for general depression and anxiety, as well as
for specific everyday problems.
There are a wide variety of therapy choices, many of which are free. Begin in your
school, community, or church, asking about community health or counseling centers and
pastoral counseling. You may want to ask friends and family members for recommendations.
You’ll probably be surprised at how many people have been to counseling, and how many
recommend it.
There are many therapists who offer a variety of treatment options. Be sure to ask about
the degrees that the therapist has earned, and about the reputation of the center in
which the therapy occurs. If you have choices, try to find a person or location that you
like, respect, and trust. This will allow you to be more open, and you will get more out
of the experience. Your sessions with the help provider will require discussing your
family history, personality, and relationships, and you should feel comfortable sharing
this information.
Remember also that confronting issues requires time to reflect, energy to get to the
appointments and deal with consequential feelings, and discipline to explore your issues
on your own. Success at therapy is difficult, and it takes effort.
The bottom line is that going for therapy should not be a difficult decision for you. All
people have the right to appropriate mental health care just as they have a right to
general health care. Just as you go to a dentist for a toothache, you may go to therapy
for psychological difficulties. Furthermore, you can be confident that you will be
treated with respect and that your privacy will be protected, because therapists follow
ethical principles in their practices. The following provides a summary of these
principles as developed by the American Psychological Association. [2]
- Before therapy starts, you will be told what will happen in therapy, what it will
cost, what risks there are, and what alternatives are available. You will have an
opportunity to ask any questions you have and you will receive answers to those
questions before you commit yourself to the therapy process.
- If therapy involves other people, such as spouses or relatives, the psychologist
will explain how each person will fit into the therapy and what the therapist’s
relationship is with each person. If conflicts arise when working with several
people, the psychologist must immediately act to assure that everyone receives full
and respectful treatment.
- Psychologists may not have sexual relationships or other intimate relationships with
clients.
- The psychologist must end therapy when it has met your goals or is no longer
effective.
Psychodynamic Therapy
Psychodynamic therapy (psychoanalysis) is a psychological treatment based on Freudian and neo-Freudian
personality theories in which the therapist helps the patient explore the
unconscious dynamics of personality. The analyst engages with the
patient, usually in one-on-one sessions, often with the patient lying on a couch
and facing away. The goal of the psychotherapy is for the patient to talk about
his or her personal concerns and anxieties, allowing the
therapist to try to understand the underlying unconscious problems that are
causing the symptoms (the process of interpretation). The analyst may try out some interpretations on the
patient and observe how he or she responds to them.
The patient may be asked to verbalize his or her thoughts through free association, in which the therapist listens while the client talks about whatever comes to mind,
without any censorship or filtering. The client may also be asked to
report on his or her dreams, and the therapist will use dream
analysis to analyze the symbolism of the dreams in
an effort to probe the unconscious thoughts of the client and interpret
their significance. On the basis of the thoughts expressed by the
patient, the analyst discovers the unconscious conflicts causing the patient’s
symptoms and interprets them for the patient.
The goal of psychotherapy is to help the patient develop insight—that is, an understanding of the
unconscious causes of the disorder, [3] [4]
but the patient often shows resistance to these new
understandings, using defense mechanisms to avoid the painful feelings in his or her unconscious. The
patient might forget or miss appointments, or act out with hostile feelings
toward the therapist. The therapist attempts to help the patient develop insight
into the causes of the resistance. The sessions may also lead to transference, in which the patient
unconsciously redirects feelings experienced in an important personal
relationship toward the therapist. For instance, the patient may
transfer feelings of guilt that come from the father or mother to the therapist.
Some therapists believe that transference should be encouraged, as it allows the
client to resolve hidden conflicts and work through feelings that are present in
the relationships.
Important Characteristics and Experiences in Psychoanalysis
-
Free association. The therapist listens while the
client talks about whatever comes to mind, without any censorship or
filtering. The therapist then tries to interpret these free associations,
looking for unconscious causes of symptoms.
-
Dream analysis. The therapist listens while the client
describes his or her dreams and then analyzes the symbolism of the dreams in
an effort to probe the unconscious thoughts of the client and interpret
their significance.
-
Insight. An understanding by the patient of the
unconscious causes of his or her symptoms.
-
Interpretation. The therapist uses the patient’s
expressed thoughts to try to understand the underlying unconscious problems.
The analyst may try out some interpretations on the patient and observe how
he or she responds to them.
-
Resistance. The patient’s use of defense mechanisms to
avoid the painful feelings in his or her unconscious. The patient might
forget or miss appointments, or act out with hostile feelings toward the
therapist. The therapist attempts to help the patient develop insight into
the causes of the resistance.
-
Transference. The unconscious redirection of the
feelings experienced in an important personal relationship toward the
therapist. For instance, the patient may transfer feelings of guilt that
come from the father or mother to the therapist.
One problem with traditional psychoanalysis is that the sessions may take place
several times a week, go on for many years, and cost thousands of dollars. To
help more people benefit, modern psychodynamic approaches frequently use
shorter-term, focused, and goal-oriented approaches. In these “brief
psychodynamic therapies,” the therapist helps the client determine the important
issues to be discussed at the beginning of treatment and usually takes a more
active role than in classic psychoanalysis. [5]
Now click on “Psychodynamic” therapy and we will see what percentage of
psychotherapists in the United States practice Psychodynamic Therapy.
learn by doing
Listen to each segment of conversation between Terrance and his therapist, Dr.
Robinson, and then decide which characteristic of psychodynamic therapy is
represented.
Humanistic Therapies
Just as psychoanalysis is based on the personality theories of Freud and the
neo-Freudians, humanistic therapy is a
psychological treatment based on the personality theories of Carl Rogers and
other humanistic psychologists. Humanistic therapy is based on the idea
that people develop psychological problems when they are burdened by limits and
expectations placed on them by themselves and others, and the treatment
emphasizes the person’s capacity for self-realization and fulfillment.
Humanistic therapies attempt to promote growth and responsibility by helping
clients consider their own situations and the world around them and how they can
work to achieve their life goals.
Carl Rogers developed person-centered therapy (or
client-centered therapy), an approach to treatment
in which the client is helped to grow and develop as the therapist provides
a comfortable, nonjudgmental environment. In his book, A Way of Being, [6] Rogers argued that therapy was most
productive when the therapist created a positive relationship with the client—a
therapeutic alliance. The therapeutic alliance is a relationship between the client and the therapist that is
facilitated when the therapist is genuine (i.e., he or she creates no
barriers to free-flowing thoughts and feelings), when the therapist treats
the client with unconditional positive regard (i.e., values the client
without any qualifications, displaying an accepting attitude toward whatever
the client is feeling at the moment), and when the therapist develops
empathy with the client (i.e., that he or she actively listens to and
accurately perceives the personal feelings that the client
experiences).
The development of a positive therapeutic alliance has been found to be
exceedingly important to successful therapy. The ideas of genuineness, empathy,
and unconditional positive regard in a nurturing relationship in which the
therapist actively listens to and reflects the feelings of the client is
probably the most fundamental part of contemporary psychotherapy. [7]
Psychodynamic and humanistic therapies are recommended primarily for people
suffering from generalized anxiety or mood disorders, and who desire to feel
better about themselves overall. But the goals of people with other
psychological disorders, such as phobias, sexual problems, and
obsessive-compulsive disorder (OCD), are more specific. A person with a social
phobia may want to be able to leave his or her house, a person with a sexual
dysfunction may want to improve his or her sex life, and a person with OCD may
want to learn to stop letting his obsessions or compulsions interfere with
everyday activities. In these cases it is not necessary to revisit childhood
experiences or consider our capacities for self-realization—we simply want to
deal with what is happening in the present.
Now click on “Humanistic” therapy and we will see what percentage of psychotherapists in
the United States practice Psychodynamic Therapy.
References
- U.S. Department of Health and Human Services.
(1999).
Mental Health: A Report of the Surgeon General. U.S. Government Printing Office. Washington, DC.
- American Psychological Association.
(2010).
Ethical principles of psychologists and code of conduct. Retrieved from
http://www.apa.org/ethics/code/index.aspx?item=7#402.
- Epstein J., Stern E., and Silbersweig, D.
(2001).
"Neuropsychiatry at the millennium: The potential for mind/brain
integration through emerging interdisciplinary research
strategies." Clinical Neuroscience Research. Volume 1. Number 1. 10–18
Pages.
- Lubarsky, L., and Barrett, M. S.
(2006).
"The history and empirical status of key psychoanalytic
concepts." Annual Review of Clinical Psychology. Volume 2. Number 1. 1–19 Pages.
- Levenson, H.
(2010).
Brief Dynamic Therapy. American Psychological Association. Washington, DC.
- Rogers, C.
(1980).
A Way of Being. Houghton Mifflin. New York.
- Prochaska, J. O., and Norcross, J. C.
(2007).
Systems of Psychotherapy: A Transtheoretical Analysis. Brookes/Cole. Pacific Grove, CA. Edition 6.
Behavioral Therapy
Behavioral therapy is psychological
treatment that is based on principles of learning. The most direct approach
is through operant conditioning using reward or punishment. Reinforcement may be used
to teach new skills to people, for instance, those with autism or schizophrenia. [1] [2] [3]
If the patient has trouble dressing or grooming, then reinforcement techniques, such
as providing tokens that can be exchanged for snacks, are used to reinforce
appropriate behaviors such as putting on one’s clothes in the morning or taking a
shower at night. If the patient has trouble interacting with others, reinforcement
will be used to teach the client how to more appropriately respond in public, for
instance, by maintaining eye contact, smiling when appropriate, and modulating tone
of voice.
As the patient practices the different techniques, the appropriate behaviors are
shaped through reinforcement to allow the client to manage more complex social
situations. In some cases observational learning may also be used; the client may be
asked to observe the behavior of others who are more socially skilled to acquire
appropriate behaviors. People who learn to improve their interpersonal skills through
skills training may be more accepted by others and this social support may have
substantial positive effects on their emotions.
Exposure therapy is a behavioral therapy
based on the classical conditioning principle of extinction in which people are
confronted with a feared stimulus with the goal of decreasing their negative
emotional responses to it. [4] Exposure treatment can be carried out
in real situations or through imagination, and it is used in the treatment of panic
disorder, agoraphobia, social phobia, OCD, and posttraumatic stress disorder
(PTSD).
In flooding, a client is exposed to the
source of his fear all at once. An agoraphobic might be taken to a crowded
shopping mall or someone with an extreme fear of heights to the top of a tall
building. The assumption is that the fear will subside as the client habituates to
the situation while receiving emotional support from the therapist during the
stressful experience. An advantage of the flooding technique is that it is quick and
often effective, but a disadvantage is that the patient may relapse after a short
period of time.
More frequently, the exposure is done more gradually. Systematic
desensitization is a behavioral treatment that combines
imagining or experiencing the feared object or situation with relaxation
exercises. [4] The
client and the therapist work together to prepare a hierarchy of
fears, starting with the least frightening, and moving to the most
frightening scenario surrounding the object as shown in the table below. The patient
then confronts her fears in a systematic manner, sometimes using her imagination but
usually, when possible, in real life.
| Hierarchy of Fears Used in Systematic Desensitization |
|---|
| From Flat World Knowledge, Introduction to
Psychology, CC-BY-NC-SA. |
| Behavior |
Fear Rating |
| Think about a spider. |
10 |
| Look at a photo of a spider. |
25 |
| Look at a real spider in a closed box. |
50 |
| Hold the box with the spider. |
60 |
| Let a spider crawl on your desk. |
60 |
| Let a spider crawl on your shoe. |
80 |
| Let a spider crawl on your pants leg. |
90 |
| Let a spider crawl on your sleeve. |
95 |
| Let a spider crawl on your bare arm. |
100 |
|
Desensitization techniques use the principle of counterconditioning, in which a second incompatible
response (relaxation, e.g., through deep breathing) is conditioned to an already
conditioned response (the fear response). The continued pairing of the
relaxation responses with the feared stimulus as the patient works up the hierarchy
gradually leads the fear response to be extinguished and the relaxation response to
take its place.
Behavioral therapy works best when people directly experience the feared object.
Fears of spiders are more directly habituated when the patient interacts with a real
spider, and fears of flying are best extinguished when the patient gets on a real
plane. But it is often difficult and expensive to create these experiences for the
patient. Recent advances in virtual reality have allowed clinicians to provide
behavior therapy in what seem like real situations to the patient. In virtual reality CBT, the therapist uses
computer-generated, three-dimensional, lifelike images of the feared stimulus in a
systematic desensitization program. Specially designed computer equipment,
often with a head-mount display, is used to create a simulated environment. A common
use is in helping soldiers who are experiencing PTSD return to the scene of the
trauma and learn how to cope with the stress it invokes.
Some of the advantages of the virtual reality treatment approach are that it is
economical, the treatment session can be held in the therapist’s office with no loss
of time or confidentiality, the session can easily be terminated as soon as a patient
feels uncomfortable, and many patients who have resisted live exposure to the object
of their fears are willing to try the new virtual reality option first.
Aversion therapy is a type of behavior
therapy in which positive punishment is used to reduce the frequency of an
undesirable behavior. An unpleasant stimulus is intentionally paired with a
harmful or socially unacceptable behavior until the behavior becomes associated with
unpleasant sensations and is hopefully reduced. A child who wets his bed may be
required to sleep on a pad that sounds an alarm when it senses moisture. Over time,
the positive punishment produced by the alarm reduces the bedwetting behavior. [5]
Aversion therapy is also used to stop other specific behaviors such as nail
biting. [6]
Alcoholism has long been treated with aversion therapy. [7] In a standard approach,
patients are treated at a hospital where they are administered a drug, antabuse, that makes them nauseous if they consume any
alcohol. The technique works very well if the user keeps taking the drug, [8] but unless it
is combined with other approaches, the patients are likely to relapse after they stop
the drug.
Now click on “Behavioral” therapy and we will see what percentage of psychotherapists
in the United States practice Behavioral Therapy.
Cognitive Therapy
While behavioral approaches focus on the actions of the patient, cognitive therapy is a psychological treatment that helps
clients identify incorrect or distorted beliefs that are contributing to
disorder. In cognitive therapy the therapist helps the patient develop new,
healthier ways of thinking about themselves and about the others around them. The
idea of cognitive therapy is that changing thoughts will change emotions, and that
the new emotions will then influence behavior.
The goal of cognitive therapy is not necessarily to get people to think more
positively but rather to think more accurately. For instance, a person who thinks “no
one cares about me” is likely to feel rejected, isolated, and lonely. If the
therapist can remind the person that she has a mother or daughter who does care about
her, more positive feelings will likely follow. Similarly, changing beliefs from “I
have to be perfect” to “No one is always perfect—I’m doing pretty good,” from “I am a
terrible student” to “I am doing well in some of my courses,” or from “She did that
on purpose to hurt me” to “Maybe she didn’t realize how important it was to me” may
all be helpful.
The psychiatrist Aaron T. Beck (1921–) and the psychologist Albert Ellis (1913–2007)
together provided the basic principles of cognitive therapy. Ellis [9] called his approach rational emotive behavior therapy (REBT) or rational emotive therapy (RET), and he focused on pointing out the flaws in
the patient’s thinking. Ellis noticed that people experiencing strong negative
emotions tend to personalize and overgeneralize their beliefs, leading to an
inability to see situations accurately. [10] In REBT, the therapist’s goal is to
challenge these irrational thought patterns, helping the patient replace the
irrational thoughts with more rational ones, leading to the development of more
appropriate emotional reactions and behaviors.
Beck’s [11] [12]
cognitive
therapy was based on his observation that people who were depressed generally had a
large number of highly accessible negative thoughts that influenced their thinking.
His goal was to develop a short-term therapy for depression that would modify these
unproductive thoughts. Beck’s approach challenges the client to test his beliefs
against concrete evidence. If a client claims that “everybody at work is out to get
me,” the therapist might ask him to provide instances to corroborate the claim. At
the same time the therapist might point out contrary evidence, such as the fact that
a certain coworker is actually a loyal friend or that the patient’s boss had recently
praised him.
Now click on “Cognitive” therapy and we will see what percentage of psychotherapists
in the United States practice Cognitive Therapy.
Cognitive-Behavior Therapy
Cognitive-behavior therapy (CBT) is a
structured approach to treatment that attempts to reduce psychological disorders through systematic procedures based on cognitive and
behavioral principles. As you can see in following figure, CBT is based on
the idea that there is a recursive link among our thoughts, our feelings, and our
behavior. For instance, if we are feeling depressed, our negative thoughts (“I am
doing poorly in my chemistry class”) lead to negative feelings (“I feel hopeless and
sad”), which then contribute to negative behaviors (lethargy, disinterest, lack of
studying). When we or other people look at the negative behavior, the negative
thoughts are reinforced and the cycle repeats itself. [13] Similarly, in panic disorder a patient may
misinterpret his or her feelings of anxiety as a sign of an impending physical or
mental catastrophe (such as a heart attack), leading to an avoidance of a particular
place or social situation. The fact that the patient is avoiding the situation
reinforces the negative thoughts. Again, the thoughts, feelings, and behavior amplify
and distort each other.
CBT is a very broad approach that is used for the treatment of a variety of problems,
including mood, anxiety, personality, eating, substance abuse, attention-deficit, and
psychotic disorders. CBT treats the symptoms of the disorder (the behaviors or the
cognitions) and does not attempt to address the underlying issues that cause the
problem. The goal is simply to stop the negative cycle by intervening to change
cognition or behavior. The client and the therapist work together to develop the
goals of the therapy, the particular ways that the goals will be reached, and the
timeline for reaching them. The procedures are problem-solving and action-oriented,
and the client is forced to take responsibility for his or her own treatment. The
client is assigned tasks to complete that will help improve the disorder and takes an
active part in the therapy. The treatment usually lasts between 10 and 20
sessions.
Depending on the particular disorder, some CBT treatments may be primarily behavioral
in orientation, focusing on the principles of classical, operant, and observational
learning, whereas other treatments are more cognitive, focused on changing negative
thoughts related to the disorder. But almost all CBT treatments use a combination of
behavioral and cognitive approaches.
Combination (Eclectic) Approaches to Therapy
To this point we have considered the different approaches to psychotherapy under the
assumption that a therapist will use only one approach with a given patient. But this
is not the case; as you saw in the pie chart "The Many Types of Therapy Practiced in
the United
States,"
the most commonly practiced approach to therapy is an eclectic
therapy, an approach to treatment in which the therapist
uses whichever techniques seem most useful and relevant for a given patient.
For bipolar disorder, for instance, the therapist may use both psychological skills
training to help the patient cope with the severe highs and lows, but may also
suggest that the patient consider biomedical drug therapies. [14]
Treatment for major depressive disorder usually involves antidepressant drugs as well
as CBT to help the patient deal with particular problems. [15]
As we have seen in the unit on disorders, one of the most commonly diagnosed
disorders is borderline personality disorder (BPD). Consider this description,
typical of the type of borderline patient who arrives at a therapist’s office:
Even as an infant, it seemed that there was something different about Bethany. She
was an intense baby, easily upset and difficult to comfort. She had very severe
separation anxiety—if her mother left the room, Bethany would scream until she
returned. In her early teens, Bethany became increasingly sullen and angry. She
started acting out more and more—yelling at her parents and teachers and engaging in
impulsive behavior such as promiscuity and running away from home. At times Bethany
would have a close friend at school, but some conflict always developed and the
friendship would end.
By the time Bethany turned 17, her mood changes were totally unpredictable. She was
fighting with her parents almost daily, and the fights often included violent
behavior on Bethany’s part. At times she seemed terrified to be without her mother,
but at other times she would leave the house in a fit of rage and not return for a
few days. One day, Bethany’s mother noticed scars on Bethany’s arms. When confronted
about them, Bethany said that one night she just got more and more lonely and nervous
about a recent breakup until she finally stuck a lit cigarette into her arm. She
said, “I didn’t really care for him that much, but I had to do something
dramatic.”
When she was 18 Bethany rented a motel room where she took an overdose of sleeping
pills. Her suicide attempt was not successful, but the authorities required that she
seek psychological help.
Most therapists will deal with a case such as Bethany’s using an eclectic approach.
First, because her negative mood states are so severe, they will likely recommend
that she start taking antidepressant medications. These drugs are likely to help her
feel better and will reduce the possibility of another suicide attempt, but they will
not change the underlying psychological problems. Therefore, the therapist will also
provide psychotherapy.
The first sessions of the therapy will likely be based primarily on creating trust.
Person-centered approaches will be used in which the therapist attempts to create a
therapeutic alliance conducive to a frank and open exchange of information.
If the therapist is trained in a psychodynamic approach, he or she will probably
begin intensive face-to-face psychotherapy sessions at least three times a week. The
therapist may focus on childhood experiences related to Bethany’s attachment
difficulties but will also focus in large part on the causes of the present behavior.
The therapist will understand that because Bethany does not have good relationships
with other people, she will likely seek a close bond with the therapist, but the
therapist will probably not allow the transference relationship to develop fully. The
therapist will also realize that Bethany will probably try to resist the work of the
therapist.
Most likely the therapist will also use principles of CBT. For one, cognitive therapy
will likely be used in an attempt to change Bethany’s distortions of reality. She
feels that people are rejecting her, but she is probably bringing these rejections on
herself. If she can learn to better understand the meaning of other people’s actions,
she may feel better. And the therapist will likely begin using some techniques of
behavior therapy, for instance, by rewarding Bethany for successful social
interactions and progress toward meeting her important goals.
The eclectic therapist will continue to monitor Bethany’s behavior as the therapy
continues, bringing into play whatever therapeutic tools seem most beneficial.
Hopefully, Bethany will stay in treatment long enough to make some real progress in
repairing her broken life.
One example of an eclectic treatment approach that has been shown to be successful in
treating BPD is dialectical behavioral therapy (DBT). [16] DBT is
essentially a cognitive therapy, but it includes a particular emphasis on attempting
to enlist the help of the patient in his or her own treatment. A dialectical
behavioral therapist begins by attempting to develop a positive therapeutic alliance
with the client, and then tries to encourage the patient to become part of the
treament process. In DBT the therapist aims to accept and validate the client’s
feelings at any given time while nonetheless informing the client that some feelings
and behaviors are maladaptive, and showing the client better alternatives. The
therapist will use both individual and group therapy, helping the patient work toward
improving interpersonal effectiveness, emotion regulation, and distress tolerance
skills.
Now click on “Eclectic (combination)” types of therapy and we will see what
percentage of psychotherapists in the United States practice Eclectic types of
therapy.
learn by doing
Instructions: Below are four examples of therapy sessions
between a client and therapist. Read each of the dialogues and determine the type of
therapy that is most likely taking place.
Example 1:
Therapist: So, tell me about your childhood.
Client: Well, I had a tough relationship with my father. He
never seemed to trust me to do the right thing. I think that still influences how I
deal with men today. It even has had an impact on my sleeping habits too.
Therapist: Tell me more about your sleeping habits. Please
feel free to recall any dreams you can remember so we can explore them.
Client: Just last night I had the wildest dream. I was
running in a forest being chased by ninjas. I couldn’t seem to escape. They were all
around me. What does it mean?
Example 2:
Client: Thank you for meeting with me on such short notice,
Dr. Lovelace. I’ve heard such good things about you and how warm and understanding
you are, which is why I decided to see you for therapy.
Therapist: I am here to help. I believe that every person has
the capacity to change and grow. We all have the answers to our problems, we just may
need a little guidance sometimes. Tell me more about yourself and why you are here,
Susan.
Client: Well, I’m here because I’ve been doing bad things
lately. I’ve been yelling at my kids, and I’ve been very irritable with my coworkers.
This is so unlike me. Do you think that makes me a bad person?
Therapist: I can understand why you might feel upset with
yourself, Susan. This doesn’t match with your concept of yourself, and it makes you
feel bad. I’m not judging you; I accept you for who you are. How do you think you can
better line up your ideas about yourself (as being a good person) with reality?
Example 3:
Therapist: I understand you are here because you have a
terrible fear of flying. Is that correct?
Client: Yes, doctor, it is. I get horrible panic attacks
going into airports and even thinking about getting on a plane causes me some
anxiety. What can I do to fix this?
Therapist: Let’s start by creating a hierarchy of fears that
you have around flying. Please start with what causes you the least amount of anxiety
to the most amount of anxiety around this issue. Then we’ll work through these
anxieties and help you to relax at each stage. You can’t be relaxed and anxious at
the same time, right?
Client: Good point, doctor. I guess the least amount of
anxiety would be thinking about planes. The next would be booking a flight. Next
would be going to the airport, and after that, stepping on the plane and getting
ready for take-off. I think you know that the flying part would produce the most
anxiety!
Example 4:
Client: I’ve been coming here for a few weeks now, Dr.
Harris, and you’ve asked me to monitor how I’m thinking about things.
Therapist: Yes. How is it going? What have been some of your
automatic thoughts, Lisa?
Client: Well, I find that I keep doubting myself and telling
myself that I’m not a good student. If I get an answer wrong in class, I tell myself
I’m stupid and that other people must think I’m so incompetent. I think this is what
is leading me to feel sad and depressed most days.
Therapist: Thank you for sharing that, Lisa. Negative
thoughts and pessimistic thinking can lead us to have bad feelings about ourselves. I
like to encourage my clients to talk to themselves as a friend would. A friend would
never speak to us that way, so why should we?
References
- Granholm, E., McQuaid, J. R., Link, P. C., Fish,
S., Patterson, T., and
Jeste, D. V.
(2008).
"Neuropsychological predictors of functional outcome in cognitive
behavioral
social skills training for older people with
schizophrenia." Schizophrenia Research. Volume 100. Number 1–3. 133–143
Pages.
- Herbert, J. D., Gaudini, B. A., Rheingold, A. A., Myers, V. H., Dalrymple,
K., and Nolan, E. M.
(2005).
"Social skills training augments the effectiveness of cognitive behavioral
group therapy for social anxiety disorder." Behavior Therapy. Volume 36. Number 2. 125–138 Pages.
- Scattone, D.
(2007).
"Social skills interventions for children with autism." Psychology in the Schools. Volume 44. Number 7. 717–726 Pages.
- Wolpe, J.
(2007).
The Practice of Behavior Therapy. Pergamon. New York.
- Houts, A. C., Berman, J. S., and Abramson, H.
(1994).
"Effectiveness of psychological and pharmacological treatments for nocturnal
enuresis." Journal of Consulting and Clinical Psychology. Volume 62. Number 4. 737–745 Pages.
- Allen, K. W.
(1996).
"Chronic nailbiting: A controlled comparison of competing response and mild
aversion treatments." Behaviour Research and Therapy. Volume 32. Number 3. 269–272 Pages.
- Baker, T. B., and Cannon, D. S.
(1988).
Assessment and Treatment of Addictive Disorders. Praeger. New York.
- Krampe, H., Stawicki, S., Wagner, T.,
Bartels, C., Aust, C., Rüther, E., et
al.
(2006).
"Follow-up of 180 alcoholic patients for up to 7 years after
outpatient
treatment: Impact of alcohol deterrents on outcomes."
Alcoholism: Clinical and Experimental Research. Volume 30. Number 1.
86–95 Pages.
- Ellis, A.
(2004).
"Why rational emotive behavior therapy is the most comprehensive
and effective
form of behavior therapy." Journal of Rational-Emotive
and Cognitive-Behavior Therapy. Volume 22. Number 2. 85–92 Pages.
- Leahy, R. L.
(2003).
Cognitive Therapy Techniques: A Practitioner’s Guide. Guilford Press. New York.
- Beck, J. S.
(1995).
Cognitive Therapy: Basics and Beyond. Guilford Press. New York.
- Beck, A. T., Freeman, A., and Davis, D. D.
(2004).
Cognitive Therapy of Personality Disorders. Guilford Press. New York.
- Beck, A. T.
(1976).
Cognitive Therapy and the Emotional Disorders. New American Library. New York.
- Newman, C. F., Leahy, R. L., Beck, A. T., Reilly-Harrington, N. A., and
Gyulai, L.
(2002).
Bipolar Disorder: A Cognitive Therapy Approach.
Chapter Clinical management of depression, hopelessness, and
suicidality in
patients with bipolar disorder. American Psychological
Association. Washington, DC. 79–100 Pages. C. F. Newman, R. L. Leahy, A.
T. Beck, N. A. Reilly-Harrington, and L. Gyulai
(Eds.).
- McBride, C., Farvolden, P., and Swallow, S. R.
(2002).
Cognitive Schemas and Core Beliefs in Psychological Problems: A
Scientist-Practitioner Guide. Chapter Major
depressive disorder and cognitive schemas. American Psychological
Association. Washington, DC. 11–39 Pages. L. P. Riso, P. L. du Toit, D.
J. Stein, and J. E. Young (Eds.).
- Linehan, M. M., and Dimeff, L.
(2001).
"Dialectical behavior therapy in a nutshell." California Psychologist. Volume 34. Number 1. 10–13 Pages.
Like other medical problems, psychological disorders may in some cases be
treated biologically. Biomedical therapies are treatments designed to reduce psychological disorder by
influencing the action of the central nervous system. These therapies
primarily involve the use of medications but also include direct methods of
brain intervention, including electroconvulsive therapy
(ECT),transcranial magnetic stimulation (TMS),
and psychosurgery.
Psychologists understand that an appropriate balance of neurotransmitters
in the brain is necessary for mental health. If there is a proper balance
of chemicals, then the person’s mental health will be acceptable, but
psychological disorder will result if there is a chemical imbalance. The
most frequently used biological treatments provide the patient with
medication that influences the production and reuptake of
neurotransmitters in the central nervous system (CNS). The use of these
drugs is rapidly increasing, and drug therapy is now the most common
approach to treatment of most psychological disorders.
Unlike some medical therapies that can be targeted toward specific
symptoms, current psychological drug therapies are not so specific; they
don’t change particular behaviors or thought processes, and they don’t
really solve psychological disorders. However, although they cannot
“cure” disorder, drug therapies are nevertheless useful therapeutic
approaches, particularly when combined with psychological therapy, in
treating a variety of psychological disorders. The best drug combination
for the individual patient is usually found through trial and
error. [1]
Using Stimulants to Treat ADHD
Attention-deficit/hyperactivity disorder (ADHD) is frequently treated
with biomedical therapy, usually along with cognitive-behavior therapy
(CBT). The most commonly prescribed drugs for ADHD are psychostimulants,
including Ritalin, Adderall, and Dexedrine. Short-acting forms of the
drugs are taken as pills and last between 4 and 12 hours, but some of the
drugs are also available in long-acting forms (skin patches) that can be
worn on the hip and last up to 12 hours. The patch is placed on the child
early in the morning and worn all day.
Stimulants improve the major symptoms of ADHD, including inattention,
impulsivity, and hyperactivity, often dramatically, in about 75% of the
children who take
them. [2]
But the effects of the drugs wear off quickly. Additionally, the best
drug and best dosage varies from child to child, so it may take some time
to find the correct combination.
It may seem surprising to you that a disorder that involves hyperactivity
is treated with a psychostimulant, a drug that normally increases
activity. The answer lies in the dosage. When large doses of stimulants
are taken, they increase activity, but in smaller doses the same
stimulants improve attention and decrease motor
activity. [3]
The most common side effects of psychostimulants in children include
decreased appetite, weight loss, sleeping problems, and irritability as
the effect of the medication tapers off. Stimulant medications may also
be associated with a slightly reduced growth rate in children, although
in most cases growth isn’t permanently
affected. [4]
Antidepressant Medications
Antidepressant medications are drugs designed to improve moods. Although they are used
primarily in the treatment of depression, they are also effective for
patients who suffer from anxiety, phobias, and obsessive-compulsive
disorders. Antidepressants work by influencing the production and
reuptake of neurotransmitters that relate to emotion, including
serotonin, norepinephrine, and dopamine. Although exactly why they work
is not yet known, as the amount of the neurotransmitters in the CNS is
increased through the action of the drugs, the person often experiences
less depression.
The original antidepressants were the tricyclic
antidepressants, with the brand names of Tofranil and Elavil, and
the monamine oxidase inhibitors (MAOIs), including Nardil and Parnate. These
medications work by increasing the amount of serotonin, norepinephrine,
and dopamine at the synapses, but they also have severe side effects
including potential increases in blood pressure and the need to follow
particular diets.
The antidepressants most prescribed today are the selective serotonin reuptake inhibitors (SSRIs), including Prozac, Paxil, and Zoloft, which are designed
to selectively block the reuptake of serotonin at the synapse, thereby
leaving more serotonin available in the CNS. SSRIs are safer and have
fewer side effects than the tricyclics or the
MAOIs. [5] [6]
SSRIs are effective, but patients taking them often suffer a variety of
sometimes unpleasant side effects, including dry mouth, constipation,
blurred vision, headache, agitation, drowsiness, as well as a reduction
in sexual enjoyment.
Recently, there has been concern that SSRIs may increase the risk of
suicide among teens and young adults, probably because when the
medications begin working they give patients more energy, which may lead
them to commit the suicide that they had been planning but lacked the
energy to go through with. This concern has led the FDA to put a warning
label on SSRI medications and has led doctors to be more selective about
prescribing antidepressants to this age
group. [7] [8] [9]
Because the effects of antidepressants may take weeks or even months to
develop, doctors usually work with each patient to determine which
medications are most effective, and may frequently change medications
over the course of therapy. In some cases other types of antidepressants
may be used instead of or in addition to the SSRIs. These medications
also work by blocking the reuptake of neurotransmitters, including
serotonin, norepinephrine, and dopamine. Brand names of these medications
include Effexor and Wellbutrin.
Patients who are suffering from bipolar disorder are not helped by the
SSRIs or other antidepressants because their disorder also involves the
experience of overly positive moods. Treatment is more complicated for
these patients, often involving a combination of antipsychotics and
antidepressants along with mood stabilizing
medications. [10]
The most well-known mood stabilizer, lithium carbonate (or “lithium”),
was approved by the FDA in the 1970s for treating both manic and
depressive episodes, and it has proven very effective. Anticonvulsant
medications can also be used as mood stabilizers. Another drug, Depakote,
has also proven very effective, and some bipolar patients may do better
with it than with
lithium. [11]
People who take lithium must have regular blood tests to be sure that the
levels of the drug are in the appropriate range. Potential negative side
effects of lithium are loss of coordination, slurred speech, frequent
urination, and excessive thirst. Though side effects often cause patients
to stop taking their medication, it is important that treatment be
continuous, rather than intermittent. There is no cure for bipolar
disorder, but drug therapy does help many people.
Antianxiety Medications
Antianxiety medications are drugs that help relieve fear or anxiety. They work by increasing
the action of the neurotransmitter GABA. The increased level of GABA
helps inhibit the action of the sympathetic division of the autonomic
nervous system, creating a calming experience.
The most common class of antianxiety medications is the tranquilizers, known as benzodiazepines. These drugs, which are prescribed millions of
times a year, include Ativan, Valium, and Xanax. The benzodiazepines act
within a few minutes to treat mild anxiety disorders but also have major
side effects. They are addictive, frequently leading to tolerance, and
they can cause drowsiness, dizziness, and unpleasant withdrawal symptoms
including relapses into increased
anxiety. [12] Furthermore,
because the effects of the benzodiazepines are very similar to those of
alcohol, they are very dangerous when combined with it.
Antipsychotic Medications
Until the middle of the 20th century, schizophrenia was inevitably
accompanied by the presence of positive symptoms, including bizarre,
disruptive, and potentially dangerous behavior. As a result,
schizophrenics were locked in asylums to protect them from themselves and
to protect society from them. In the 1950s, a drug called chlorpromazine
(Thorazine) was discovered that could reduce many of the positive
symptoms of schizophrenia. Chlorpromazine was the first of many
antipsychotic drugs.
Antipsychotic drugs (neuroleptics) are drugs that treat the symptoms of schizophrenia and
related psychotic disorders. Today there are many antipsychotics,
including Thorazine, Haldol, Clozaril, Risperdal, and Zyprexa. Some of
these drugs treat the positive symptoms of schizophrenia, and some treat
both the positive, negative, and cognitive symptoms.
The discovery of chlorpromazine and its use in clinics has been described
as the single greatest advance in psychiatric care, because it has
dramatically improved the prognosis of patients in psychiatric hospitals
worldwide. Using antipsychotic medications has allowed hundreds of
thousands of people to move out of asylums into individual households or
community mental health centers, and in many cases to live near-normal
lives.
Antipsychotics reduce the positive symptoms of schizophrenia by reducing
the transmission of dopamine at the synapses in the limbic system, and
they improve negative symptoms by influencing levels of
serotonin. [13]
Despite their effectiveness, antipsychotics have some negative side
effects, including restlessness, muscle spasms, dizziness, and blurred
vision. In addition, their long-term use can cause permanent neurological
damage, a condition called tardive dyskinesia that
causes uncontrollable muscle movements, usually in
the mouth
area. [14]
Newer antipsychotics treat more symptoms with fewer side effects than
older medications do. [15]
References
- Biedermann, F., and Fleischhacker, W. W.
(2009).
"Antipsychotics in the early stage of development." Current Opinion Psychiatry. Volume 22. Number 3. 326–330 Pages.
- Greenhill, L. L., Halperin, J. M., and
Abikof, H.
(1999).
"Stimulant medications." Journal of the American Academy of Child
and Adolescent Psychiatry. Volume 38. Number 5. 503–512 Pages.
- Zahn, T. P., Rapoport, J. L., and Thompson, C.
L.
(1980).
"Autonomic and behavioral effects of dextroamphetamine and placebo
in normal and hyperactive prepubertal boys." Journal of Abnormal Child
Psychology. Volume 8. Number 2. 145–160 Pages.
- Spencer, T. J., Biederman, J., Harding, M.,
and O’Donnell, D.
(1996).
"Growth deficits in ADHD children revisited: Evidence for
disorder-associated growth delays?." Journal of the American Academy of
Child and Adolescent Psychiatry. Volume 35. Number 11. 1460–1469 Pages.
- Fraser, A. R.
(2000).
"Antidepressant choice to minimize treatment resistance." British
Journal of Psychiatry. Volume 176. Number 4. 493–494 Pages.
- Hollon, S. D., Thase, M. E., and Markowitz, J. C.
(2002).
"Treatment and prevention of depression." Psychological Science in the Public Interest. Volume 3. Number 1. 39–77 Pages.
- Healy, D., and Whitaker, C. J.
(2003).
"Antidepressants and suicide: Risk-benefit conundrums." Journal of
Psychiatry and Neuroscience. Volume 28. Number 5. 331–339 Pages.
- Simon, G. E.
(2006).
"The antidepressant quandary—Considering suicide risk when treating
adolescent depression." New England Journal of Medicine. Volume 355.
Number 26. 2722–2723 Pages.
- Simon, G. E., Savarino, J., Operskalski, B., and Wang, P. S.
(2006).
"Suicide risk during antidepressant treatment." American Journal of Psychiatry. Volume 163. Number 1. 41–47 Pages.
- McElroy, S. L., and Keck, P. E.
(2000).
"Pharmacologic agents for the treatment of acute bipolar mania."
Biological Psychiatry. Volume 48. Number 6. 539–557 Pages.
- Kowatch, R. A., Suppes, T., Carmody, T. J.,
Bucci, J. P., Hume, J. H., Kromelis, M., et al.
(2000).
"Effect size of lithium, divalproex sodium, and carbamazepine in
children and adolescents with bipolar disorder." Journal of the American
Academy of Child and Adolescent Psychiatry. Volume 39. Number 6.
713–720 Pages.
- Otto, M. W., Pollack, M. H., Sachs, G. S.,
Reiter, S. R., Meltzer-Brody, S., and Rosenbaum, J. F.
(1993).
"Discontinuation of benzodiazepine treatment: Efficacy of
cognitive-behavioral therapy for patients with panic disorder." American
Journal of Psychiatry. Volume 150. Number 10. 1485–1490 Pages.
- Marangell, L. B., Silver, J. M., Goff, D. C., and Yudofsky, S. C.
(2003).
The American Psychiatric Publishing Textbook of Clinical Psychiatry.
Chapter Psychopharmacology and electroconvulsive therapy. American
Psychiatric Publishing. Arlington, VA. Edition 4. 1047–1149 Pages. R. E.
Hales and S. C. Yudofsky (Eds.).
- National Institute of Mental Health.
(2008).
Mental health medications (NIH Publication No. 08-3929). Retrieved from http://www.nimh.nih.gov/health/publications/mental-health-medications/complete-index.shtml#pub4.
- Casey, D. E.
(1996).
"Side effect profiles of new antipsychotic agents." Journal of
Clinical Psychiatry. Volume 57. Number Suppl. 11. 40–45 Pages.
In cases of severe disorder it may be desirable to directly influence brain
activity through electrical activation of the brain or through brain surgery.
Electroconvulsive therapy (ECT) (as shown in the figure below) is a medical procedure designed to alleviate psychological disorder in which
electric currents are passed through the brain, deliberately triggering a
brief seizure. ECT has been used since the
1930s to treat severe depression.
When it was first developed, the procedure involved strapping the patient to a
table before the electricity was administered. The patient was knocked out by
the shock, went into severe convulsions, and awoke later, usually without any
memory of what had happened. Today ECT is used only in the most severe cases
when all other treatments have failed, and the practice is more humane. The
patient is first given muscle relaxants and a general anesthesia, and precisely
calculated electrical currents are used to achieve the most benefit with the
fewest possible risks.
ECT is very effective; about 80% of people who undergo three sessions of ECT
report dramatic relief from their depression. ECT reduces suicidal thoughts and
is assumed to have prevented many
suicides. [1] On the other hand, the
positive effects of ECT do not always last; over one-half of patients who
undergo ECT experience relapse within one year, although antidepressant
medication can help reduce this
outcome. [2] ECT may also cause
short-term memory loss or cognitive impairment. [3] [4]
Although ECT continues to be used, newer approaches to treating chronic
depression are also being developed. A newer and gentler method of brain
stimulation is transcranial magnetic stimulation (TMS),
a medical procedure designed to reduce psychological
disorder that uses a pulsing magnetic coil to electrically stimulate the
brain as shown in the following figure. TMS seems to work by activating
neural circuits in the prefrontal cortex, which is less active in people with
depression, causing an elevation of mood. TMS can be performed without
sedation, does not cause seizures or memory loss, and may be as effective as
ECT. [5] [6]
TMS has also been used in the treatment of Parkinson’s disease and
schizophrenia.
Still other biomedical therapies are being developed for people with severe
depression that persists over years. One approach involves implanting a device
in the chest that stimulates the vagus nerve, a major nerve that descends from
the brain stem toward the
heart. [7] [8]
When the vagus nerve is stimulated by the device, it activates brain structures
that are less active in severely depressed people.
Psychosurgery, that is, surgery that removes or
destroys brain tissue in the hope of improving disorder, is reserved for the most
severe cases. The most well-known psychosurgery is the prefrontal
lobotomy. Developed in 1935 by Nobel Prize winner Egas Moniz to treat severe
phobias and anxiety, the procedure destroys the connections between the prefrontal cortex
and the rest of the brain. Lobotomies were performed on thousands of patients. The
procedure—which was never validated scientifically—left many patients in worse condition
than before, subjecting the already suffering patients and their families to further
heartbreak. [9]
Perhaps the most notable failure was the lobotomy performed on Rosemary Kennedy, the sister
of President John F. Kennedy, which left her severely incapacitated.
There are very few centers that still conduct psychosurgery today, and when such surgeries
are performed, they are much more limited in nature and called cingulotomy. [10] The ability to more accurately image
and localize brain structures using modern neuroimaging techniques suggests that new, more
accurate, and more beneficial developments in psychosurgery may soon be available. [11]
References
- Kellner, C. H., Fink, M., Knapp, R., Petrides, G.,
Husain, M., Rummans, T., et al.
(2005).
"Relief of expressed suicidal intent by ECT: A consortium for
research in ECT study." American Journal of Psychiatry. Volume 162.
Number 5. 977–982 Pages.
- Sackheim, H. A., Haskett, R. F., Mulsant,
B. H., Thase, M. E., Mann, J. J., Pettinati, H., et al.
(2001).
"Continuation pharmacotherapy in the prevention of relapse
following electroconvulsive therapy: A randomized controlled trial."
Journal of the American Medical Association. Volume 285. Number 10.
1299–1307 Pages.
- Abrams, R.
(1997).
Electroconvulsive Therapy. Oxford University Press. Oxford, England. Edition 3.
- Sackeim, H. A., Prudic, J., Fuller, R.,
Keilp, J., Philip, W., Lavori, P. W., and Olfson, M.
(2007).
"The cognitive effects of electroconvulsive therapy in community
settings." Neuropsychopharmacology. Volume 32. Number 1. 244–254 Pages.
- Loo, C. K., Schweitzer, I., and Pratt, C.
(2006).
"Recent advances in optimizing electroconvulsive therapy."
Australian and New Zealand Journal of Psychiatry. Volume 40. Number 8.
632–638 Pages.
- Rado, J., Dowd, S. M., and Janicak, P. G.
(2008).
"The emerging role of transcranial magnetic stimulation (TMS) for
treatment of psychiatric disorders." Directions in Psychiatry. Volume
28. Number 4. 315–332 Pages.
- Corcoran, C. D., Thomas, P., Phillips, J.,
and O’Keane, V.
(2008).
"Vagus nerve stimulation in chronic treatment-resistant depression:
Preliminary findings of an open-label study." Directions in Psychiatry.
Volume 189. Number 3. 282–283 Pages.
- Nemeroff, C., Mayberg, H., Krahl, S.,
McNamara, J., Frazer, A., Henry, T., et al.
(2006).
"VNS therapy in treatment-resistant depression: Clinical evidence
and putative neurobiological mechanisms." Neuropsychopharmacology.
Volume 31. Number 7. 1345–1355 Pages.
- Valenstein, E.
(1986).
Great and Desperate Cures: The Rise and Decline of Psychosurgery and Other Radical Treatments for Mental Illness. Basic Books. New York.
- Dougherty, D., Baer, L., Cosgrove, G.,
Cassem, E., Price, B., Nierenberg, A., et al.
(2002).
"Prospective long-term follow-up of 44 patients who received
cingulotomy for treatment-refractory obsessive-compulsive disorder."
American Journal of Psychiatry. Volume 159. Number 2. 269–275 Pages.
- Sachdev, P. S., and Chen, X.
(2009).
"Neurosurgical treatment of mood disorders: Traditional
psychosurgery and the advent of deep brain stimulation." Current Opinion
in Psychiatry. Volume 22. Number 1. 25–31 Pages.
Although the individual therapies that we have discussed so far in this unit focus
primarily on the psychological and biological aspects of the bio-psycho-social model of
disorder, the social dimension is never out of the picture. Therapists understand that
disorder is caused, and potentially prevented, in large part by the people with whom we
interact. A person with schizophrenia does not live in a vacuum. He interacts with his
family members and with the other members of the community, and the behavior of those
people may influence his disease. And depression and anxiety are created primarily by
the affected individual’s perceptions (and misperceptions) of the important people
around them. Thus prevention and treatment are influenced in large part by the social
context in which the person is living.
Group, Couples, and Family Therapy
Practitioners sometimes incorporate the social setting in which disorder occurs by conducting
therapy in groups. Group therapy is psychotherapy in which clients receive psychological treatment together
with others. A professionally trained therapist guides the group,
usually between 6 and 10 participants, to create an atmosphere of support and
emotional safety for the participants. [1]
Group therapy provides a safe place where people come together to share problems
or concerns, to better understand their own situations, and to learn from and
with each other. Group therapy is often cheaper than individual therapy, as the
therapist can treat more people at the same time, but economy is only one part
of its attraction. Group therapy allows people to help each other, by sharing
ideas, problems, and solutions. It provides social support, offers the knowledge
that other people are facing and successfully coping with similar situations,
and allows group members to model the successful behaviors of other group
members. Group therapy makes explicit the idea that our interactions with others
may create, intensify, and potentially alleviate disorders.
Group therapy has met with much success in the more than 50 years it has been in
use, and it has generally been found to be as or more effective than individual
therapy. [2] Group
therapy is particularly effective for people who have life-altering illness, as
it helps them cope better with their disease, enhances the quality of their
lives, and in some cases has even been shown to help them live
longer. [3]
Sometimes group therapy is conducted with people who are in close relationships.
Couples therapy is treatment in which two people who
are cohabitating, married, or dating meet together with the practitioner to
discuss their concerns and issues about their relationship. These therapies are
in some cases educational, providing the couple with information about what is
to be expected in a relationship. The therapy may focus on such topics as sexual
enjoyment, communication, or the symptoms of one of the partners (e.g.,
depression).
Family therapy involves families meeting together with a
therapist. In some cases the meeting is precipitated by a particular problem
with one family member, such as a diagnosis of bipolar disorder in a child.
Family therapy is based on the assumption that the problem, even if it is
primarily affecting one person, is the result of an interaction among the people
in the family.
Self-Help Groups
Group therapy is based on the idea that people can be helped by the positive social
relationships that others provide. One way for people to gain this social
support is by joining a self-help group, which is a voluntary association of people who share a common desire
to overcome psychological disorder or improve their well-being. [4] Self-help groups have
been used to help individuals cope with many types of addictive behaviors. Three
of the best-known self-help groups are Alcoholics Anonymous, of which there are
more than 2 million members in the United States; Gamblers Anonymous; and
Overeaters Anonymous.
The idea behind self-help groups is similar to that of group therapy, but the groups are open
to a broader spectrum of people. As in group therapy, the benefits include
social support, education, and observational learning. Religion and spirituality
are often emphasized, and self-blame is discouraged. Regular group meetings are
held with the supervision of a trained leader.
References
- Yalom, I., and Leszcz, M.
(2005).
The Theory and Practice of Group Psychotherapy. Basic Books. New York. Edition 5.
- McDermut, W., Miller, I. W., and Brown, R. A.
(2001).
"The efficacy of group psychotherapy for depression: A
meta-analysis and review of the empirical research." Clinical
Psychology: Science and Practice. Volume 8. Number 1. 98–116 Pages.
- American Group Psychotherapy Association.
(2000).
About group psychotherapy. Retrieved from http://www.groupsinc.org/group/consumersguide2000.html.
- Humphreys, K., and Rappaport, J.
(1994).
"Researching self-help/mutual aid groups and organizations: Many
roads, one journey." Applied and Preventative Psychology. Volume 3.
Number 4. 217–231 Pages.
The social aspect of disorder is also understood and treated at the community
level. Community mental health services are psychological treatments and interventions that are
distributed at the community level. Community mental health services
are provided by nurses, psychologists, social workers, and other professionals
in sites such as schools, hospitals, police stations, drug treatment clinics,
and residential homes. The goal is to establish programs that will help people
get the mental health services that they need. [1]
Unlike traditional therapy, the primary goal of community mental health
services is prevention. Just as widespread vaccination of children has
eliminated diseases such as polio and smallpox, mental health services are
designed to prevent psychological disorder. [2] Community
prevention can be focused on one more of three levels: primary prevention,
secondary prevention, and tertiary prevention.
Primary prevention is prevention in
which all members of the community receive the treatment. Examples of
primary prevention are programs designed to encourage all pregnant women to
avoid cigarettes and alcohol because of the risk of health problems for the
fetus, and programs designed to remove dangerous lead paint from homes.
Secondary prevention is more limited
and focuses on people who are most likely to need it—those who display risk
factors for a given disorder. Risk factors are
the social, environmental, and economic vulnerabilities
that make it more likely than average that a given individual will develop a
disorder. [3] The
following presents a list of potential risk factors for psychological
disorders.
Finally, tertiary prevention is treatment, such as psychotherapy or biomedical therapy, that focuses
on people who are already diagnosed with disorder.
Some Risk Factors for Psychological Disorders
Community mental health workers practicing secondary prevention will
focus on youths with these markers of future problems.
- Academic difficulties
- Attention-deficit/hyperactivity disorder (ADHD)
- Child abuse and neglect
- Developmental disorders
- Drug and alcohol abuse
- Dysfunctional family
- Early pregnancy
- Emotional immaturity
- Homelessness
- Learning disorder
- Low birth weight
- Parental mental illness
- Poor nutrition
- Poverty
Community prevention programs are designed to provide support during
childhood or early adolescence with the hope that the interventions will
prevent disorders from appearing or will keep existing disorders from
expanding. Interventions include such things as help with housing,
counseling, group therapy, emotional regulation, job and skills training,
literacy training, social responsibility training, exercise, stress
management, rehabilitation, family therapy, or removing a child from a
stressful or dangerous home situation.
The goal of community interventions is to make it easier for individuals
to continue to live a normal life in the face of their problems.
Community mental health services are designed to make it less likely that
vulnerable populations will end up in institutions or on the streets. In
summary, their goal is to allow at-risk individuals to continue to
participate in community life by assisting them within their own
communities.
Research Focus: The Implicit Association Test as a Behavioral Marker for
Suicide
Secondary prevention focuses on people who are at risk for disorder or
for harmful behaviors. Suicide is a leading cause of death worldwide, and
prevention efforts can help people consider other alternatives,
particularly if it can be determined who is most at risk. Determining
whether a person is at risk of suicide is difficult, however, because
people are motivated to deny or conceal such thoughts to avoid
intervention or hospitalization. One recent study found that 78% of
patients who die by suicide explicitly deny suicidal thoughts in their
last verbal communications before killing
themselves. [4]
Nock and colleagues [5] tested the possibility that
implicit measures of the association between the self-concept and death
might provide a more direct behavioral marker of suicide risk that would
allow professionals to more accurately determine whether a person is
likely to commit suicide in comparison to existing self-report measures.
They measured implicit associations about death and suicide in 157 people
seeking treatment at a psychiatric emergency department.
The participants all completed a version of the Implicit Association Test
(IAT), which was designed to assess the strength of a person’s mental
associations between death and the self. [6]
Using a notebook computer, participants classified stimuli representing
the constructs of “death” (i.e., die, dead, deceased, lifeless, and
suicide) and “life” (i.e., alive, survive, live, thrive, and breathing)
and the attributes of “me” (i.e., I, myself, my, mine, and self) and “not
me” (i.e., they, them, their, theirs, and other). Response latencies for
all trials were recorded and analyzed, and the strength of each
participant’s association between “death” and “me” was calculated.
The researchers then followed participants over the next 6 months to test
whether the measured implicit association of death with self could be
used to predict future suicide attempts. The authors also tested whether
scores on the IAT would add to prediction of risk above and beyond other
measures of risk, including questionnaire and interview measures of
suicide risk. Scores on the IAT predicted suicide attempts in the next 6
months above all the other risk factors that were collected by the
hospital staff, including past history of suicide attempts. These results
suggest that measures of implicit cognition may be useful for determining
risk factors for clinical behaviors such as suicide.
References
- Gonzales, L. R., Kelly, J. G., Mowbray, C. T., Hays, R. B., and Snowden, L. R.
(2003).
The Clinical Psychology Handbook. Chapter
Community mental health. Pergamon Press. Elmsford, NY. Edition 2.
762–779 Pages. M. Hersen, A. E. Kazdin, and A. S. Bellack (Eds.).
- Institute of Medicine.
(1994).
Reducing Risks for Mental Disorders: Frontiers for Preventive Intervention Research. National Academy Press. Washington, DC.
- Werner, E. E., and Smith, R. S.
(1992).
Overcoming the Odds: High Risk Children from Birth to Adulthood. Cornell University Press. Ithaca, NY.
- Busch, K. A., Fawcett, J., and Jacobs, D. G.
(2003).
"Clinical correlates of inpatient suicide." Journal of Clinical Psychiatry. Volume 64. Number 1. 14–19 Pages.
- Nock, M. K., Park, J. M., Finn, C. T.,
Deliberto, T. L., Dour, H. J., and Banaji, M. R.
(2010).
"Measuring the suicidal mind: Implicit cognition predicts suicidal
behavior." Psychological Science. Volume 21. Number 4. 511–517 Pages.
- Greenwald, A. G., McGhee, D. E., and
Schwartz, J. L. K.
(1998).
"Measuring individual differences in implicit cognition: The
Implicit Association Test." Journal of Personality and Social
Psychology. Volume 74. Number 6. 1464–1480 Pages.
We have seen that psychologists and other practitioners employ a variety of treatments in
their attempts to reduce the negative outcomes of psychological disorders. But we have
not yet considered the important question of whether these treatments are effective, and
if they are, which approaches are most effective for which people and for which
disorders. Accurate empirical answers to these questions are important as they help
practitioners focus their efforts on the techniques that have been proven to be most
promising, and will guide societies as they make decisions about how to spend public
money to improve the quality of life of their
citizens. [1]
Psychologists use outcome research, that is, studies that assess the effectiveness of medical treatments, to determine the
effectiveness of different therapies. In these studies the independent variable is the
type of the treatment—for instance, whether it was psychological or biological in
orientation or how long it lasted. In most cases characteristics of the client (e.g.,
his or her gender, age, disease severity, and prior psychological histories) are also
collected as control variables. The dependent measure is an assessment of the benefit
received by the client. In some cases we might simply ask the client if she feels
better, and in other cases we may directly measure behavior: Can the client now get in
the airplane and take a flight? Has the client remained out of juvenile detention?
In every case the scientists evaluating the therapy must keep in mind the potential that
other effects rather than the treatment itself might be important, that some treatments
that seem effective might not be, and that some treatments might actually be harmful, at
least in the sense that money and time are spent on programs or drugs that do not
work.
One threat to the validity of outcome research studies is natural
improvement—the possibility that people might get better
over time, even without treatment. People who begin therapy or join a self-help
group do so because they are feeling bad or engaging in unhealthy behaviors. After being
in a program over a period of time, people frequently feel that they are getting better.
But it is possible that they would have improved even if they had not attended the
program, and that the program is not actually making a difference. To demonstrate that
the treatment is effective, the people who participate in it must be compared with
another group of people who do not get treatment.
Another possibility is that therapy works, but that it doesn’t really matter which type
of therapy it is. Nonspecific treatment effects occur when the patient gets better over time simply by coming to therapy,
even though it doesn’t matter what actually happens at the therapy sessions.
The idea is that therapy works, in the sense that it is better than doing nothing, but
that all therapies are pretty much equal in what they are able to accomplish. Finally,
placebo effects are improvements that occur
as a result of the expectation that one will get better rather than from the actual
effects of a treatment.
Effectiveness of Psychological Therapy
Thousands of studies have been conducted to test the effectiveness of
psychotherapy, and by and large they find evidence that it works. Some outcome
studies compare a group that gets treatment with another (control) group that
gets no treatment. For instance, Ruwaard, Broeksteeg, Schrieken, Emmelkamp, and
Lange [2] found that patients who interacted with a
therapist over a website showed more reduction in symptoms of panic disorder
than did a similar group of patients who were on a waiting list but did not get
therapy. Although studies such as this one control for the possibility of
natural improvement (the treatment group improved more than the control group,
which would not have happened if both groups had only been improving naturally
over time), they do not control for either nonspecific treatment effects or for
placebo effects. The people in the treatment group might have improved simply by
being in the therapy (nonspecific effects), or they may have improved because
they expected the treatment to help them (placebo effects).
An alternative is to compare a group that gets “real” therapy with a group that gets only a
placebo. For instance, Keller and colleagues [3] had adolescents who were experiencing anxiety
disorders take pills that they thought would reduce anxiety for 8 weeks.
However, one-half of the patients were randomly assigned to actually receive the
antianxiety drug Paxil, while the other half received a placebo drug that did
not have any medical properties. The researchers ruled out the possibility that
only placebo effects were occurring because they found that both groups improved
over the 8 weeks, but the group that received Paxil improved significantly more
than the placebo group did.
Studies that use a control group that gets no treatment or a group that gets only
a placebo are informative, but they also raise ethical questions. If the
researchers believe that their treatment is going to work, why would they
deprive some of their participants, who are in need of help, of the possibility
for improvement by putting them in a control group?
Another type of outcome study compares different approaches with each other. For
instance, Herbert and colleagues [4] tested whether social
skills training could boost the results received for the treatment of social
anxiety disorder with cognitive-behavioral therapy (CBT) alone. As you can see
in the figure below, they found that people in both groups improved, but CBT
coupled with social skills training showed significantly greater gains than CBT
alone.
Other studies [5] [6]
have compared brief sessions of psychoanalysis with longer-term psychoanalysis
in the treatment of anxiety disorder, humanistic therapy with psychodynamic
therapy in treating depression, and cognitive therapy with drug therapy in
treating anxiety. [7] [8]
These studies are advantageous because they compare the specific effects of one
type of treatment with another, while allowing all patients to get
treatment.
References
- Hunsley, J., and Di Giulio, G.
(2002).
"Dodo bird, phoenix, or urban legend? The question of psychotherapy
equivalence." Scientific Review of Mental Health Practice. Volume 1.
Number 1. 11–22 Pages.
- Ruwaard, J., Broeksteeg, J., Schrieken, B.,
Emmelkamp, P., and Lange, A.
(2010).
"Web-based therapist-assisted cognitive behavioral treatment of
panic symptoms: A randomized controlled trial with a three-year
follow-up." Journal of Anxiety Disorders. Volume 24. Number 4. 387–396
Pages.
- Keller, M. B., Ryan, N. D., Strober, M., Klein,
R. G., Kutcher, S. P., Birmaher, B., et al.
(2001).
"Efficacy of paroxetine in the treatment of adolescent major
depression: A randomized, controlled trial." Journal of the American
Academy of Child and Adolescent Psychiatry. Volume 40. Number 7. 762–772
Pages.
- Herbert, J. D., Gaudini, B. A., Rheingold, A.
A., Myers, V. H., Dalrymple, K., and Nolan, E. M.
(2005).
"Social skills training augments the effectiveness of cognitive
behavioral group therapy for social anxiety disorder." Behavior Therapy.
Volume 36. Number 2. 125–138 Pages.
- Crits-Christoph, P.
(1992).
"The efficacy of brief dynamic psychotherapy: A meta-analysis."
American Journal of Psychiatry. Volume 149. Number 2. 151–158 Pages.
- Crits-Christoph, P., Gibbons, M. B.,
Losardo, D., Narducci, J., Schamberger, M., and Gallop, R.
(2004).
"Who benefits from brief psychodynamic therapy for generalized
anxiety disorder?." Canadian Journal of Psychoanalysis. Volume 12.
Number 2. 301–324 Pages.
- Dalgleish, T.
(2004).
"Cognitive approaches to posttraumatic stress disorder: The
evolution of multirepresentational theorizing." Psychological Bulletin.
Volume 130. Number 2. 228–260 Pages.
- Hollon, S. D., Thase, M. E., and Markowitz, J. C.
(2002).
"Treatment and prevention of depression." Psychological Science in the Public Interest. Volume 3. Number 1. 39–77 Pages.
Because there are thousands of studies testing the effectiveness of
psychotherapy, and the independent and dependent variables in the studies vary
widely, the results are often combined using a meta-analysis. A meta-analysis is a statistical technique that uses the results of existing
studies to integrate and draw conclusions about those studies. In one
important meta-analysis analyzing the effect of psychotherapy, Smith, Glass, and
Miller [1] summarized studies that compared different types of
therapy or that compared the effectiveness of therapy against a control group.
To find the studies, the researchers systematically searched computer databases
and the reference sections of previous research reports to locate every study
that met the inclusion criteria. Over 475 studies were located, and these
studies used over 10,000 research participants.
The results of each of these studies were systematically coded, and a measure of
the effectiveness of treatment known as the effect size
was created for each study. Smith and her colleagues found that the average
effect size for the influence of therapy was 0.85, indicating that psychotherapy
had a relatively large positive effect on recovery. What this means is that,
overall, receiving psychotherapy for behavioral problems is substantially better
for the individual than not receiving therapy as shown in the following figure. Although they did not measure it,
psychotherapy presumably has large societal benefits as well—the cost of the
therapy is likely more than made up for by the increased productivity of those
who receive it.
Other meta-analyses have also found substantial support for the effectiveness of
specific therapies, including cognitive therapy, CBT, [2] [3] couples and
family therapy, [4] and psychoanalysis. [5]
On the basis of these and other meta-analyses,
a list of bold—that is,
therapies that are known to be effective—has been developed. [6] [7] These
therapies include cognitive therapy and behavioral therapy for depression;
cognitive therapy, exposure therapy, and stress inoculation training for
anxiety; CBT for bulimia; and behavior modification for bed-wetting.
Smith, Glass, and Miller [1] did not find
much evidence that any one type of therapy was more effective than any other
type, and more recent meta-analyses have not tended to find many differences
either. [8]
What this means is that a good part of the effect of therapy is nonspecific, in
the sense that simply coming to any type of therapy is helpful in comparison to
not coming. This is true partly because there are fewer distinctions among the
ways that different therapies are practiced than the theoretical differences
among them would suggest. What a good therapist practicing psychodynamic
approaches does in therapy is often not much different from what a humanist or a
cognitive-behavioral therapist does, and so no one approach is really likely to
be better than the other.
What all good therapies have in common is that they give people hope; help them
think more carefully about themselves and about their relationships with others;
and provide a positive, empathic, and trusting relationship with the
therapist—the therapeutic alliance. [9]
This is why many self-help groups are also likely to be effective and perhaps
why having a psychiatric service dog may also make us feel better.
References
- Smith, M. L., Glass, G. V., and Miller, R. L.
(1980).
The Benefits of Psychotherapy. Johns Hopkins University Press. Baltimore.
- Butler A. C., Chapman, J. E., Forman, E. M.,
Beck, A. T.
(2006).
"The empirical status of cognitive-behavioral therapy: A review of
meta-analyses." Clinical Psychology Review. Volume 26. Number 1. 17–31
Pages.
- Deacon, B. J., and Abramowitz, J. S.
(2004).
"Cognitive and behavioral treatments for anxiety disorders: A
review of meta-analytic findings." Journal of Clinical Psychology.
Volume 60. Number 4. 429–441 Pages.
- Shadish, W. R., and Baldwin, S. A.
(2002).
Effectiveness Research in Marriage and Family Therapy.
Chapter Meta-analysis of MFT interventions. American Association for
Marriage and Family Therapy. Alexandria, VA. 339–370 Pages. D. H.
Sprenkle (Ed.).
- Shedler, J.
(2010).
"The efficacy of psychodynamic psychotherapy." American Psychologist. Volume 65. Number 2. 98–109 Pages.
- Chambless, D. L., and Hollon, S. D.
(1998).
"Defining empirically supported therapies." Journal of Consulting
and Clinical Psychology. Volume 66. Number 1. 7–18 Pages.
- Hollon, S., Stewart, M., and Strunk, D.
(2006).
"Enduring effects for cognitive therapy in the treatment of
depression and anxiety." Annual Review of Psychology. Volume 57. Number
1. 285–316 Pages.
- Cuijpers, P., van Straten, A., Andersson, G.,
and van Oppen, P.
(2008).
"Psychotherapy for depression in adults: A meta-analysis of
comparative outcome studies." Journal of Consulting and Clinical
Psychology. Volume 76. Number 6. 909–922 Pages.
- CuijAhn, H.-N., and Wampold, B. E.
(2001).
"Where oh where are the specific ingredients? A meta-analysis of
component studies in counseling and psychotherapy." Journal of
Counseling Psychology. Volume 48. Number 3. 261–257 Pages.
Effectiveness of Biomedical Therapies
Although there are fewer of them because fewer studies have been
conducted, meta-analyses also support the effectiveness of drug therapies
for psychological disorder. For instance, the use of psychostimulants to
reduce the symptoms of attention-deficit/hyperactivity disorder (ADHD) is
well known to be successful, and many studies find that the positive and
negative symptoms of schizophrenia are substantially reduced by the use
of antipsychotic medications. [1]
People who take antidepressants for mood disorders or antianxiety
medications for anxiety disorders almost always report feeling better,
although drugs are less helpful for phobic disorder and
obsessive-compulsive disorder. Some of these improvements are almost
certainly the result of placebo effects, [2] but
the medications do work, at least in the short term. An analysis of U.S.
Food and Drug Administration databases found effect sizes of 0.26 for
Prozac, 0.26 for Zoloft, 0.24 for Celexa, 0.31 for Lexapro, and 0.30 for
Cymbalta. The overall average effect size for antidepressant medications
approved by the FDA between 1987 and 2004 was 0.31. [3] [4]
One problem with drug therapies is that although they provide temporary
relief, they don’t treat the underlying cause of the disorder. Once the
patient stops taking the drug, the symptoms often return in full force.
In addition many drugs have negative side effects, and some also have the
potential for addiction and abuse. Different people have different
reactions, and all drugs carry warning labels. As a result, although
these drugs are frequently prescribed, doctors attempt to prescribe the
lowest doses possible for the shortest possible periods of time.
Older patients face special difficulties when they take medications for
mental illness. Older people are more sensitive to drugs, and drug
interactions are more likely because older patients tend to take a
variety of different drugs every day. They are more likely to forget to
take their pills, to take too many or too few, or to mix them up due to
poor eyesight or faulty memory.
Like all types of drugs, medications used in the treatment of mental
illnesses can carry risks to an unborn infant. Tranquilizers should not
be taken by women who are pregnant or expecting to become pregnant,
because they may cause birth defects or other infant problems, especially
if taken during the first trimester. Some selective serotonin reuptake
inhibitors (SSRIs) may also increase risks to the
fetus, [5] [6]
as do
antipsychotics. [7]
Decisions on medication should be carefully weighed and based on each
person’s needs and circumstances. Medications should be selected based on
available scientific research, and they should be prescribed at the
lowest possible dose. All people must be monitored closely while they are
on medications.
Effectiveness of Social-Community Approaches
Measuring the effectiveness of community action approaches to mental
health is difficult because they occur in community settings and impact a
wide variety of people, and it is difficult to find and assess valid
outcome measures. Nevertheless, research has found that a variety of
community interventions can be effective in preventing a variety of
psychological disorders. [8]
Data suggest that federally funded prevention programs such as the Special Supplemental Program for Women, Infants, and
Children (WIC), which provides federal grants to states for
supplemental foods, health-care referral, and nutrition education for
low-income women and their children, are successful. WIC mothers have
higher birth weight babies and lower infant mortality than other
low-income mothers. [9] And
the average blood-lead levels among children have fallen approximately
80% since the late 1970s as a result of federal legislation designed to
remove lead paint from housing. [10]
Although some of the many community-based programs designed to reduce alcohol,
tobacco, and drug abuse; violence and delinquency; and mental illness have been
successful, the changes brought about by even the best of these programs are, on
average, modest. [11] [12]
This does not necessarily mean that the programs are not useful. What is important is
that community members continue to work with researchers to help determine which
aspects of which programs are most effective and to concentrate efforts on the most
productive approaches. [13] The most
beneficial preventive interventions for young people involve coordinated, systemic
efforts to enhance their social and emotional competence and health. Many
psychologists continue to work to promote policies that support community prevention
as a model of preventing disorder.
References
- Lieberman, J., Stroup, T., McEvoy, J., Swartz,
M., Rosenheck, R., Perkins, D., et al.
(2005).
"Effectiveness of antipsychotic drugs in patients with chronic
schizophrenia." New England Journal of Medicine. Volume 353. Number 12.
1209–1223 Pages.
- Cardeña, E., and Kirsch, I.
(2000).
"True or false: The placebo effect as seen in drug studies is
definitive proof that the mind can bring about clinically relevant
changes in the body: What is so special about the placebo effect?."
Advances in Mind-Body Medicine. Volume 16. Number 1. 16–18 Pages.
- Deshauer, D., Moher, D., Fergusson, D.,
Moher, E., Sampson, M., and Grimshaw, J.
(2008).
"Selective serotonin reuptake inhibitors for unipolar depression: A
systematic review of classic long-term randomized controlled trials."
Canadian Medical Association Journal. Volume 178. Number 10. 1293–1301
Pages.
- Turner, E. H., Matthews, A. M., Linardatos,
E., Tell, R. A., and Rosenthal, R.
(2008).
"Selective publication of antidepressant trials and its influence
on apparent efficacy." New England Journal of Medicine. Volume 358.
Number 3. 252–260 Pages.
- Louik, C., Lin, A. E., Werler M. M.,
Hernandez, S., and Mitchell, A. A.
(2007).
"First-trimester use of selective serotonin-reuptake inhibitors and
the risk of birth defects." New England Journal of Medicine. Volume
356. Number 26. 2675–2683 Pages.
- U.S. Food and Drug Administration.
(2004).
FDA Medwatch drug alert on Effexor and SSRIs. Retrieved from http://www.fda.gov/medwatch/safety/2004/safety04.htm#effexor.
- Diav-Citrin, O., Shechtman, S., Ornoy,
S., Arnon, J., Schaefer, C., Garbis, H., et al.
(2005).
"Safety of haloperidol and penfluridol in pregnancy: A multicenter,
prospective, controlled study." Journal of Clinical Psychiatry. Volume
66. Number 3. 317–322 Pages.
- Price, R. H., Cowen, E. L., Lorion, R. P., and Ramos-McKay, J. (Eds.).
(1988).
Fourteen Ounces of Prevention: A Casebook for Practitioners. American Psychological Association. Washington, DC.
- Ripple, C. H., and Zigler, E.
(2003).
"Research, policy, and the federal role in prevention initiatives
for children." American Psychologist. Volume 58. Number 6–7. 482–490
Pages.
- Centers for Disease Control and Prevention.
(2000).
"Blood lead levels in young children: United States and selected
states, 1996–1999." Morbidity and Mortality Weekly Report. Volume 48.
Number 50. 1133–1137 Pages.
- Wandersman, A., and Florin, P.
(2003).
"Community interventions and effective prevention." American Psychologist. Volume 58. Number 6–7. 441–448 Pages.
- Wilson, D. B., Gottfredson, D. C., and
Najaka, S. S.
(2001).
"School-based prevention of problem behaviors: A meta-analysis."
Journal of Quantitative Criminology. Volume 17. Number 3. 247–272 Pages.
- Weissberg, R. P., Kumpfer, K. L., and
Seligman, M. E. P.
(2003).
"Prevention that works for children and youth: An introduction."
American Psychologist. Volume 58. Number 6–7. 425–432 Pages.
Please begin this unit on consciousness by watching the following video. It
features Darren Brown, an English illusionist, mentalist, and professional
skeptic.
Mentalism is a type of performing art in which the performer appears to read the mind of
another. Such powers may seem to be the result of psychic or paranormal practices, but in
reality is the result of a combination of suggestion, misdirection, and psychology. Darren
Brown himself claims no supernatural ability and often denounces those who do. As you
witnessed at the end of the video, Darren Brown was able to strongly influence the behavior
of the advertisers without their being aware that they had been manipulated. Although the
advertisers had been shown all of the stimuli that later made it into what they thought was
their original art piece, it did not register in their conscious awareness.
Consciousness is defined as our subjective awareness of
ourselves and our environment. [1] The experience
of consciousness is fundamental to human nature. We all know what it means to be conscious,
and we assume (although we can never be sure) that others experience their consciousness
similarly to how we experience ours.
The study of consciousness has long been important to psychologists and plays a role in
many important psychological theories. For instance, Sigmund Freud’s personality theories
differentiated between the unconscious and the conscious aspects of behavior. According to
Freud, our unconscious mind could influence conscious aspects of our behaviors. Some
examples he gave included memory repression, phobias, denial, and "Freudian slips."
Present-day psychologists distinguish between automatic
(unconscious, or autonomic) and controlled
(conscious) behaviors and between implicit (unconscious) and explicit (conscious) memory. [2] [3]
learn by doing
There are some useful distinctions between the terms we just introduced. Let’s take a
brief look at them.
Some philosophies and religions argue that the mind (or soul) and the
body are separate entities, a concept called dualism.
However, most psychologists agree that consciousness and the mind are
biologically based and exist within the brain, a concept called monism.
The differences between monism and dualism may seem subtle, but these distinctions are
extremely important for the study of psychology. Put simply, in order to study psychology
experimentally, we must assume that conscious behaviors are the result of, and are not
separate from, the physical brain. Fields such as cognitive neuroscience, which looks to
correlate brain activity to behavior through the use of functional brain imaging, require
the assumption that monism is true. After all, it makes little sense to look at the brain
to study memory, learning, and other behaviors if those behaviors actually arise from a
nonmaterial source separate from the brain itself. So remember, although either side can be
argued for in a philosophical debate, we must assume that monism is correct in the study of
psychology.
The study of consciousness is also important to the fundamental psychological question
regarding the presence of free will. Although we may understand and believe that some of
our behaviors are caused by forces outside our awareness (i.e., unconscious), we
nevertheless believe we have control over the behaviors we engage in. It is possible,
however, for an individual to engage in a complex behavior, such as driving a car and
causing an accident, without being at all conscious of his or her actions. Although such
events are rare and even shocking, psychologists are increasingly certain that a great deal
of our behavior is caused by processes of which we are unaware and over which we have
little or no control. [4] [5]
Our experience of consciousness is functional because we use it to guide and control our
behavior and to think logically about
problems. [6] Consciousness
allows us to plan activities and to monitor our progress toward the goals we set for
ourselves. In addition, consciousness is fundamental to our sense of morality—we believe we
have the free will to perform moral actions while avoiding immoral behaviors.
On the other hand, consciousness may become aversive. For instance, negative emotional
reactions occur when we are not living up to our anticipated goals or expectations or when
we believe that other people perceive us negatively. In these cases, we may engage in
maladaptive behaviors, such as the use of alcohol or other psychoactive drugs, to escape
from consciousness. [7]
Because the brain varies in its current level and type of activity,
consciousness is transitory. For instance, if we drink too much coffee or beer,
the caffeine or alcohol influences the activity in our brain. Consequently, our
consciousness may change. Being anesthetized before an operation or
experiencing a concussion after a knock on the head may result in loss of
consciousness, which also alters brain activity. We also lose consciousness
when we sleep, and it is with this altered state of consciousness that we begin
our unit.
References
- Koch, C.
(2004).
The Quest for Consciousness: A Neurobiological Approach. Roberts. Englewood, CO.
- Petty, R., Wegener, D., Chaiken, S., and Trope, Y.
(1999).
Dual-Process Theories in Social Psychology. Guilford Press. New York.
- Shanks, D.
(2005).
Handbook of Cognition. Chapter Implicit learning. Sage. London, England. 202–220 Pages. K. Lamberts (Ed.).
- Libet, B.
(1999).
"Do we have free will?." Journal of Consciousness Studies. Volume 6. Number 8/9. 47–57 Pages.
- Wegner, D. M.
(2003).
"The mind’s best trick: How we experience conscious will." Trends
in Cognitive Sciences. Volume 7. Number 2. 65–69 Pages.
- DeWall, C., Baumeister, R., and Masicampo, E.
(2008).
"Evidence that logical reasoning depends on conscious processing."
Consciousness and Cognition. Volume 17. Number 3. 628–645 Pages.
- Baumeister, R.
(1998).
The Handbook of Social Psychology, Vol. 2. Chapter The self. McGraw-Hill. New York. Edition 4. 680–740 Pages. D. T. Gilbert, S. T. Fiske, and G. Lindzey (Eds.).
The lives of all organisms, including humans, are influenced by regularly occurring cycles of behaviors known as
biological rhythms. One important biological rhythm is the daily circadian
rhythm (from the Latin circa, meaning “about” or
“approximately,” and dian, meaning “daily”) that guides
the daily waking and sleeping cycle in many animals, including humans.
Sleep is influenced by ambient light. The ganglion cells in the retina send
signals to a brain area above the thalamus called the suprachiasmatic nucleus, which is the body’s primary circadian
“pacemaker.” The suprachiasmatic nucleus analyzes the strength and duration of
the light stimulus and sends signals to the pineal gland when the ambient light
level is low or its duration is short. In response, the pineal gland secretes
melatonin, a powerful hormone that facilitates the
onset of sleep.
Although our conscious state changes as we sleep, the brain nevertheless remains active.
The patterns of sleep have been tracked in thousands of research participants who have
spent nights sleeping in research labs while their brain waves were recorded by monitors,
such as an electroencephalogram, or EEG.
Sleep researchers have found that sleeping people undergo a fairly consistent pattern of
sleep stages, each lasting about 90 minutes. Although you might not be aware of it, you go
through cycles of sleep, or different stages of sleep as the night progresses. Each sleep
stage has its own distinct pattern of brain activity. [1] As you can see in the following
figure, these stages are of two major types: rapid eye
movement (REM) sleep (dreaming) and slow-wave sleep (deep sleep). People seem to need an
adequate amount of sleep as well as a certain amount of REM and slow-wave sleep each night
in order to feel rested. Slow-wave sleep is part of a larger sleep type known as NREM
(non-REM) sleep, which is often divided into three stages: N1, N2, and N3.
During REM sleep, our awareness of external events is dramatically reduced, and
consciousness is dominated primarily by internally generated images and a lack
of overt thinking. [2]
As you can see in the following
figure, the brain waves
recorded by an EEG as we sleep show that the brain’s activity changes during each stage of
sleeping. When we are awake, our brain activity is characterized by the presence of very
fast beta waves. When we first begin to fall asleep, the waves get
longer (alpha waves), and as we move into stage N1 sleep,
characterized by drowsiness, the brain begins to produce even slower theta waves. During stage N1 sleep, some muscle tone is lost, as well as most
awareness of the environment. Some people may experience sudden jerks or twitches and even
vivid hallucinations during this initial stage of sleep.
Normally, if we are allowed to keep sleeping, we move from stage N1 to stage N2 sleep.
During stage N2, muscular activity is further decreased and conscious awareness of the
environment is lost. This stage typically represents about half of the total sleep time in
normal adults. Stage N2 sleep is characterized by theta waves interspersed with bursts of
rapid brain activity known as sleep spindles.
Stage N3, also known as slow-wave sleep, is the deepest level of
sleep, characterized by an increased proportion of very slow delta
waves. This is the stage in which most sleep abnormalities, such as sleepwalking,
sleeptalking, nightmares, and bedwetting occur. Some skeletal muscle tone remains, making
it possible for affected individuals to rise from their beds and engage in sometimes very
complex behaviors, but consciousness is distant. Even in the deepest sleep, however, we are
still aware of the external world. If smoke enters the room or if we hear the cry of a
baby, we are likely to react even though we are sound asleep. These occurrences demonstrate
the extent to which we process information outside consciousness.
After falling initially into a very deep sleep, the brain begins to become more active
again, and we normally move into the first period of REM sleep about 90 minutes after
falling asleep. REM sleep is accompanied by an increase in heart rate, facial twitches, and
the repeated rapid eye movements that give this stage its name. People who are awakened
during REM sleep almost always report that they were dreaming, while those awakened in
other stages of sleep report dreams much less often. REM sleep is also emotional sleep.
Activity in the limbic system, including the amygdala, is increased during REM sleep, and
the genitals become aroused even if the content of the dreams we are having is not sexual.
A typical 25-year-old man may have an erection nearly half of the night, and the common
“morning erection” is left over from the last REM period before waking.
Normally, we go through several cycles of REM and NREM sleep each
night. The
length of the REM portion of the cycle tends to increase through the night, from about 5 to
10 minutes early in the night to 15 to 20 minutes shortly before awakening in the morning.
Dreams also tend to become more elaborate and vivid as the night goes on. Eventually, as
the sleep cycle finishes, the brain resumes its faster alpha and beta waves and we awake,
normally refreshed.
References
- Dement, W., and Kleitman, N.
(1957).
"Cyclic variations in EEG during sleep and their relation to eye
movements, body motility, and dreaming." Electroencephalography and
Clinical Neurophysiology. Volume 9. Number 4. 673–690 Pages.
- Hobson, A.
(2004).
"A model for madness? Dream consciousness: Our understanding of the
neurobiology of sleep offers insight into abnormalities in the waking
brain." Nature. Volume 430. Number 1. 69–95 Pages.
According to a recent poll, [1] about
one-fourth of American adults say they get a good night’s sleep only a few nights a month
or less. These people are suffering from a sleep disorder known as insomnia, defined as persistent difficulty falling or staying
asleep. Insomnia can be caused by a wide range of things, from physical and
psychological illness to simply staying out later than usual on the weekend.
Sometimes the sleep that the insomniac does get is disturbed and
nonrestorative, and the lack of quality sleep produces impairment of
functioning during the day. Ironically, the problem may be compounded by
people’s anxiety over insomnia itself: Their fear of being unable to sleep may
wind up keeping them awake. Some people may also develop a conditioned anxiety
to the bedroom or the bed.
People who have difficulty sleeping may turn to drugs to help them sleep. Barbiturates,
benzodiazepines, and other sedatives are frequently marketed and prescribed as sleep aids,
but they may interrupt the natural stages of the sleep cycle and ultimately are likely to
do more harm than good. In some cases, they may also promote dependence.
Another common sleep problem is sleep apnea, a
sleep disorder characterized by pauses in breathing that last at least 10 seconds during
sleep. [2]
In addition to preventing restorative sleep, sleep apnea can cause high blood pressure and
may raise the risk of stroke and heart attack. [3] Most sleep apnea is caused by an obstruction
of the walls of the throat that occurs when we fall asleep. It is most common in obese or
older individuals who have lost muscle tone and is particularly common in men. Sleep apnea
caused by obstructions is usually treated with an air machine that uses a mask to create a
continuous pressure that prevents the airway from collapsing or with a mouthpiece that keep
the airway open. If all other treatments have failed, sleep apnea may be treated with
surgery to open the airway.
Narcolepsy is a disorder characterized by extreme
daytime sleepiness with frequent episodes of “nodding off.” The syndrome may also
be accompanied by attacks of cataplexy in which the individual
loses muscle tone, resulting in a partial or complete collapse. It is estimated that at
least 200,000 Americans suffer from narcolepsy, although only about a quarter of these
people have been diagnosed. [4]
Narcolepsy is in
part the result of genetics—people who suffer from the disease lack neurotransmitters that
are important in keeping us
alert [5] —and in part the result
of a lack of deep sleep. While most people descend through the sequence of sleep stages,
then move back up to REM sleep soon after falling asleep, narcolepsy sufferers move
directly into REM and undergo numerous awakenings during the night, often preventing them
from getting good sleep.
Narcolepsy can be treated with stimulants, such as amphetamines, to counteract the daytime
sleepiness, or with antidepressants to treat a presumed underlying depression. However,
since these drugs further disrupt already abnormal sleep cycles, these approaches may, in
the long run, make the problem worse. Many sufferers find relief by taking a number of
planned short naps during the day, and some individuals may find it easier to work in jobs
that allow them to sleep during the day and work at night.
Other sleep disorders occur when cognitive or motor processes that should be turned off or
reduced in magnitude during sleep operate at higher than normal
levels. [6] One example is somnamulism (sleepwalking), in which the person leaves the bed and
moves around while still asleep. Sleepwalking is more common in childhood, with the most
frequent occurrences around the age of 12 years. About 4% of adults experience
somnambulism. [6]
Sleep terrors is a disruptive sleep disorder, most
frequently experienced in childhood, that may involve loud screams and intense
panic. The sufferer cannot wake from sleep even though he or she is trying to.
In extreme cases, sleep terrors may result in bodily harm or property damage as
the sufferer moves about abruptly. Up to 3% of adults suffer from sleep
terrors, which typically occur in sleep stage
N3. [6]
Other sleep disorders include bruxism, in which the sufferer grinds
his teeth during sleep; restless legs syndrome, in which the
sufferer reports an itching, burning, or otherwise uncomfortable feeling in his or her
legs, usually exacerbated when resting or asleep; and periodic limb
movement disorder, which involves sudden involuntary movement of limbs. The latter
can cause sleep disruption and injury for both the sufferer and bed partner.
Although many sleep disorders occur during non-REM sleep, REM sleep behavior disorder [6] is a condition in which
people (usually middle-aged or older men) engage in vigorous and bizarre
physical activities during REM sleep in response to intense, violent dreams. As
their actions may injure themselves or their sleeping partners, this disorder,
thought to be neurological in nature, is normally treated with medications.
References
- National Sleep Foundation.
(2009).
Sleep in America Poll. Retrieved from http://www.sleepfoundation.org/sites/default/files/2009%20Sleep%20in%20America%20SOF%20EMBARGOED.pdf.
- Morgenthaler, T. I., Kagramanov, V., Hanak, V., and Decker, P. A.
(2006).
"Complex sleep apnea syndrome: Is it a unique clinical syndrome?." Sleep. Volume 29. Number 9. 1203–1209 Pages.
- Yaggi, H. K., Concato, J., Kernan, W. N.,
Lichtman, J. H., Brass, L. M., and Mohsenin, V.
(2005).
"Obstructive sleep apnea as a risk factor for stroke and death."
New England Journal of Medicine. Volume 353. Number 19. 2034–2041 Pages.
- National Heart, Lung, and Blood Institute.
(2008).
Who is at risk for narcolepsy?. Retrieved from http://www.nhlbi.nih.gov/health/dci/Diseases/nar/nar_who.html.
- Taheri, S., Zeitzer, J. M., and Mignot, E.
(2002).
"The role of hypocretins (Orexins) in sleep regulation and
narcolepsy." Annual Review of Neuroscience. Volume 25. Number 3. 283–313
Pages.
- Mahowald, M., and Schenck, C.
(2000).
Principles and Practice of Sleep Medicine.
Chapter REM sleep parasomnias. Saunders. Philadelphia. Edition 3.
724–741 Pages. W. C. Dement, T. Roth, and M. H. Kryger (Eds.).
We already discussed actions you can take if you have trouble sleeping, but how much sleep
do you really need?
Our preferred sleep times and our sleep requirements vary throughout our life cycle.
Newborns tend to sleep between 16 and 18 hours per day, preschoolers tend to sleep between
10 and 12 hours per day, school-aged children and teenagers usually prefer at least 9 hours
of sleep per night, and most adults say they require 7 to 8 hours per
night. [1] [2]
There are also individual differences in need for sleep. Some people do quite well with
fewer than 6 hours of sleep per night, whereas others need 9 hours or more. Studies suggest
that adults should get between 7 and 9 hours of sleep per night, and yet Americans now
average fewer than 7 hours. In fact, the most recent research by the National Sleep
Foundation found that the average U.S. adult reported getting only 6.7 hours of sleep per
night, which is less than the recommended range propose by the National Sleep
Foundation. [2]
Getting needed rest is difficult in part because school and work schedules
still follow the early-to-rise timetable that was set years ago. We tend to
stay up late to enjoy activities in the evening but then are forced to get up
early to go to work or school. The situation is particularly bad for college
students, who are likely to combine a heavy academic schedule with an active
social life and who may, in some cases, also work. Getting enough sleep is a
luxury that many of us seem to be unable or unwilling to afford, and yet
sleeping is one of the most important things we can do for ourselves. Continued
over time, a nightly deficit of even only 1 or 2 hours can have a substantial
impact on mood and performance.
Sleep has a vital restorative function, and a prolonged lack of sleep results in increased
anxiety, diminished performance, and, if severe and extended, may even result in death.
Many road accidents involve sleep deprivation, and people who are sleep deprived show
decrements in driving performance similar to those who have ingested
alcohol. [3] [4]
Poor treatment by doctors [5]
and a variety
of industrial accidents have also been traced in part to the effects of sleep
deprivation.
learn by doing
In 1964, 17-year-old high school student Randy Gardner remained awake for 264 hours
(11 days) in order to set a new Guinness World Record. At the request of his worried
parents, he was monitored by a U.S. Navy psychiatrist, Lieutenant Commander John J.
Ross. This chart maps the progression of his behavioral changes over the 11
days. [6]
Good sleep is also important to our health and longevity. It is no surprise that we sleep
more when we are sick, because sleep works to fight infection. Sleep deprivation suppresses
immune responses that fight off infection, and it can lead to obesity, hypertension, and
memory impairment. [7] [8] Sleeping well can even save
our lives. Dew and colleagues [9] found
that older adults who had better sleep patterns also lived longer.
References
- Mercer, P., Merritt, S., and Cowell, J.
(1998).
"Differences in reported sleep need among adolescents." Journal of
Adolescent Health. Volume 23. Number 5. 259–263 Pages.
- National Sleep Foundation.
(2008).
Sleep in America poll. Retrieved from http://www.sleepfoundation.org/sites/default/files/2008%20POLL%20SOF.PDF.
- Hack, M. A., Choi, S. J., Vijayapalan, P.,
Davies, R. J. O., and Stradling, J. R. S.
(2001).
"Comparison of the effects of sleep deprivation, alcohol and
obstructive sleep apnoea (OSA) on simulated steering performance."
Respiratory Medicine. Volume 95. Number 7. 594–601 Pages.
- Williamson, A., and Feyer, A.
(2000).
"Moderate sleep deprivation produces impairments in cognitive and
motor performance equivalent to legally prescribed levels of alcohol
intoxication." Occupational and Environmental Medicine. Volume 57.
Number 10. 649–655 Pages.
- Smith-Coggins, R., Rosekind, M. R.,
Hurd, S., and Buccino, K. R.
(1994).
"Relationship of day versus night sleep to physician performance
and mood." Annals of Emergency Medicine. Volume 24. Number 5. 928–934
Pages.
- Ross, J. J.
(1965).
"Neurological findings after prolonged sleep deprivation." Archives of Neurology. Volume 12. Number 4. 399–403 Pages.
- Ferrie, J. E., Shipley, M. J., Cappuccio, F.
P., Brunner, E., Miller, M. A., Kumari, M., and Marmot, M. G.
(2007).
"A prospective study of change in sleep duration: Associations with
mortality in the Whitehall II cohort." Sleep. Volume 30. Number 12.
1659–1666 Pages.
- Kushida, C.
(2005).
Sleep Deprivation: Basic Science, Physiology, and Behavior. Informa Healthcare. London.
- Dew, M. A., Hoch, C. C., Buysse, D. J., Monk, T.
H., Begley, A. E., Houck, P. R., et al.
(2003).
"Healthy older adults’ sleep predicts all-cause mortality at 4 to
19 years of follow-up." Psychosomatic Medicine. Volume 65. Number 1.
63–73 Pages.
Dreams are the succession of images, thoughts, sounds, and emotions
that passes through our minds while we sleep. When people are awakened from REM
sleep, they usually report that they have been dreaming, suggesting that people normally
dream several times a night but that most dreams are forgotten on
awakening. [1] The content of our dreams
generally relates to our everyday experiences and concerns and frequently to our fears
and
failures. [2] [3]
Many cultures regard dreams as having great significance for the dreamer, either by
revealing something important about the dreamer’s present circumstances or predicting
his or her future. The Austrian psychologist Sigmund Freud [4] analyzed the dreams of his patients to help him
understand their unconscious needs and desires, and psychotherapists still make use of
this technique today. Freud believed that the primary function of dreams was wish fulfillment, or the idea that dreaming allows us to act out
the desires that we must repress during the day. He differentiated between the manifest content of the dream (i.e., its literal actions) and
its latent content (i.e., the hidden psychological meaning of
the dream). Freud believed that the real meaning of dreams is often suppressed by the
unconscious mind in order to protect the individual from thoughts and feelings that are
hard to cope with. By uncovering the real meaning of dreams through psychoanalysis, Freud believed that people could better understand their
problems and resolve the issues that create difficulties in their lives.
Although Freud and others have focused on the meaning of dreams, other theories about the
causes of dreams are less concerned with their content. One possibility is that we dream
primarily to help with consolidation, or the moving of information into long-term
memory. [5] [6] Rauchs, Desgranges,
Foret, and Eustache [7]
found that rats that had been deprived of REM sleep after
learning a new task were less able to perform the task again later than were rats that
had been allowed to dream, and these differences were greater on tasks that involved
learning unusual information or developing new behaviors. Payne and Nadel [8] argued that the content of dreams
is the result of consolidation—we dream about the things that are being moved into
long-term memory. Thus dreaming may be an important part of the learning that we do
while sleeping. [9]
The activation-synthesis theory of dreaming [10] [11] proposes still
another explanation for dreaming: that dreams are our brain’s interpretation of the
random firing of neurons in the brain stem. According to this approach, the signals from
the brain stem are sent to the cortex, just as they are when we are awake, but because
the pathways from the cortex to skeletal muscles are disconnected during REM sleep, the
cortex does not know how to interpret the signals. As a result, the cortex strings the
messages together into the coherent stories we experience as dreams.
Although researchers are still trying to determine the exact causes of dreaming, one
thing remains clear—we need to dream. If we are deprived of REM sleep, we quickly become
less able to engage in the important tasks of everyday life, until we are finally able
to dream again.
References
- Dement, W.
(1997).
What all undergraduates should know about how their sleeping lives affect their waking lives. Sleepless at Stanford. Retrieved from http://www.Stanford.edu/~dement/sleepless.html.
- Cartwright, R., Agargun, M., Kirkby, J., and Friedman, J.
(2006).
"Relation of dreams to waking concerns." Psychiatry Research. Volume 141. Number 3. 261–270 Pages.
- Domhoff, G. W., Meyer-Gomes, K., and
Schredl, M.
(2005).
"Dreams as the expression of conceptions and concerns: A comparison
of German and American college students." Imagination, Cognition and
Personality. Volume 25. Number 3. 269–282 Pages.
- Freud, S., and Classics of Medicine Library.
(1988).
The Interpretation of Dreams. Classics of Medicine Library. Birmingham, AL. Edition Special. Original work published 1913.
- Alvarenga, T. A., Patti, C. L.,
Andersen, M. L., Silva, R. H., Calzavara, M. B., Lopez, G.B., et al.
(2008).
"Paradoxical sleep deprivation impairs acquisition, consolidation
and retrieval of a discriminative avoidance task in rats." Neurobiology
of Learning and Memory. Volume 90. Number 4. 624–632 Pages.
- Zhang, J.
(2004).
"Memory process and the function of sleep." Journal of Theoretics. Volume 6. Number 6. 1–7 Pages.
- Rauchs, G., Desgranges, B., Foret, J., and
Eustache, F.
(2005).
"The relationships between memory systems and sleep stages."
Journal of Sleep Research. Volume 14. Number 2. 123–140 Pages.
- Payne, J., and Nadel, L.
(2004).
"Sleep, dreams, and memory consolidation: The role of the stress
hormone cortisol." Learning and Memory. Volume 11. Number 6. 671–678
Pages.
- Hobson, J. A., Pace-Schott, E. F., and
Stickgold, R.
(2000).
"Dreaming and the brain: Toward a cognitive neuroscience of
conscious states." Behavioral and Brain Sciences. Volume 23. Number 6.
793–842 Pages.
- Hobson, J. A., and McCarley, R.
(1977).
"The brain as a dream state generator: An activation-synthesis
hypothesis of the dream process." American Journal of Psychiatry. Volume
134. Number 12. 1335–1348 Pages.
- Hobson, J. A.
(2004).
Dreams Freud Never Had: A New Mind Science. Pi Press. New York.
A psychoactive drug is a chemical that changes our states of
consciousness, and particularly our perceptions and moods. This includes
over-the-counter drugs as well as prescription drugs and those that are taken illegally for
recreational purposes. It is important to remember that psychoactive drugs can include
things that we do not typically associate with drug use, such as certain materials found in
everyday foods and beverages. While we typically use the word drug
to refer to illegal substances and medication, it can be used to describe all chemicals
that change our state of consciousness, perceptions, and mood. The four primary classes of
psychoactive drugs are stimulants, depressants, opioids, and hallucinogens.
Psychoactive drugs affect consciousness by influencing how neurotransmitters operate at the
synapses of the central nervous system (CNS). Some psychoactive drugs are agonists, which
mimic the operation of a neurotransmitter; some are antagonists, which block the action of
a neurotransmitter; and some work by blocking the reuptake of neurotransmitters at the
synapse.
In some cases, the effects of psychoactive drugs mimic other naturally occurring states of
consciousness. For instance, sleeping pills are prescribed to create drowsiness, and
benzodiazepines are prescribed to create a state of relaxation. In other cases,
psychoactive drugs are taken for recreational purposes with the goal of creating
pleasurable states of consciousness or of escaping our normal consciousness.
The use of psychoactive drugs, especially illegal drugs, has the potential to create very
negative side effects. This does not mean
that all drugs are dangerous but rather that all drugs can be dangerous, particularly if
they are used regularly over long periods of time. Psychoactive drugs create negative
effects not so much through their initial use but through the continued and increased use
that ultimately may lead to drug abuse.
The problem is that many drugs create tolerance, or an increase in the dose required to produce the same effect. The
consequence of tolerance is that the user must increase the dosage and/or the number of
times per day the drug is taken. As the use of the drug increases, the user may develop a
dependence, a need to use a drug or other
substance regularly. Dependence can be psychological, in which the drug is desired
and has become part of the everyday life without the serious physical effects if the drug
is not obtained; or physical, in which serious physical and mental effects appear when the
drug is withdrawn. Cigarette smokers who try to quit, for example, experience physical
withdrawal symptoms, such as becoming tired and irritable. In addition, smokers experience
psychological cravings to enjoy a cigarette in particular situations, such as after a meal
or when they are with friends.
Users may wish to stop using the drug, but when they reduce their dosage, they experience
withdrawal, or negative experiences that
accompany reducing or stopping drug use, including physical pain and other
symptoms. When the user powerfully craves the drug and is driven to
repeatedly seek it out, with potentially high physical, social, financial, and/or legal
cost, we say that he or she has developed an addiction to the
drug.
It is a common belief that addiction is an overwhelming, irresistibly powerful force and
that withdrawal from drugs is always an unbearably painful experience. But the reality is
more complicated and in many cases less extreme. For one, even drugs that we do not
generally think of as being addictive, such as caffeine, can be very difficult to quit for
some people. On the other hand, drugs that are normally associated with addiction,
including amphetamines, cocaine, and heroin, do not immediately create addiction in their
users. Even for a highly addictive drug like cocaine, only about 15% of users become
addicted. [1] [2]
Furthermore, the rate of addiction is lower for those who are taking drugs for medical
reasons than for those who are using drugs recreationally. Patients who have become
physically dependent on morphine administered during the course of medical treatment for
pain or a disease are able to be rapidly weaned off the drug afterward, without future
addiction. Robins, Davis, and Goodwin [3] found
that the majority of soldiers who had become addicted to morphine while overseas were
quickly able to stop using after returning home.
This does not mean that using recreational drugs is not dangerous. For people who do become
addicted to drugs, the success rate of recovery is low. Recreational drugs are generally
illegal and carry with them potential criminal consequences if a person is caught and
arrested. The way drugs and other substances are taken can also negatively impact the
user's health.
Furthermore, the quality and contents of illegal drugs are generally unknown,
and the doses can vary substantially from purchase to purchase.
Another problem is the unintended consequences of combining drugs, which can
produce serious side effects. Combining drugs is dangerous because their
combined effects on the CNS can increase dramatically and can lead to
accidental or even deliberate overdoses. For instance, ingesting alcohol or
benzodiazepines along with the usual dose of heroin is a frequent cause of
overdose deaths in opiate addicts. Furthermore, combining alcohol and cocaine
can have a dangerous impact on the cardiovascular system. [4]
Although all recreational drugs are dangerous, some can be more deadly than others. One way
to determine how dangerous recreational drugs are is to calculate a safety ratio. A safety ratio is calculated on the basis of the dose
that is likely to be fatal divided by the normal dose needed to feel the effects of the
drug. Drugs with lower ratios are more dangerous because the difference between the normal and
the lethal dose is small. For instance, heroin has a safety ratio of 6 because the
average fatal dose is only six times greater than the average effective dose. Marijuana has
a safety ratio of 1,000. This is not to say that smoking marijuana cannot be deadly, but it
is much less likely than heroin to be deadly. The safety ratios of common recreational
drugs are shown in the following table.
| Popular Recreational Drugs and Their Safety Ratios |
|---|
| Drugs with lower safety ratios have a greater risk of brain damage and death. From Flat World Knowledge, Introduction to Psychology. Source: Gable, R. (2004). Comparison of acute lethal toxicity of commonly abused psychoactive substances. Addiction 99(6):686–696. CC-BY-NC-SA. |
| Drug |
Description |
Street or Brand Names |
Safety Ratio |
| Heroin |
Strong depressant |
Smack, junk, H |
6 |
| GHB (gamma hydroxy butyrate) |
“Rave” drug (not Ecstacy), also used as a “date rape” drug |
Georgia home boy, liquid Ecstasy, liquid X, liquid G, fantasy |
8 |
| Isobutyl nitrite |
Depressant and toxic inhalant |
Poppers, rush, locker room |
8 |
| Alcohol |
Active compound is ethanol |
|
10 |
| DXM (dextromethorphan) |
Active ingredient in over-the-counter cold and cough medicines |
|
10 |
| Methamphetamine |
May be injected or smoked |
Meth, crank |
10 |
| Cocaine |
May be inhaled or smoked |
Crack, coke, rock, blue |
15 |
| MDMA (methylene dioxymetham phetamine) |
Very powerful stimulant |
Ecstasy |
16 |
| Codeine |
Depressant |
|
20 |
| Methadone |
Opioid |
|
20 |
| Mescaline |
Hallucinogen |
|
24 |
| Benzodiazepine |
Prescription tranquilizer |
Centrax, Dalmane, Doral, Halcion, Librium, ProSom, Restoril, Xanax,
Valium |
30 |
| Ketamine |
Prescription anesthetic |
Ketanest, Ketaset, Ketalar |
40 |
| DMT (dimethyl tryptamine) |
Hallucinogen |
|
50 |
| Phenobarbital |
Usually prescribed as a sleeping pill |
Luminal (phenobarbital), Mebaraland, Nembutal, Seconal, Sombulex |
50 |
| Prozac |
Antidepressant |
|
100 |
| Nitrous oxide |
Often inhaled from whipped cream dispensers |
Laughing gas |
150 |
| Lysergic acid diethylamide (LSD) |
|
Acid |
1,000 |
| Marijuana (Cannabis) |
Active ingredient is THC |
Pot, spliff, weed |
1,000 |
|
References
- Robinson, T. E., and Berridge, K. C.
(2003).
"Addiction." Annual Review of Psychology. Volume 54. Number 1. 25–53 Pages.
- Wagner, F. A., and Anthony, J. C.
(2002).
"From first drug use to drug dependence: Developmental periods of
risk for dependence upon marijuana, cocaine, and alcohol."
Neuropsychopharmacology. Volume 26. Number 4. 479–488 Pages.
- Robins, L. N., Davis, D. H., and Goodwin, D.
W.
(1974).
"Drug use by U.S. Army enlisted men in Vietnam: A follow-up on
their return home." American Journal of Epidemiology. Volume 99. Number
4. 235–249 Pages.
- McCance-Katz, E., Kosten, T., and
Jatlow, P.
(1988).
"Concurrent use of cocaine and alcohol is more potent and
potentially more toxic than use of either alone—A multiple-dose study
1." Biological Psychiatry. Volume 44. Number 4. 250–259 Pages.
A stimulant is a psychoactive drug that operates by blocking the
reuptake of dopamine, norepinephrine, and serotonin in the synapses of the CNS. By blocking reuptake of the neurotransmitter into the presynaptic cell,
the neurotransmitter stays in the synapse longer. Because more of these
neurotransmitters remain active in the brain, the result is an increase in the activity of
the sympathetic division of the autonomic nervous system (ANS). Effects of stimulants
include increased heart and breathing rates, pupil dilation, and increases in blood sugar
accompanied by decreases in appetite. For these reasons, stimulants are frequently used to
help people stay awake and to control weight.
Used in moderation, some stimulants may increase alertness, but used in an irresponsible
fashion, they can quickly create dependency. A major problem is the “crash” that results
when the drug loses its effectiveness and the activity of the neurotransmitters returns to
normal. The withdrawal from stimulants can create profound depression and lead to an
intense desire to repeat the high.
Caffeine
Caffeine is a bitter psychoactive drug found in the
beans, leaves, and fruits of plants, where it acts as a natural
pesticide. Caffeine acts as a mood enhancer and provides energy.
Although the U.S. Food and Drug Administration lists caffeine as a safe food
substance, it has at least some characteristics of dependence. People who reduce
their caffeine intake often report being irritable, restless, and drowsy. They can
also experience strong headaches, and these withdrawal symptoms may last up to a
week. Most experts feel that using small amounts of caffeine during pregnancy is
safe, but larger amounts of caffeine can be harmful to the
fetus. [1]
Nicotine
Nicotine is a psychoactive drug found in the
nightshade family of plants, where it acts as a natural
pesticide. Nicotine is the main cause for the dependence-forming
properties of tobacco use, and tobacco use is a major health threat.
Nicotine creates both psychological and physical addiction, and it is one
of the hardest addictions to break. Nicotine content in cigarettes has
slowly increased over the years, making quitting smoking more and more
difficult. Nicotine is also found in smokeless (chewing) tobacco.
People who want to quit smoking sometimes use other drugs to help them. For instance,
the prescription drug Chantix acts as an antagonist, binding to nicotine receptors in
the synapse, which prevents users from receiving the normal stimulant effect when
they smoke. At the same time, the drug releases dopamine, the reward
neurotransmitter. In this way, Chantix dampens nicotine withdrawal symptoms and
cravings. In many cases, people are able to get past the physical dependence,
allowing them to quit smoking at least temporarily. In the long run, however, the
psychological enjoyment of smoking may lead to relapse.
Cocaine
Cocaine is an addictive drug obtained from the leaves of the coca
plant. In the late 19th and early 20th centuries, it was a primary
constituent in many popular tonics and elixirs, and although it was removed in 1905,
it was one of the original ingredients in Coca-Cola. Today cocaine is taken illegally
as recreational drug.
Cocaine has a variety of adverse effects on the body. It constricts blood vessels,
dilates pupils, and increases body temperature, heart rate, and blood pressure. It
can cause headaches, abdominal pain, and nausea. Since cocaine also tends to decrease
appetite, chronic users may become malnourished. The intensity and duration of
cocaine’s effects, which include increased energy and reduced fatigue, depend on how
the drug is taken. The faster the drug is absorbed into the bloodstream and delivered
to the brain, the more intense the high. Injecting or smoking cocaine produces a
faster, stronger high than snorting it. However, the faster the drug is absorbed, the
faster the effects subside. The high from snorting cocaine may last 30 minutes,
whereas the high from smoking “crack” cocaine may last only 10 minutes. In order to
sustain the high, the user must administer the drug again, which may lead to frequent
use, often in higher doses, over a short period of
time. [2] Cocaine has a safety ratio of
15, making it a very dangerous recreational drug.
Amphetamine
Amphetamine is a stimulant that produces increased wakefulness and
focus along with decreased fatigue and appetite. Amphetamine is used in
prescription medications to treat attention deficit hyperactivity disorder (ADHD) and
narcolepsy and to control appetite. Some brand names of amphetamines are Adderall,
Benzedrine, Dexedrine, and Vyvanse. But amphetamines are also used illegally as a
recreational drug (“speed”). The methylated version of amphetamine, methamphetamine (“meth” or “crank”), is currently favored by
users, partly because it is available in ampoules ready for use by
injection. [3] Meth is a highly dangerous drug with a
safety ratio of only 10.
Amphetamines may produce a very high level of tolerance, leading users to increase
their intake, often in “jolts” taken every half hour or so. Although the level of
physical dependency is small, amphetamines may produce very strong psychological
dependence, effectively amounting to addiction. Continued use of stimulants may
result in severe psychological depression. The effects of the stimulant
methylenedioxymethamphetamine (MDMA), also known as Ecstasy, provide a good example.
MDMA is a strong stimulant that very successfully prevents the reuptake of serotonin,
dopamine, and norepinephrine. It is so effective that, when used repeatedly, it can
seriously deplete the amount of neurotransmitters available in the brain, producing a
catastrophic mental and physical “crash” resulting in serious, long-lasting
depression. MDMA also affects the temperature-regulating mechanisms of the brain, so
in high doses, and especially when combined with vigorous physical activity like
dancing, it can cause the body to become so drastically overheated that users can
literally “burn up” and die from hyperthermia and dehydration.
References
- U.S. Food and Drug Administration.
(2007).
Medicines in my home: Caffeine and your body.
Retrieved from
http://www.fda.gov/downloads/Drugs/ResourcesForYou/Consumers/BuyingUsingMedicineSafely/UnderstandingOver-the-CounterMedicines/UCM205286.pdf.
- National Institute on Drug Abuse.
(2009).
Cocaine abuse and addiction. Retrieved from http://www.nida.nih.gov/researchreports/cocaine/cocaine.html.
- Csaky, T. Z., and Barnes, B. A.
(1984).
Cutting’s Handbook of Pharmacology. Appleton-Century-Crofts. East Norwalk, CT. Edition 7.
In contrast to stimulants, which work to increase neural activity, a depressant acts to slow down consciousness. A depressant is a
psychoactive drug that reduces the activity of the CNS. Depressants are widely used
as prescription medicines to relieve pain, to lower heart rate and respiration, and as
anticonvulsants. Depressants change consciousness by increasing the production of the
neurotransmitter GABA and decreasing the production of the neurotransmitter acetylcholine,
usually at the level of the thalamus and the reticular formation. The outcome of depressant
use (similar to the effects of sleep) is a reduction in the transmission of impulses from
the lower brain to the cortex. [1]
Alcohol
The most common depressant is alcohol, a colorless liquid produced
by the fermentation of sugar or starch, which is the intoxicating agent in
fermented drinks. Alcohol is the oldest and most widely used drug of abuse in
the world. Note that alcohol is not a “safe” drug by any means—its safety ratio is
only 10.
Alcohol consumption is measured in blood alcohol concentration (BAC). Different
concentrations of alcohol in the human body can have different effects on the
individual. However, note that the effects of alcohol on any given individual can
also vary greatly depending on things like hydration and tolerance. Therefore, the
blood alcohol concentrations given in the activity below are just estimates used for
illustrative purposes.
Alcohol use is of high cost to societies because so many people abuse
alcohol and because judgment after drinking can be substantially
impaired. It is estimated that almost half of automobile fatalities are
caused by alcohol use, and excessive alcohol consumption is involved in a
majority of violent crimes, including rape and
murder. [2]
Alcohol increases the likelihood that people will respond aggressively to
provocations. [3] [4] [5]
Even people who are not normally aggressive may react with aggression
when they are intoxicated. Alcohol use also leads to rioting, unprotected
sex, and other negative outcomes.
Alcohol increases aggression in part because it reduces the ability of the person who
has consumed it to inhibit his or her
aggression. [6]
When people are intoxicated, they become more self-focused and less aware of the
social situation. As a result, they become less likely to notice the social
constraints that normally prevent them from engaging aggressively, and they are less
likely to use those social constraints to guide them. For instance, we might normally
notice the presence of a police officer or other people around us, which would remind
us that being aggressive is not appropriate. But when we are drunk, we are less
likely to be so aware. The narrowing of attention that occurs when we are intoxicated
also prevents us from anticipating the negative outcomes of our aggression. When we
are sober, we realize that being aggressive may produce a host of problems, but we
are less likely to realize these potential consequences when we have been
drinking. [7]
Alcohol also influences aggression through expectations. In other words, if we expect
that alcohol will make us more aggressive, then we tend to become more aggressive
when we drink.
Barbiturates
Barbiturates are depressants that are commonly prescribed as
sleeping pills and painkillers due to their ability to cause a wide range of
effects from mild sedation to total anesthesia. Brand names include Luminal
(phenobarbital), Mebaraland, Nembutal, Seconal, and Sombulex. In small to moderate
doses, barbiturates produce relaxation and sleepiness, but in higher doses, symptoms
may include sluggishness, difficulty in thinking, slowness of speech, drowsiness,
faulty judgment, and eventually coma or even death. [8] Barbiturates have been used as recreational drugs
because in low doses they can produce effects similar to alcohol (e.g., dizziness,
poor concentration, impaired judgement). However, individuals who use barbiturates
may also exhibit fatigue and irritability, and barbiturate use can lead to drug
dependence, tolerance, and respiratory depression (which can lead to death).
Barbiturates have now been largely replaced by a different class of depressants,
benzodiazepines. These drugs have less potential for lethal overdose. Today
barbiturates are more commonly used in general anesthesia and treatments for
epilepsy.
Thiopental (sodium amytal or sodium pentothal), a barbiturate, is often mistakenly
called a truth serum. Proponents of this idea claimed that individuals who take the
drug before an interview or questioning are more likely to provide the truth while
under its influence. In reality, this drug cannot and does not force anyone to tell
the truth. It is possible that the drug may appear to have this effect due to its
ability to decrease the inhibitions of the individual being questioned, but the same
could be said about other barbiturates and other types of depressant drugs.
Benzodiazepines
Related to barbiturates, benzodiazepines are a family
of depressants used to treat anxiety, insomnia, seizures, and muscle
spasms. In low doses, they produce mild sedation and relieve
anxiety; in high doses, they induce sleep. For these reasons, they are
commonly used to treat anxiety and insomnia. Benzodiazepines are also
used to treat epilepsy and alcohol withdrawal. In the United States,
benzodiazepines are among the most widely prescribed medications that
affect the CNS. Brand names include Centrax, Dalmane, Doral, Halcion,
Librium, ProSom, Restoril, Xanax, and Valium.
It is possible to overdose on benzodiazepines, but they are much less toxic than
their predecessors (barbiturates), and death rarely occurs when they are taken alone.
However, when taken in combination with other drugs, the potential for overdose and
complications increases. The lack of coordination, drowsiness, and dizziness that are
side effects of benzodiazepines tend to increase their danger. This is particularly
true for the elderly, in whom these side effects can result in falls and other
injuries. These side effects also make it more likely for an individual to be
involved in a (potentially fatal) car accident.
Toxic Inhalants
Toxic inhalants is a broad term used to describe recreation
drugs that are inhaled to create a change in consciousness. These drugs are easily
accessible as the vapors of glue, gasoline, propane, hair spray, and spray paint.
Inhalants are some of the most dangerous recreational drugs, with a safety index
below 10, and their continued use may lead to permanent brain damage. Users typically
inhale the vapors or the aerosol using plastic bags or open containers or by
breathing through solvent-soaked material. This behavior is sometimes called
“huffing.” The effects of toxic inhalants can vary widely from alcohol-like
intoxication to euphoria or hallucinations depending on the substance used and the
dose taken.
Related drugs are the nitrites (amyl and butyl nitrite; “poppers,”
“rush,” “locker room”) and anesthetics such as nitrous oxide (laughing
gas) and ether.
References
- Csaky, T. Z., and Barnes, B. A.
(1984).
Cutting’s Handbook of Pharmacology. Appleton-Century-Crofts. East Norwalk, CT. Edition 7.
- Abbey, A., Ross, L. T., McDuffie, D., and
McAuslan, P.
(1996).
"Alcohol and dating risk factors for sexual assault among college
women." Psychology of Women Quarterly. Volume 20. Number 1. 147–169
Pages.
- Bushman, B. J.
(1993).
"Human aggression while under the influence of alcohol and other
drugs: An integrative research review." Current Directions in
Psychological Science. Volume 2. Number 5. 148–152 Pages.
- Bushman, B. J. (Ed.).
(1997).
Effects of Alcohol on Human Aggression: Validity of Proposed Explanations. Plenum Press. New York.
- Graham, K., Osgood, D. W., Wells, S., and
Stockwell, T.
(2006).
"To what extent is intoxication associated with aggression in bars?
A multilevel analysis." Journal of Studies on Alcohol. Volume 67.
Number 3. 382–390 Pages.
- Steele, C. M., and Southwick, L.
(1985).
"Alcohol and social behavior: I. The psychology of drunken excess."
Journal of Personality and Social Psychology. Volume 48. Number 1.
18–34 Pages.
- Bushman, B. J., and Cooper, H. M.
(1990).
"Effects of alcohol on human aggression: An integrative research
review." Psychological Bulletin. Volume 107. Number 3. 341–354 Pages.
- Medline Plus.
(2008).
Barbiturate intoxication and overdose. Retrieved from http://www.nlm.nih.gov/medlineplus/ency/article/000951.htm.
Opioids are chemicals that increase activity in opioid
receptor neurons in the brain and in the digestive system, producing
euphoria, analgesia, slower breathing, and constipation. Their chemical
makeup is similar to the endorphins, the neurotransmitters that serve as the
body’s “natural pain reducers.” Natural opioids are derived from the opium
poppy, which is widespread in Eurasia, but they can also be created
synthetically.
The opioids activate the sympathetic division of the ANS, causing blood
pressure and heart rate to increase, often to dangerous levels that can lead to
heart attack or stroke. At the same time the drugs also influence the
parasympathetic division, leading to constipation and other negative side
effects. Symptoms of opioid withdrawal include diarrhea, insomnia,
restlessness, irritability, and vomiting, all accompanied by a strong craving
for the drug.
The powerful psychological dependence of the opioids and the severe effects of
withdrawal make it very difficult for opioid abusers to quit using. In
addition, because many users take these drugs intravenously and share
contaminated needles, they run a very high risk of being infected with
diseases. Opioid addicts suffer a high rate of infections such as HIV,
pericarditis (an infection of the membrane around the heart), and hepatitis B,
any of which can be fatal.
Opium
Opium is the dried juice of the unripe seed capsule of the opium
poppy. It may be the oldest drug on record, known to the Sumerians before
4000 BC. It was originally used in religious rituals and has been used as an
analgesic in early as well as modern cultures. Opium was made popular during the
opium trade in the 17th century, when it was brought from China to the rest of the
world by the British. It was prohibited by many countries by the beginning of the
20th century.
Morphine and Heroin
Morphine and heroin are stronger, more addictive drugs derived
from opium, while codeine is a weaker analgesic and less
addictive member of the opiate family. Opioids are often abused due to the
effects that they produce, which include a “body high” as well as intense feelings of
euphoria and relaxation. However, these drugs can be extremely dangerous in part due
to the extremely addictive nature of opioids. When morphine was first refined from
opium in the early 19th century, it was touted as a cure for opium addiction, but it
did not take long to discover that it was actually more addicting than raw opium.
When heroin was produced a few decades later, it was also initially thought to be a
more potent, less addictive painkiller but was soon found to be much more addictive
than morphine. Today, morphine is still used in hospitals as a painkiller to reduce
severe pain, but it is given in a limited fashion due to its high potential for
addiction and psychological dependence. Other synthetic opioids, such as oxycodone,
are more typically prescribed in cases of severe pain because they have fewer side
effects. Heroin is about twice as addictive as morphine and creates severe tolerance,
moderate physical dependence, and severe psychological dependence. Because of this,
it is considered to be one of the most dangerous street drugs. The danger of heroin
is demonstrated in the fact that it has the lowest safety ratio (6) of all the drugs
(see the table “Popular Recreational Drugs and Their Safety
Ratios”).
The drugs that produce the most extreme alteration of consciousness are the
hallucinogens, psychoactive drugs that alter sensation and
perception and that may create hallucinations. The hallucinogens are
frequently known as “psychedelics.”
Drugs in this class include lysergic acid diethylamide (LSD, or “acid”), mescaline, and
phencyclidine (PCP), as well as a number of natural plants including cannabis (marijuana),
peyote, and psilocybin (shrooms). The chemical compositions of the hallucinogens are
similar to the neurotransmitters serotonin and epinephrine, and they act primarily as
agonists by mimicking the action of serotonin at the synapses. The hallucinogens may
produce striking changes in perception through one or more of the senses. The precise
effects a user experiences are a function not only of the drug itself but also of the
user’s preexisting mental state and expectations of the drug experience. In other words,
the user tends to extract what he or she brings to the
experience. The hallucinations that may be experienced when taking these drugs are
strikingly different from everyday experience and frequently are more similar to dreams
than to everyday consciousness.
Although the hallucinogens are powerful drugs that produce striking
“mind-altering” effects, they do not produce physiological or psychological
tolerance or dependence. While they are not addictive and pose little physical
threat to the body, their use is not advisable in any situation in which the
user needs to be alert and attentive, exercise focused awareness or good
judgment, or demonstrate normal mental functioning, such as driving a car,
studying, or operating machinery.
Marijuana
Cannabis (marijuana) is the most widely used hallucinogen and is
used for recreational and medicinal purposes. Until it was banned in the
United States under the Marijuana Tax Act of 1938, it was widely used for medical
purposes. In recent years, cannabis has been prescribed for the treatment of pain and
nausea, particularly in cancer sufferers, as well as for a wide variety of other
physical and psychological disorders. [1] Although medical marijuana is now legal in several
American states, it is still banned under federal law, putting those states in
conflict with the federal government. Marijuana also acts as a stimulant, producing
giggling, laughing, and mild intoxication. It acts to enhance perception of sights,
sounds, and smells and may produce a sensation of time slowing down. It is much less
likely to lead to antisocial acts than is the other popular intoxicant, alcohol, and
it is also the one psychedelic drug whose use has not declined in recent years. [2]
Lysergic Acid Diethylamide (LSD or Acid)
LSD is a psychedelic drug that is known for its psychological side
effects, which include altered thinking processes, altered sensory experiences,
and an altered sense of time. However, the effects of LSD can vary widely
from person to person depending on factors such as dosage, previous experiences,
current state of mind, and the environment. Although it was initially used as a
therapeutic agent, LSD became popular as a recreational drug in 1960s youth
counterculture, which later resulted in its prohibition. LSD is not addictive and has
a very low toxicity relative to dosage. However, adverse psychiatric reactions such
as anxiety or delusions have been known to occur. LSD is typically taken orally,
usually on an absorbent substrate such as a sugar cube or paper.
Psilocybin
Psilocybin is a naturally occurring compound found in a number of mushroom species.
Effects can include euphoria, visual hallucinations, changes in perception, and a
distorted sense of time. As with other hallucinogens, the effects of psilocybin are
highly variable and depend on the mindset of the individual and the environment that
he or she is in. Psilocybin has low toxicity and does not cause dependence, but it
does have negative side effects such as nausea, disorientation, confusion, and panic
attacks. Negative incidents involving psilocybin typically involve the simultaneous
use of other drugs, including alcohol.
References
- Ben Amar, M.
(2006).
"Cannabinoids in medicine: A review of their therapeutic
potential." Journal of Ethnopharmacology. Volume 105. Number 1–2. 1–25
Pages.
- National Institute on Drug Abuse.
(2009).
NIDA InfoFacts: High school and youth trends. Retrieved from http://www.drugabuse.gov/infofacts/HSYouthTrends.html.
People have used, and often abused, psychoactive drugs for thousands of years.
Perhaps this should not be surprising, because many people find using drugs to
be fun and enjoyable. Even when we know the potential costs of using drugs, we
may engage in them anyway because the pleasures of using the drugs are
occurring right now, whereas the potential costs are abstract and occur in the
future.
Research Focus: Risk Tolerance Predicts Cigarette Use
Because drug and alcohol abuse is a behavior that has such important
negative consequences for so many people, researchers have tried to
understand what leads people to use drugs.
Researchers [1]
tested the hypothesis that cigarette smoking was related to a desire to
take risks. The study compared risk-taking behavior in adolescents who
reported having tried a cigarette at least once with those who reported
that they had never tried smoking.
Participants in the research were 125 5th- through 12th-graders attending
after-school programs throughout inner-city neighborhoods in the
Washington, DC, metropolitan area. Eighty percent of the adolescents
indicated that they had never tried even a puff of a cigarette, and 20%
indicated that they had had at least one puff of a cigarette.
The participants were tested in a laboratory where they completed the
Balloon Analogue Risk Task (BART), a measure of risk
taking. [2]
The BART is a computer task in which the participant pumps up a series of
simulated balloons by pressing on a computer key. With each pump the
balloon appears bigger on the screen, and more money accumulates in a
temporary “bank account.” However, when a balloon is pumped up too far,
the computer generates a popping sound, the balloon disappears from the
screen, and all the money in the temporary bank is lost. At any point
during each balloon trial, the participant can stop pumping up the
balloon, click on a button, transfer all money from the temporary bank to
the permanent bank, and begin with a new balloon.
Because the participants do not have precise information about the
probability of each balloon exploding, and because each balloon is
programmed to explode after a different number of pumps, the participants
have to determine how much to pump up the balloon. The number of pumps
that participants take is used as a measure of their tolerance for risk.
Low-tolerance people tend to make a few pumps and then collect the money,
whereas more risky people pump more times into each balloon.
Supporting the hypothesis that risk tolerance is related to smoking,
Lejuez et al. [1] found that the tendency to take risks was
indeed correlated with cigarette use: The participants who indicated that
they had puffed on a cigarette had significantly higher risk-taking
scores on the BART than did those who had never tried smoking.
Individual ambitions, expectations, and values also influence drug use. Vaughan,
Corbin, and Fromme [3] found that college
students who expressed positive academic values and strong ambitions had less alcohol
consumption and alcohol-related problems, and cigarette smoking has declined more
among youth from wealthier and more educated homes than among those from lower
socioeconomic backgrounds. [4]
Drug use is in part the result of socialization. Children try drugs when their
friends convince them to do it, and these decisions are based on social norms about
the risks and benefits of various drugs. In the period 1991 to 1997, the percentage
of 12th-graders who responded that they perceived “great harm in regular marijuana
use” declined from 79% to 58%, while annual use of marijuana in this group rose from
24% to 39%. [4] And students
binge drink in part when they see that other people around them are also
binging. [5]
All recreational drug use is associated with at
least some risks. Young people have experimented with cigarettes,
alcohol, and other dangerous drugs for many generations, and those who begin using drugs early are more
likely to use more dangerous drugs later. [6]
References
- Lejuez, C. W., Aklin, W. M., Bornovalova, M. A.,
and Moolchan, E. T.
(2005).
"Differences in risk-taking propensity across inner-city adolescent
ever- and never-smokers." Nicotine and Tobacco Research. Volume 7.
Number 1. 71–79 Pages.
- Lejuez, C. W., Read, J. P., Kahler, C. W.,
Richards, J. B., Ramsey, S. E., Stuart, G. L., et al.
(2002).
"Evaluation of a behavioral measure of risk taking: The Balloon
Analogue Risk Task (BART)." Journal of Experimental Psychology: Applied.
Volume 8. Number 2. 75–85 Pages.
- Vaughan, E. L., Corbin, W. R., and Fromme,
K.
(2009).
"Academic and social motives and drinking behavior." Psychology of
Addictive Behaviors. Volume 23. Number 4. 564–576 Pages.
- Johnston, L. D., O’Malley, P. M., Bachman, J. G., and Schulenberg, J. E.
(2004).
Monitoring the Future: National Results on Adolescent Drug Use.
Institute for Social Research, University of Michigan. Ann Arbor, MI.
(Conducted for the National Institute on Drug Abuse, National Institute
of Health).
- Clapp, J., Reed, M., Holmes, M., Lange, J.,
and Voas, R.
(2006).
"Drunk in public, drunk in private: The relationship between
college students, drinking environments and alcohol consumption."
American Journal of Drug and Alcohol Abuse. Volume 32. Number 2. 275–285
Pages.
- Lynskey, M. T., Heath, A. C., Bucholz, K.
K., Slutske, W. S., Madden, P. A. F., Nelson, E. C., et al.
(2003).
"Escalation of drug use in early-onset cannabis users vs co-twin
controls." Journal of the American Medical Association. Volume 289.
Number 4. 427–433 Pages.
The development of this CC-OLI Introduction to Psychology course and
its ongoing improvement is a collaborative effort involving many individuals whose
expertise, time, and dedication to this course we wish to recognize.
|
|---|
| Course Authors |
Affiliation |
| Keith Bujak |
Georgia Institute of Technology |
| Pat Carroll (Lead Content Author) |
University of Texas at Austin |
| Jack Chuang |
Highline Community College |
| Michael Considine |
Clinical Psychologist |
| Chelsea Cornelius |
University of Texas at Austin |
| Chris De La Ronde |
Austin Community College |
| Igor Dolgov |
New Mexico State University |
| Jennifer Eno Louden |
University of Texas at El Paso |
| Amber Gilewski |
Tompkins Cortland Community College |
| Nancy Gup |
Georgia Perimeter College |
| Pamela Hill |
San Antonio Community College |
| Sachi Horback |
Colby-Sawyer College |
| Jerry Marshall |
Green River Community College |
| Larry Rudiger |
The University of Vermont |
| Brook Schepp |
University of Texas at Austin |
| Laura Selkirk |
The University of Vermont |
| Kat Snyder |
University of Texas at Austin |
| Deborah Stote |
Clinical Psychologist |
| Michael Vitevitch |
The University of Kansas |
| Anne Wiley |
Greenfield Community College |
| Other Contributors |
Affiliation |
| Norman Bier |
Carnegie Mellon University |
| Adam Ellis |
Miami University |
| Greg Goodhile |
Carnegie Mellon University |
| Kim Henry |
Carnegie Mellon University |
| Carol Lallier |
Carnegie Mellon University |
| Ross Strader |
Carnegie Mellon University (University of Texas at Austin) |
| Cheryl Templeton |
Carnegie Mellon University |
|






. Calkins made significant contributions to the study of memory and the self-concept. Mahzarin Banaji (upper left), Marilynn Brewer (upper right), and Linda Bartoshuk (lower left) all have been recent presidents of the American Psychological Association.")
 and Aristotle. Plato believed that much knowledge was innate, whereas Aristotle thought that each child was born as an “empty slate” and that knowledge was primarily acquired through learning and experience.")
 and Edward Titchener (right) helped create the structuralist school of psychology. Their goal was to classify the elements of sensation through introspection.")
, was influenced by the work of Charles Darwin.")



 and those living in Eastern cultures which value families and social groups (collectivism).")










 the assurance that the independent variable (also known as the experimental manipulation) occurs prior to the measured dependent variable, and (2) the creation of initial equivalence between the conditions of the experiment (in this case by using random assignment to conditions).")

. Confounding makes it impossible to be sure that the independent variable (rather than the confounding variable) caused the dependent variable.")









, each of which has four lobes (temporal, frontal, occipital, and parietal). Furthermore, there are specific cortical areas that control different processes.")





 and on the tasks the person is engaging in.")
 machine")


 and a Schizophrenic Brain")

 Equipment")






.")


 are accurate; the other two (misses and false alarms) are errors.")



 is detectable by the human eye.")

, the lens properly focuses incoming light on the retina. For people who are nearsighted (center), images from far objects focus too far in front of the retina, whereas for people who are farsighted (right), images from near objects focus too far behind the retina. Eyeglasses solve the problem by adding a secondary, corrective, lens.")





. However, people who are colorblind cannot see the numbers at all.")











 that transduce the rotational movements of the body and the vestibular sacs (blue) that sense linear accelerations.")




 naturally produces the unconditioned response (UR). Top right: Before conditioning, the neutral stimulus (the whistle) does not produce the salivation response. Bottom left: The unconditioned stimulus (US), in this case the food, is repeatedly presented immediately after the neutral stimulus. Bottom right: After learning, the neutral stimulus (now known as the conditioned stimulus or CS), is sufficient to produce the conditioned responses (CR).")
 represents a case of classical conditioning to a severe trauma that does not easily become extinct. In this case the original fear response, experienced during combat, has become conditioned to a loud noise. When the person with PTSD hears a loud noise, he or she experiences a fear response despite being far from the site of the original trauma.")



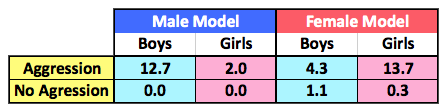





















 influenced other specific intelligences (s)")
")





































 Versus a Brain With Advanced Alzheimer’s Disease (Right)")






























 for the behaviors of others, even where situational factors such as poor education and growing up in poverty might be better explanations, is caused by the fundamental attribution error.")










 when the initial split was 3–3.")








 has been used since prehistoric times in attempts to cure epilepsy, schizophrenia, and other psychological disorders.")


.")

, personal writings, and behavior (including cutting off his own ear), it is commonly thought that van Gogh suffered from bipolar disorder. He committed suicide at age 37.")








 is based on the idea that our thoughts, feelings, and behavior reinforce each other and that changing our thoughts or behavior can make us feel better.")
")
")






 was a proponent of dualism, the theory that the mind and body are two separate entities. Psychologists reject this idea, however, believing that consciousness is a result of activity in the brain, not separate from it.")






